You might also like
- Clinical Decision Support System: Fundamentals and ApplicationsFrom EverandClinical Decision Support System: Fundamentals and ApplicationsNo ratings yet
- Quality of VigiBase Reports Vital for Patient SafetyDocument0 pagesQuality of VigiBase Reports Vital for Patient Safetysreeraj.guruvayoorNo ratings yet
- Umc Caveat September-2021Document1 pageUmc Caveat September-2021Aranaya WayaNo ratings yet
- Oms Lista de Exames Essenciais 2018Document35 pagesOms Lista de Exames Essenciais 2018João LuccasNo ratings yet
- Artigo - ImpactoMR - A Brazilian Nationwide Platform StudyDocument18 pagesArtigo - ImpactoMR - A Brazilian Nationwide Platform StudyMICHELLE SOUSANo ratings yet
- Ad Hoc Data SourcesDocument10 pagesAd Hoc Data SourcesgowthamNo ratings yet
- Eng PDFDocument80 pagesEng PDFDamicNo ratings yet
- Drug Misuse England 2018Document7 pagesDrug Misuse England 2018mikepeterpowerNo ratings yet
- EDL Executive SummaryDocument36 pagesEDL Executive SummaryJosé Esteban Guerrero DávilaNo ratings yet
- Whonet Documentation: Travancore Medical CollegeDocument20 pagesWhonet Documentation: Travancore Medical Collegetummalapalli venkateswara raoNo ratings yet
- Pharmaceutics 04 00607Document34 pagesPharmaceutics 04 00607محمد خليلNo ratings yet
- Real World Data and Data Science in Medical ResearDocument13 pagesReal World Data and Data Science in Medical Researhabeeb4saNo ratings yet
- Eng 2Document80 pagesEng 2Achmad ArrosyidiNo ratings yet
- Newsletters 13Document7 pagesNewsletters 13Peet UpNo ratings yet
- Cloud MRM-A Bio-IT Tool For Correlative Studies in Dermatology 30.08.2011Document11 pagesCloud MRM-A Bio-IT Tool For Correlative Studies in Dermatology 30.08.2011Aimoldina AlmaNo ratings yet
- The importance of real-world data to precision medicineDocument4 pagesThe importance of real-world data to precision medicineAngeline JebaNo ratings yet
- The Status Quo On Existing Routine Health InformatDocument15 pagesThe Status Quo On Existing Routine Health InformatJaweria KhanNo ratings yet
- IWGDF Guideline On The Classification of Diabetic Foot UlcersDocument15 pagesIWGDF Guideline On The Classification of Diabetic Foot Ulcersdr. Ellen FernandaNo ratings yet
- Whonet DocumentationDocument19 pagesWhonet DocumentationinvisibleyetinvincibleNo ratings yet
- Patient View European Health App DirectoryDocument231 pagesPatient View European Health App Directorysravan5341No ratings yet
- A Machine Learning-Based Clinical Decision Support System To Identify Prescriptions With A High Risk of Medication ErrorDocument7 pagesA Machine Learning-Based Clinical Decision Support System To Identify Prescriptions With A High Risk of Medication Errorafri pakalessyNo ratings yet
- Public Health Surveillance System Evaluation Project - Part3Team1Document17 pagesPublic Health Surveillance System Evaluation Project - Part3Team1dasarathramNo ratings yet
- 121217what Are in Vitro Diagnostic Tests, and How Are They Regulated?Document3 pages121217what Are in Vitro Diagnostic Tests, and How Are They Regulated?buvaeltyaeNo ratings yet
- Clinical Data RepositoriesDocument5 pagesClinical Data RepositoriesvivianschuylerNo ratings yet
- Common Datatypes in Healthcare, Workflow and ManagementDocument9 pagesCommon Datatypes in Healthcare, Workflow and ManagementKrishnanjali VuNo ratings yet
- Vaers Data Use Guide: 1. Important Information About VAERSDocument17 pagesVaers Data Use Guide: 1. Important Information About VAERSMalu HadassaNo ratings yet
- PSNC Model DPIADocument8 pagesPSNC Model DPIAmartin_vkNo ratings yet
- Popdx: An Automated Framework For Patient Phenotyping Across 392 246 Individuals in The Uk Biobank StudyDocument11 pagesPopdx: An Automated Framework For Patient Phenotyping Across 392 246 Individuals in The Uk Biobank StudysubaNo ratings yet
- Essential PV System RequirementsDocument2 pagesEssential PV System RequirementsKishoreNo ratings yet
- UNIT-5-CLINICAL-DATA-REPOSITORIES Public Health - RemovedDocument10 pagesUNIT-5-CLINICAL-DATA-REPOSITORIES Public Health - RemovedKelvin CafirmaNo ratings yet
- ScientificSummary Hta19570Document8 pagesScientificSummary Hta19570Anonymous hvOuCjNo ratings yet
- Alien TechnologyDocument11 pagesAlien TechnologySharvari TaklikarNo ratings yet
- Internet Tools For Advanced Nursing PracticeDocument39 pagesInternet Tools For Advanced Nursing PracticemalindaNo ratings yet
- NHSN OverviewDocument5 pagesNHSN OverviewhfarrukhnNo ratings yet
- WHO Guiding Principles For Pathogen Genome Data SharingDocument12 pagesWHO Guiding Principles For Pathogen Genome Data Sharingiq_dianaNo ratings yet
- 2-4 What Is A Safety SignalDocument4 pages2-4 What Is A Safety Signalx7w34TNo ratings yet
- Health InformaticsDocument10 pagesHealth Informaticsjose layaNo ratings yet
- Drug-Related Admissions and Hospital-Acquired Adverse Drug Events in Germany: A Longitudinal Analysis From 2003 To 2007 of ICD-10-coded Routine DataDocument9 pagesDrug-Related Admissions and Hospital-Acquired Adverse Drug Events in Germany: A Longitudinal Analysis From 2003 To 2007 of ICD-10-coded Routine DataYuli CartrinaNo ratings yet
- Production of ICD-11: The overall revision processDocument22 pagesProduction of ICD-11: The overall revision processdfriadyNo ratings yet
- 2009 Drug InformationDocument8 pages2009 Drug InformationAnggioppleNo ratings yet
- Mental Health & Substance Abuse Drug Abuse Monitoring SystemDocument29 pagesMental Health & Substance Abuse Drug Abuse Monitoring SystemRavi Gaura Das100% (1)
- Key Terms of EHRs and Examples in Various Types of Care SettingsDocument10 pagesKey Terms of EHRs and Examples in Various Types of Care SettingsDariaZhuravlevaNo ratings yet
- Health Information SystemsDocument7 pagesHealth Information SystemsCharlene Kaye DumanjugNo ratings yet
- UPPSALADocument10 pagesUPPSALASam PradhanNo ratings yet
- Unit - 3Document18 pagesUnit - 3Meharaj UnnisaNo ratings yet
- Issues in International Health Policy: Electronic Health Records: An International Perspective On "Meaningful Use"Document18 pagesIssues in International Health Policy: Electronic Health Records: An International Perspective On "Meaningful Use"Sevi Cephy ONo ratings yet
- PV in Developing Countries - CrispDocument4 pagesPV in Developing Countries - CrispVandana ReddyNo ratings yet
- DOH ICT SytemDocument19 pagesDOH ICT Sytemricohizon99No ratings yet
- Pdfs 8502 InTech-Rfid Based Information System For Patients and Medical Staff Identification and TrackingDocument15 pagesPdfs 8502 InTech-Rfid Based Information System For Patients and Medical Staff Identification and TrackingSankula Siva SankarNo ratings yet
- Computerized Medical Lab Record SystemDocument41 pagesComputerized Medical Lab Record SystemUmar Ridwan saniNo ratings yet
- Patient Information Systems in The LiteratureDocument6 pagesPatient Information Systems in The LiteratureJohn MunaonyediNo ratings yet
- The burden of antimicrobial resistance (AMR) in MalaysiaDocument4 pagesThe burden of antimicrobial resistance (AMR) in MalaysiaalbertNo ratings yet
- WHO Policy Development Processes For A New Vaccine: Case Study of Malaria VaccinesDocument11 pagesWHO Policy Development Processes For A New Vaccine: Case Study of Malaria VaccinesAndi Dirhan TNo ratings yet
- CCD Case StudyDocument5 pagesCCD Case StudyMeenalNo ratings yet
- The Open Data Platform - Improving Healthcare With AnalyticsDocument6 pagesThe Open Data Platform - Improving Healthcare With Analyticshuber.mcNo ratings yet
- ADEpedia 2.0-Integration of Normalized Adverse Drug Events (ADEs)Document23 pagesADEpedia 2.0-Integration of Normalized Adverse Drug Events (ADEs)AMIANo ratings yet
- BA PresentationDocument23 pagesBA PresentationRajpurohit Jigar SinghNo ratings yet
- JPS Ferranti Cognos SurveillanceDocument7 pagesJPS Ferranti Cognos SurveillancesamlenciNo ratings yet
- Unraveling The Potential of Real-World Studies (2017)Document4 pagesUnraveling The Potential of Real-World Studies (2017)Arturo Lopez GilNo ratings yet
- Thinkpad 11E and Thinkpad Yoga 11E Fru Bom, MT: 20da, 20D9: Fru Cru Id Description Ac AdapterDocument6 pagesThinkpad 11E and Thinkpad Yoga 11E Fru Bom, MT: 20da, 20D9: Fru Cru Id Description Ac AdapterAranaya WayaNo ratings yet
- Schematic diagram of main circuit with audio and voltage linesDocument1 pageSchematic diagram of main circuit with audio and voltage linesAranaya WayaNo ratings yet
- SonyvaioDocument4 pagesSonyvaioAranaya WayaNo ratings yet
- LG He LCD Ss 32LE5300-5Document2 pagesLG He LCD Ss 32LE5300-5Aranaya WayaNo ratings yet
- Specification FOR Approval: Title 11.6" FHD TFT LCDDocument30 pagesSpecification FOR Approval: Title 11.6" FHD TFT LCDAranaya WayaNo ratings yet
- Ehci Removal 6th Gen Core PCH Technical PaperDocument10 pagesEhci Removal 6th Gen Core PCH Technical PaperAranaya WayaNo ratings yet
- Tire Thread Machine Learning ModelDocument12 pagesTire Thread Machine Learning ModelMarcos CostaNo ratings yet
- CRD - c48 CRD-C48-92 Standard Test Method For Water Permeability of ConcreteDocument4 pagesCRD - c48 CRD-C48-92 Standard Test Method For Water Permeability of ConcreteazharbNo ratings yet
- Literacy Narrative Essay 1Document3 pagesLiteracy Narrative Essay 1api-644119616No ratings yet
- Q3876 Common Questions About ActiveX Controls in CitectSCADADocument5 pagesQ3876 Common Questions About ActiveX Controls in CitectSCADAdesrico20039088No ratings yet
- Myon Parent GuideDocument13 pagesMyon Parent Guideapi-527646442No ratings yet
- CDP Report FormatDocument2 pagesCDP Report FormatSajath SabryNo ratings yet
- Organizational Theory Quiz 1Document1 pageOrganizational Theory Quiz 1Shabana NaveedNo ratings yet
- DownloadDocument2 pagesDownloadapextelecomsaNo ratings yet
- 03-M-U-300000 List of Documents & Drawings For Cold Box-REV01Document5 pages03-M-U-300000 List of Documents & Drawings For Cold Box-REV01mahmoudNo ratings yet
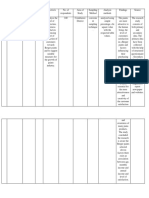
- Sample - Table - Literature ReviewDocument11 pagesSample - Table - Literature ReviewKeyur KevadiyaNo ratings yet
- "Experimental Investigation On The Use of Coconut Shell As Partial Replacement of Coarse Aggregate in Concrete'' Nikhil M. DofeDocument18 pages"Experimental Investigation On The Use of Coconut Shell As Partial Replacement of Coarse Aggregate in Concrete'' Nikhil M. DofeKomal mankarNo ratings yet
- Study On Electricity Distribution Substation Operation Amp Maintenance of DescoDocument46 pagesStudy On Electricity Distribution Substation Operation Amp Maintenance of DescoJayant KoshtiNo ratings yet
- 華語輔導系統使用說明 Mandarin Tutorial System GuidelineDocument11 pages華語輔導系統使用說明 Mandarin Tutorial System GuidelineAsnidar SiahaanNo ratings yet
- 2. CHUYÊN ĐỀ 2 (LỖI SAI + VIẾT CÂU)Document4 pages2. CHUYÊN ĐỀ 2 (LỖI SAI + VIẾT CÂU)farm 3 chi di0% (1)
- Aire Acondicionado Split Mural X Frig TK 10992786 TechsheetsupDocument1 pageAire Acondicionado Split Mural X Frig TK 10992786 TechsheetsupJOSE ANGEL VILLALOBOS JIMENEZNo ratings yet
- E-Mobility LD DIDACTICDocument12 pagesE-Mobility LD DIDACTICromauli100% (1)
- Redwan Ahmed Miazee - HW - 1Document3 pagesRedwan Ahmed Miazee - HW - 1REDWAN AHMED MIAZEENo ratings yet
- Hybrid Pile Foundations IPWE SeminarDocument22 pagesHybrid Pile Foundations IPWE Seminarrohit100% (1)
- Finlatics NotesDocument48 pagesFinlatics NotesShailesh TirkeyNo ratings yet
- SST Programming Guide for Gen4 SystemsDocument8 pagesSST Programming Guide for Gen4 SystemsdmaslachNo ratings yet
- HPA4 Service ManualDocument7 pagesHPA4 Service ManualMarcelo ArayaNo ratings yet
- PerpetuumSoft RSS Getting StartedDocument20 pagesPerpetuumSoft RSS Getting StartedEvqueni Yero RodríguezNo ratings yet
- NMTC 2017 (5th-6th-7th-8th-9th-10th) Answer Keys With Solution - AMANS MATHS BLOGSDocument41 pagesNMTC 2017 (5th-6th-7th-8th-9th-10th) Answer Keys With Solution - AMANS MATHS BLOGSanjuNo ratings yet
- Unit 25 Sound RecordingDocument21 pagesUnit 25 Sound Recordingapi-480389176No ratings yet
- JD Requirement College 25jun21Document2 pagesJD Requirement College 25jun21Will MNo ratings yet
- Check-Lists D'inspectionDocument43 pagesCheck-Lists D'inspectionElisee93% (29)
- Novent Microfluidics: Installation GuideDocument24 pagesNovent Microfluidics: Installation GuidetalebNo ratings yet
- ECE 271 MOS Memory and Storage Circuits TopicDocument98 pagesECE 271 MOS Memory and Storage Circuits TopicNiharikaNo ratings yet
- RULES and GUIDELINES Extempo and Poster Making ContestDocument4 pagesRULES and GUIDELINES Extempo and Poster Making ContestChrisa C. TabiliranNo ratings yet
- Computer Graphics: Unit - I O P: P LDocument42 pagesComputer Graphics: Unit - I O P: P LNileshIndulkarNo ratings yet