You might also like
- A Review of Core Myopathy Central Core Disease Multiminic - 2021 - NeuromusculDocument10 pagesA Review of Core Myopathy Central Core Disease Multiminic - 2021 - NeuromusculSuzie Simone Mardones SilvaNo ratings yet
- Neurogenic Arthrogryposis and The Power of Phenoty 2021 Neuromuscular DisordDocument8 pagesNeurogenic Arthrogryposis and The Power of Phenoty 2021 Neuromuscular DisordSuzie Simone Mardones SilvaNo ratings yet
- Neurogenic Arthrogryposis and The Power of Phenoty - 2021 - Neuromuscular DisordDocument8 pagesNeurogenic Arthrogryposis and The Power of Phenoty - 2021 - Neuromuscular DisordSuzie Simone Mardones SilvaNo ratings yet
- Primary Mitochondrial Myopathies in Childhood 2021 Neuromuscular DisordersDocument10 pagesPrimary Mitochondrial Myopathies in Childhood 2021 Neuromuscular DisordersSuzie Simone Mardones SilvaNo ratings yet
- Met5. Mitochondrial DisordersDocument8 pagesMet5. Mitochondrial DisordersMonica J Ortiz PereiraNo ratings yet
- New Classification and Treatment For Myotonic Disorders: Review ArticleDocument6 pagesNew Classification and Treatment For Myotonic Disorders: Review ArticleDana DumitruNo ratings yet
- New Lymphatic Cell Formation Is Associated With Damaged Brain Tissue Clearance After Penetrating Traumatic Brain InjuryDocument8 pagesNew Lymphatic Cell Formation Is Associated With Damaged Brain Tissue Clearance After Penetrating Traumatic Brain Injurymuralim_phy1986No ratings yet
- Chronic Inflammatory Demyelinating PolyradiculoneuropathDocument13 pagesChronic Inflammatory Demyelinating Polyradiculoneuropathrafael rocha novaesNo ratings yet
- Transverse Myelitis: Pathogenesis, Diagnosis and Treatment: Frontiers in Bioscience June 2004Document18 pagesTransverse Myelitis: Pathogenesis, Diagnosis and Treatment: Frontiers in Bioscience June 2004fadelwputraNo ratings yet
- Zaman Muscle PathologyDocument14 pagesZaman Muscle PathologyartikslennonNo ratings yet
- Guerrini 2021Document13 pagesGuerrini 2021Francis CastellonNo ratings yet
- 300 FullDocument8 pages300 Fulldaf GREWNo ratings yet
- Abnormal DevelopmentDocument9 pagesAbnormal DevelopmentJatzully RVNo ratings yet
- Synapse Neurobiology: Week 5 - Part 2Document20 pagesSynapse Neurobiology: Week 5 - Part 2bobobNo ratings yet
- Diagnosis and Treatment of Mitochondrial MyopathiesDocument14 pagesDiagnosis and Treatment of Mitochondrial MyopathiesUname EpithetoNo ratings yet
- Et DGDocument11 pagesEt DGNathaly LapoNo ratings yet
- Myositis Diagnosis and Management.Document8 pagesMyositis Diagnosis and Management.zaquvubeNo ratings yet
- Brain Sciences: Multiple Sclerosis: Immunopathology and Treatment UpdateDocument27 pagesBrain Sciences: Multiple Sclerosis: Immunopathology and Treatment UpdateAhmed KumarNo ratings yet
- Mitochondrial Cytopathies: Ens Teaching ReviewDocument11 pagesMitochondrial Cytopathies: Ens Teaching ReviewGréta BotyánszkiNo ratings yet
- Revenge 3Document2 pagesRevenge 3Descargar scribdNo ratings yet
- Mitochondrial Disorders Overview - GeneReviews® - NCBI Bookshelf HTTPSWWW - Ncbi.nlm - nih.govbooksNBK1224Document24 pagesMitochondrial Disorders Overview - GeneReviews® - NCBI Bookshelf HTTPSWWW - Ncbi.nlm - nih.govbooksNBK1224denisaNo ratings yet
- Emss 74052Document31 pagesEmss 74052SARAHI MACIAS REALNo ratings yet
- Mitochondrial DiseaseDocument12 pagesMitochondrial DiseaseWSETNo ratings yet
- Muscle-Brain AxisDocument23 pagesMuscle-Brain AxisAnonymous y9EilyNo ratings yet
- RG 244035151Document21 pagesRG 244035151Radio ResidentNo ratings yet
- WHO2022 Update NeuroendocrinoDocument20 pagesWHO2022 Update NeuroendocrinoDoc ShivaNo ratings yet
- Fisiología Del Músculo Esquelético: Tema: Introducción Al MionúcleoDocument16 pagesFisiología Del Músculo Esquelético: Tema: Introducción Al MionúcleoDiana Jaramillo HNo ratings yet
- Proximal MiopatiasDocument19 pagesProximal MiopatiasJorge GámezNo ratings yet
- Lamperti 2010Document10 pagesLamperti 2010Marina GomesNo ratings yet
- 2022 Masingue P.Latour Rev Neurol Genetic Analysis in HereditaryDocument20 pages2022 Masingue P.Latour Rev Neurol Genetic Analysis in HereditaryLéo VidoniNo ratings yet
- Frontotemporal Dementia NeuropathologyDocument14 pagesFrontotemporal Dementia Neuropathologyppico1963No ratings yet
- Polycystic Kidney - Eight CasesDocument11 pagesPolycystic Kidney - Eight CasesKAINAT ANJUMNo ratings yet
- Secondary Syphilis Presenting As Diffused Folliculitis: ReferencesDocument3 pagesSecondary Syphilis Presenting As Diffused Folliculitis: ReferencesNazihan Safitri AlkatiriNo ratings yet
- 2016 - Algorithmic Approach To Neuroendocrine Tumors - Duan - 2016Document14 pages2016 - Algorithmic Approach To Neuroendocrine Tumors - Duan - 2016Pramod BiradarNo ratings yet
- Motor Neurone Disease PDFDocument4 pagesMotor Neurone Disease PDFTONY GO AWAYNo ratings yet
- Pathology QuizDocument4 pagesPathology QuizGamal ShohdyNo ratings yet
- Lim - Brain Somatic Mutations in MTOR Cause FCDIIDocument9 pagesLim - Brain Somatic Mutations in MTOR Cause FCDIIkudlaceksystemNo ratings yet
- 5437 FullDocument14 pages5437 FullFahrunnisa NurdinNo ratings yet
- Deg ModuleDocument15 pagesDeg Modulebiswajitpaul8403No ratings yet
- Critical Illness Polyneuropathy and Critical Illness Myopathy PDFDocument5 pagesCritical Illness Polyneuropathy and Critical Illness Myopathy PDFAhraxazel Galicia ReynaNo ratings yet
- Neuromuscular DiseaseDocument69 pagesNeuromuscular DiseaseDevi SiswaniNo ratings yet
- (03241750 - Acta Medica Bulgarica) Neurofibromatosis Type I (Von Recklinghausen Disease) - A Case Report and Review of The LiteratureDocument4 pages(03241750 - Acta Medica Bulgarica) Neurofibromatosis Type I (Von Recklinghausen Disease) - A Case Report and Review of The LiteratureTeodorNo ratings yet
- Fneur 12 648740Document7 pagesFneur 12 648740june.talon7No ratings yet
- Diverse Antigen Presentation by The Group 1 CD1 Molecule, CD1cDocument4 pagesDiverse Antigen Presentation by The Group 1 CD1 Molecule, CD1cPao MoralesNo ratings yet
- Transverse Myelitis AtfDocument3 pagesTransverse Myelitis AtfRishi VermaNo ratings yet
- A Homozygous MED11 C Terminal Variant Causes A Lethal Ne - 2022 - Genetics in MeDocument10 pagesA Homozygous MED11 C Terminal Variant Causes A Lethal Ne - 2022 - Genetics in Meronaldquezada038No ratings yet
- Recent Advances in Nemaline Myopathy: Jenni Laitila, Carina Wallgren-PetterssonDocument13 pagesRecent Advances in Nemaline Myopathy: Jenni Laitila, Carina Wallgren-PetterssonSuzie Simone Mardones SilvaNo ratings yet
- Complexity of Skeletal Muscle Degeneration Multi Systems Pathophysiology and Organ Crosstalk in DystrophinopathyDocument27 pagesComplexity of Skeletal Muscle Degeneration Multi Systems Pathophysiology and Organ Crosstalk in Dystrophinopathybose21No ratings yet
- Jurnal KUSTADocument10 pagesJurnal KUSTAzizee61No ratings yet
- Clearance of Defective Muscle Stem Cells by Senolytics Restores Myogenesis in Myotonic Dystrophy Type 1Document17 pagesClearance of Defective Muscle Stem Cells by Senolytics Restores Myogenesis in Myotonic Dystrophy Type 1wohoso4679No ratings yet
- 2011 Dickson FTLD TauDocument12 pages2011 Dickson FTLD TauvkarmoNo ratings yet
- Case Report of Intrafamilial Variability in Autosomal Recessive Centronuclear Myopathy Associated To A Novel BIN1 Stop MutationDocument6 pagesCase Report of Intrafamilial Variability in Autosomal Recessive Centronuclear Myopathy Associated To A Novel BIN1 Stop Mutationyael1991No ratings yet
- Mitophagy in Degenerative Joint DiseasesDocument12 pagesMitophagy in Degenerative Joint DiseaseseNo ratings yet
- Mitochondrial Encephalomyopathies (MEM)Document66 pagesMitochondrial Encephalomyopathies (MEM)Fatma KaledNo ratings yet
- Miopatías Inflamatorias IdiopáticasDocument14 pagesMiopatías Inflamatorias IdiopáticasGerarNo ratings yet
- JCB 2007Document10 pagesJCB 2007Supinder RawatNo ratings yet
- Johnson 2019Document14 pagesJohnson 2019Mariel González.No ratings yet
- CIDPDocument13 pagesCIDPOsvaldo CortésNo ratings yet
- ZV Class Links @medliferesuscitationDocument31 pagesZV Class Links @medliferesuscitationDebajyoti DasNo ratings yet
- Spinal Muscular Atrophy From Rags To Riches 2021 Neuromuscular DisordersDocument6 pagesSpinal Muscular Atrophy From Rags To Riches 2021 Neuromuscular DisordersSuzie Simone Mardones SilvaNo ratings yet
- Sarcoglycanopathies An Update 2021 Neuromuscular DisordersDocument7 pagesSarcoglycanopathies An Update 2021 Neuromuscular DisordersSuzie Simone Mardones SilvaNo ratings yet
- Fools Rush in Where Angels Fear To Tread: CommentaryDocument4 pagesFools Rush in Where Angels Fear To Tread: CommentarySuzie Simone Mardones SilvaNo ratings yet
- Congenital Muscular Dystrophies What Is New 2021 Neuromuscular DisordersDocument12 pagesCongenital Muscular Dystrophies What Is New 2021 Neuromuscular DisordersSuzie Simone Mardones SilvaNo ratings yet
- RS, 5-7Document33 pagesRS, 5-7Suzie Simone Mardones SilvaNo ratings yet
- Newborn Screening of Neuromuscular Diseases - 2021 - Neuromuscular DisordersDocument11 pagesNewborn Screening of Neuromuscular Diseases - 2021 - Neuromuscular DisordersSuzie Simone Mardones SilvaNo ratings yet
- Reflections On The World Muscle Society: 1. A New UniverseDocument6 pagesReflections On The World Muscle Society: 1. A New UniverseSuzie Simone Mardones SilvaNo ratings yet
- Recent Advances in Nemaline Myopathy: Jenni Laitila, Carina Wallgren-PetterssonDocument13 pagesRecent Advances in Nemaline Myopathy: Jenni Laitila, Carina Wallgren-PetterssonSuzie Simone Mardones SilvaNo ratings yet
- Dialight CE Catalogue 2016 2Document60 pagesDialight CE Catalogue 2016 2KABRENo ratings yet
- Nazi Germany IGCSE QuestionDocument2 pagesNazi Germany IGCSE QuestionNeema AkalaNo ratings yet
- Introduction To French FestivalsDocument8 pagesIntroduction To French Festivalsmanyabhutani1308No ratings yet
- F1 Case IIM BangaloreDocument32 pagesF1 Case IIM Bangalorerishabh jainNo ratings yet
- MS For Alloy Steel Pipe FabricationDocument9 pagesMS For Alloy Steel Pipe FabricationuemaaplNo ratings yet
- 4th Competency Mapping (Final)Document11 pages4th Competency Mapping (Final)Mitz JazNo ratings yet
- Qdoc - Tips - PHP and Mysql Project On Invoice Management SystemDocument119 pagesQdoc - Tips - PHP and Mysql Project On Invoice Management SystemREDNo ratings yet
- Applying Quality StandardsDocument11 pagesApplying Quality StandardsKay Tracey Urbiztondo100% (1)
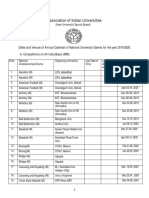
- Sports Calendar 2019-20 PDFDocument10 pagesSports Calendar 2019-20 PDFSailajaNo ratings yet
- TurpDocument9 pagesTurpIndah HarnitaNo ratings yet
- Monster Bestiary Full - OdsDocument886 pagesMonster Bestiary Full - Odsellie cressyNo ratings yet
- Umberto Eco - How To Write A Thesis EbookDocument8 pagesUmberto Eco - How To Write A Thesis Ebookfc51eh59100% (2)
- ABB Motor General CatalogueDocument27 pagesABB Motor General CatalogueargaNo ratings yet
- Cuestionario de Evaluación. Unit 10 - Revisión Del IntentoDocument4 pagesCuestionario de Evaluación. Unit 10 - Revisión Del IntentoPetraNo ratings yet
- Compilation of Academic PapersDocument27 pagesCompilation of Academic PapersGerald LandichoNo ratings yet
- Strategist 14Document159 pagesStrategist 14Namrit ZatakiyaNo ratings yet
- Ars Quatuor Coronatorum v21 1000057345Document496 pagesArs Quatuor Coronatorum v21 1000057345Δημητρης Ιατριδης0% (1)
- Justification of StorytellingDocument3 pagesJustification of StorytellingJoanne Lian Li FangNo ratings yet
- Lecture 1 - Part 1 - Introduction To ECE 105Document12 pagesLecture 1 - Part 1 - Introduction To ECE 105homamhomarNo ratings yet
- Kali Hanuman Vani HanumanjiDocument11 pagesKali Hanuman Vani HanumanjiDharmendrasinh AtaliaNo ratings yet
- Arduino Electronics Blueprints - Sample ChapterDocument33 pagesArduino Electronics Blueprints - Sample ChapterPackt Publishing100% (1)
- ASSIGNMENT Marketing Coca ColaDocument11 pagesASSIGNMENT Marketing Coca ColaFazal MuhammedNo ratings yet
- Basic English I: Fadia NaeemDocument12 pagesBasic English I: Fadia Naeemwaleed waleedNo ratings yet
- Food Drink Europe Memoria 2015Document28 pagesFood Drink Europe Memoria 2015intspainNo ratings yet
- Deped Matatag CurriculumDocument22 pagesDeped Matatag CurriculumNELLY L. ANONUEVO100% (5)
- Firewalld Iptables (Continued)Document36 pagesFirewalld Iptables (Continued)Alex ValenciaNo ratings yet
- Morality: How Black Is The Night?: Moral Option 1: A Worthy OpponentDocument8 pagesMorality: How Black Is The Night?: Moral Option 1: A Worthy OpponentmpotatoNo ratings yet
- Journal LL ManojDocument5 pagesJournal LL ManojmanojNo ratings yet
- Posting+0051-2023 +Resolution+No +01,+series+of+2023+ (E) + (HVB+SGD)Document6 pagesPosting+0051-2023 +Resolution+No +01,+series+of+2023+ (E) + (HVB+SGD)Carolyn VillagraciaNo ratings yet
- ĐỀ TIẾNG ANH - ÔN TUYỂN SINH 10 SỐ 02Document4 pagesĐỀ TIẾNG ANH - ÔN TUYỂN SINH 10 SỐ 02Minh ChâuNo ratings yet