You might also like
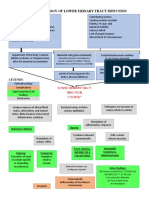
- Pathophysiology of Lower Urinary Tract InfectionDocument1 pagePathophysiology of Lower Urinary Tract InfectionSTORAGE FILENo ratings yet
- Pathophysiology of the urinary tractDocument8 pagesPathophysiology of the urinary tractMarjorie CarganillaNo ratings yet
- Pathophysiology of Acute PyelonephritisDocument2 pagesPathophysiology of Acute Pyelonephritisgodwinkent888No ratings yet
- Hydronephrosis Fred LuceDocument69 pagesHydronephrosis Fred LuceKMNo ratings yet
- Pre Eclampsia of Severe FeaturesDocument3 pagesPre Eclampsia of Severe FeaturesPrincess Diane S. VillegasNo ratings yet
- Pneumonia PathoDocument2 pagesPneumonia PathoDerick Nyl PascualNo ratings yet
- Patho DengueDocument3 pagesPatho DengueLindy Shane BoncalesNo ratings yet
- Pathophysiology of Chronic Glomerulonephritis: LegendDocument1 pagePathophysiology of Chronic Glomerulonephritis: LegendGeorich Narciso50% (4)
- Pathophysiology AppendicitisDocument3 pagesPathophysiology AppendicitisIra Krystel ReyesNo ratings yet
- Thromboangiitis Obliterans (Buerger's Disease): A Case PresentationDocument16 pagesThromboangiitis Obliterans (Buerger's Disease): A Case PresentationYan VencerNo ratings yet
- Pathophysiology of Hyperemesis Gravidarum DiagramDocument1 pagePathophysiology of Hyperemesis Gravidarum DiagramQuintin MangaoangNo ratings yet
- Case Presentation of Acute PyelonephritisDocument1 pageCase Presentation of Acute PyelonephritisANALYN ANUBNo ratings yet
- MYOMA PathoDocument1 pageMYOMA Pathobsn2011100% (1)
- N. Bacalso Ave., Cebu City Philippines: Page 1 of 32Document32 pagesN. Bacalso Ave., Cebu City Philippines: Page 1 of 32Joule PeirreNo ratings yet
- Case Study - Dengue Fever V - S UtiDocument12 pagesCase Study - Dengue Fever V - S UtiHarlene Joyce ReyNo ratings yet
- Pathophysiology (Client Base) :: Predisposing Factors: Precipitating FactorsDocument1 pagePathophysiology (Client Base) :: Predisposing Factors: Precipitating Factorsleslie_macasaetNo ratings yet
- AGE PathophysiologyDocument2 pagesAGE Pathophysiologyjosephcanlas67% (3)
- Pathophysiology of Pressure UlcersDocument1 pagePathophysiology of Pressure UlcersSTORAGE FILENo ratings yet
- Pa Tho Physiology of Open FractureDocument2 pagesPa Tho Physiology of Open FracturegiffersonbNo ratings yet
- Pa Tho Physiology of PyelonephritisDocument2 pagesPa Tho Physiology of PyelonephritisYuan Li100% (1)
- Etiology: Predisposing Factors: Precipitating FactorsDocument5 pagesEtiology: Predisposing Factors: Precipitating FactorsJanelle NarcisoNo ratings yet
- Pathophysiology of Acute Gastroenteritis: Causes, Symptoms & TreatmentDocument1 pagePathophysiology of Acute Gastroenteritis: Causes, Symptoms & TreatmentZhenmeiNo ratings yet
- Liver AbscessDocument3 pagesLiver AbscessStephanie Pe100% (1)
- PneumoniaDocument1 pagePneumoniaAyen FornollesNo ratings yet
- Bea-Case StudyDocument21 pagesBea-Case Studybea pegadNo ratings yet
- Abnormal Uterine BleedingDocument2 pagesAbnormal Uterine BleedingNatasha EnidNo ratings yet
- Pathophysiology Dengue Hemorrhagic FeverDocument1 pagePathophysiology Dengue Hemorrhagic FeverShiella Heart Malana100% (1)
- Patho Pott's DseDocument2 pagesPatho Pott's Dsexai_teovisioNo ratings yet
- Urinary Tract Infection Anatomy and PhysiologyDocument12 pagesUrinary Tract Infection Anatomy and PhysiologyPaul Anthony Centeno PimentelNo ratings yet
- SCHEMATIC DIAGRAM Obstructive JaundiceDocument1 pageSCHEMATIC DIAGRAM Obstructive JaundiceJan Niño EstrellaNo ratings yet
- BFCDocument8 pagesBFCIrene GunongNo ratings yet
- Pathophy NCADocument1 pagePathophy NCAKaren ValdezNo ratings yet
- Non-Modifiable Factor Modifiable Factor: South-East Asia, Eastern, Mediterranean, Western Pacific, and The AmericasDocument2 pagesNon-Modifiable Factor Modifiable Factor: South-East Asia, Eastern, Mediterranean, Western Pacific, and The Americaschristian quiaoitNo ratings yet
- Pathophysiology Cholelithiasis 2Document2 pagesPathophysiology Cholelithiasis 2Jamie HaravataNo ratings yet
- AmoebiasisDocument1 pageAmoebiasisYakumaNo ratings yet
- DiverticulitisDocument2 pagesDiverticulitisyapyapvinx50% (2)
- H MoleDocument2 pagesH MoleJoanna Marie Datahan EstomoNo ratings yet
- IntussusceptionDocument2 pagesIntussusceptionkentkriziaNo ratings yet
- Acute Gastroenteritis Case StudyDocument42 pagesAcute Gastroenteritis Case StudyGelah DacanayNo ratings yet
- Nursing Care Plan For Incarcerated Inguinal Hernia RightDocument2 pagesNursing Care Plan For Incarcerated Inguinal Hernia RightTrisha Lapid MatulaNo ratings yet
- Pathway - Urethral StrictureDocument1 pagePathway - Urethral StrictureCiptaningrum Marisa PNo ratings yet
- Chronic PyelonephritisDocument5 pagesChronic PyelonephritisIsak ShatikaNo ratings yet
- Pathophysiology of Congenital Heart Defects in BabiesDocument1 pagePathophysiology of Congenital Heart Defects in BabiesMarlon CruzNo ratings yet
- Hirschsprung Disease Case Study: Maecy P. Tarinay BSN 4-1Document5 pagesHirschsprung Disease Case Study: Maecy P. Tarinay BSN 4-1Maecy OdegaardNo ratings yet
- Assessment/ Cues Nursing Diagnosis Background Knowledge Goal and Objectives Nursing Interventions and Rationale EvaluationDocument6 pagesAssessment/ Cues Nursing Diagnosis Background Knowledge Goal and Objectives Nursing Interventions and Rationale EvaluationimnasNo ratings yet
- Tetanus PathoDocument3 pagesTetanus PathoElisha Gine AndalesNo ratings yet
- Osteoarthritis 1583-170210113823Document34 pagesOsteoarthritis 1583-170210113823Angelic khanNo ratings yet
- Pathophysiology of Urinary Tract ObstructionDocument50 pagesPathophysiology of Urinary Tract ObstructionPryo UtamaNo ratings yet
- Pathophysiology of Amoebiasis: Ingestion to ExcretionDocument1 pagePathophysiology of Amoebiasis: Ingestion to ExcretionCathy AcquiatanNo ratings yet
- Pcap PathoDocument2 pagesPcap PathoLardel CarayNo ratings yet
- Schistosomiasis (From Anatomy To Pathophysiology)Document10 pagesSchistosomiasis (From Anatomy To Pathophysiology)Tiger Knee100% (1)
- Amoebiasis PathophysiologyDocument3 pagesAmoebiasis PathophysiologyApril CornejoNo ratings yet
- Urinary Tract Infection pATho SHEENADocument2 pagesUrinary Tract Infection pATho SHEENASheena Arnoco ToraynoNo ratings yet
- Pathophysiology FinalDocument2 pagesPathophysiology FinallarissedeleonNo ratings yet
- Annotated Group 2 Impetigo Concept Mapping 1Document30 pagesAnnotated Group 2 Impetigo Concept Mapping 1DHANE ANN CAMPOSANONo ratings yet
- Reflection PaperDocument2 pagesReflection PapershanoiapowelllNo ratings yet
- Urinary Tract Infection in PregnancyDocument49 pagesUrinary Tract Infection in PregnancyBALMERA, DANIELLA B.No ratings yet
- Everything You Need to Know About Urinary Tract Infections (UTIsDocument10 pagesEverything You Need to Know About Urinary Tract Infections (UTIsMira Mariana UlfahNo ratings yet
- UTI PathophysiologyDocument1 pageUTI PathophysiologyNathaniel SupanNo ratings yet
- Predisposing Factors Primary Infection of Parenchyma: Lower Urinary Tract InfectionDocument1 pagePredisposing Factors Primary Infection of Parenchyma: Lower Urinary Tract InfectionstoragejoannamsvNo ratings yet
- Medication Administration RevDocument9 pagesMedication Administration RevIrish EspinosaNo ratings yet
- BagTechnique ReviewerDocument2 pagesBagTechnique ReviewerIrish EspinosaNo ratings yet
- Anaphy & Pathophy (Hyperemesis)Document6 pagesAnaphy & Pathophy (Hyperemesis)Irish EspinosaNo ratings yet
- Signs and Stages of PregnancyDocument4 pagesSigns and Stages of PregnancyIrish EspinosaNo ratings yet
- Anaphy & Pathophy (Hyperemesis)Document6 pagesAnaphy & Pathophy (Hyperemesis)Irish EspinosaNo ratings yet
- Book Based: Etiology: Tubercle Bacilli Precipitating Factors Predisposing FactorsDocument7 pagesBook Based: Etiology: Tubercle Bacilli Precipitating Factors Predisposing FactorsIrish EspinosaNo ratings yet
- Reviewerenema and Oxygen MarieDocument4 pagesReviewerenema and Oxygen MarieIrish EspinosaNo ratings yet
- Anaphy & Pathophy (Hyperemesis)Document6 pagesAnaphy & Pathophy (Hyperemesis)Irish EspinosaNo ratings yet
- Signs and Stages of PregnancyDocument4 pagesSigns and Stages of PregnancyIrish EspinosaNo ratings yet
- Unit 5 WB - Answer KeyDocument2 pagesUnit 5 WB - Answer KeyNgọc AnhNo ratings yet
- Microscope ReportDocument9 pagesMicroscope ReportYap StainleyNo ratings yet
- 2 - Yasemin Celebi - MicrofluidicsDocument7 pages2 - Yasemin Celebi - MicrofluidicsYasemin ÇelebiNo ratings yet
- 58 - 18015erdheim ChesterDocument5 pages58 - 18015erdheim ChesterGerman HaroNo ratings yet
- AIIMS May 2019 - PhysiologyDocument3 pagesAIIMS May 2019 - Physiologyshibira surendran vkNo ratings yet
- A-Level H2 Biology Topical 2004-2013 AnswersDocument82 pagesA-Level H2 Biology Topical 2004-2013 AnswersMuhammad Amin SuhaimiNo ratings yet
- Pathphysiology CurriculumDocument14 pagesPathphysiology Curriculumapi-3728690No ratings yet
- Earth Scie 22Document26 pagesEarth Scie 22HayaradjNo ratings yet
- Microbial Ecology and Microbial BiotechnologyDocument4 pagesMicrobial Ecology and Microbial BiotechnologynmdconahapNo ratings yet
- Biodegradable Polymers For Biomedical Additive ManufacturingDocument59 pagesBiodegradable Polymers For Biomedical Additive ManufacturingRafael Franco GontijoNo ratings yet
- Plant MovementDocument25 pagesPlant MovementMichael PradhanNo ratings yet
- ANTHROPOLOGYDocument29 pagesANTHROPOLOGYPrincess Ann BalongaNo ratings yet
- Biology of Tendon Injury: Healing, Modeling and Remodeling: P. Sharma and N. MaffulliDocument10 pagesBiology of Tendon Injury: Healing, Modeling and Remodeling: P. Sharma and N. MaffulliBrianna RyanNo ratings yet
- Cell Organelle Review Worksheet 14-15Document2 pagesCell Organelle Review Worksheet 14-15Kirsten Troupe100% (1)
- Kryon Attributes of AscensionDocument15 pagesKryon Attributes of AscensionMeaghan Mathews100% (2)
- HBG112 New Syllabus 2023-2024Document9 pagesHBG112 New Syllabus 2023-2024shahd elmaghraby (user206)No ratings yet
- Basic ChemistryDocument43 pagesBasic ChemistryKarim Wasi100% (6)
- The Typification and Status of Phymatolithon Corallinaceae RhodophytaDocument27 pagesThe Typification and Status of Phymatolithon Corallinaceae RhodophytaJamesNo ratings yet
- CSGO Matches & LivescoreDocument1 pageCSGO Matches & LivescoreВлад ГаманNo ratings yet
- RFLP & RapdDocument25 pagesRFLP & RapdBalaji Prasanna KumarNo ratings yet
- Maternal and Child Health ReferencesDocument4 pagesMaternal and Child Health ReferencesMeyke PotutuNo ratings yet
- 0097 Stage 5 Primary Science Scheme of Work Tcm142-595394Document69 pages0097 Stage 5 Primary Science Scheme of Work Tcm142-595394Romana Miriam OlivettiNo ratings yet
- Enzymes History and ClassificationDocument33 pagesEnzymes History and ClassificationZzeba KhanNo ratings yet
- Best Offer for EAMCET 2020 aspirantsDocument45 pagesBest Offer for EAMCET 2020 aspirantsrajaprasad2No ratings yet
- University EssayDocument2 pagesUniversity Essaykitzun sanNo ratings yet
- 5c Thailand - DMCR (Dhana)Document13 pages5c Thailand - DMCR (Dhana)Sanjeev KumarNo ratings yet
- NewbookchapteranthuriumDocument8 pagesNewbookchapteranthuriumTaashi Tiyon RuwanpathiranaNo ratings yet
- Fotosintesis 1213Document25 pagesFotosintesis 1213scanny16No ratings yet
- Approach To Skin Adnexal TumorsDocument20 pagesApproach To Skin Adnexal TumorsNirmalya Chakrabarti100% (1)
- The Plant Cell Wall A. IntroductionDocument6 pagesThe Plant Cell Wall A. IntroductionRizky EliandiNo ratings yet