Professional Documents
Culture Documents
377 Hyperthyroidism
377 Hyperthyroidism
Uploaded by
allenh016Original Title
Copyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
377 Hyperthyroidism
377 Hyperthyroidism
Uploaded by
allenh016Copyright:
Available Formats
may be needed if there is severe hyponatremia or hypoglycemia; rarely begins before adolescence and typically occurs between 20 and
curs between 20 and 2703
hypotonic IV fluids should be avoided because they may exacerbate 50 years of age; it also occurs in the elderly.
water retention secondary to reduced renal perfusion and inappro-
priate vasopressin secretion. The metabolism of most medications
Pathogenesis As in autoimmune hypothyroidism, a combina-
tion of environmental and genetic factors, including polymorphisms
is impaired, and sedatives should be avoided if possible or used in
in HLA-DR, the immunoregulatory genes CTLA-4, CD25, PTPN22,
reduced doses. Medication blood levels should be monitored, when
FCRL3, and CD226, as well as the gene encoding the thyroid-
available, to guide dosage.
stimulating hormone receptor (TSH-R), contributes to Graves’ disease
susceptibility. The concordance for Graves’ disease in monozygotic
■■FURTHER READING twins is 20–30%, compared to <5% in dizygotic twins. Indirect evidence
Hanley P et al: Thyroid disorders in children and adolescents: A suggests that stress is an important environmental factor, presumably
CHAPTER 377 Hyperthyroidism
review. JAMA Pediatr 170:1008, 2016. operating through neuroendocrine effects on the immune system.
Jonklaas J et al: Guidelines for the treatment of hypothyroidism: Smoking is a minor risk factor for Graves’ disease and a major risk fac-
Prepared by the American Thyroid Association Task Force on thyroid tor for the development of ophthalmopathy. Sudden increases in iodine
hormone replacement. Thyroid 24:1670, 2014. intake may precipitate Graves’ disease, and there is a threefold increase
Rugge JB, Bougatsos C, Chou R: Screening and treatment of thyroid in the occurrence of Graves’ disease in the postpartum period. Graves’
dysfunction: An evidence review for the U. S. Preventive Services disease may occur during the immune reconstitution phase after highly
Task Force. Ann Intern Med 162:35, 2015. active antiretroviral therapy (HAART) or alemtuzumab treatment.
The hyperthyroidism of Graves’ disease is caused by thyroid-
stimulating immunoglobulin (TSI) that are synthesized in the thyroid
gland as well as in bone marrow and lymph nodes. Such antibodies
can be detected by bioassays or by using the more widely available
377 Hyperthyroidism
J. Larry Jameson, Susan J. Mandel,
thyrotropin-binding inhibitory immunoglobulin (TBII) assays. The
presence of TBII in a patient with thyrotoxicosis implies the existence
of TSI, and these assays are useful in monitoring pregnant Graves’
Anthony P. Weetman patients in whom high levels of TSI can cross the placenta and cause
neonatal thyrotoxicosis. Other thyroid autoimmune responses, similar
to those in autoimmune hypothyroidism (see above), occur concur-
THYROTOXICOSIS rently in patients with Graves’ disease. In particular, thyroid peroxi-
Thyrotoxicosis is defined as the state of thyroid hormone excess and is dase (TPO) and thyroglobulin (Tg) antibodies occur in up to 80% of
not synonymous with hyperthyroidism, which is the result of excessive cases. Because the coexisting thyroiditis can also affect thyroid func-
thyroid function. However, the major etiologies of thyrotoxicosis are tion, there is no direct correlation between the level of TSI and thyroid
hyperthyroidism caused by Graves’ disease, toxic multinodular goiter hormone levels in Graves’ disease.
(MNG), and toxic adenomas. Other causes are listed in Table 377-1. Cytokines appear to play a major role in thyroid-associated ophthal-
mopathy. There is infiltration of the extraocular muscles by activated
■■GRAVES’ DISEASE T cells; the release of cytokines such as interferon γ (IFN-γ), tumor
necrosis factor (TNF), and interleukin-1 (IL-1) results in fibroblast acti-
Epidemiology Graves’ disease accounts for 60–80% of thyrotox- vation and increased synthesis of glycosaminoglycans that trap water,
icosis. The prevalence varies among populations, reflecting genetic thereby leading to characteristic muscle swelling. Late in the disease,
factors and iodine intake (high iodine intake is associated with an there is irreversible fibrosis of the muscles. Though the pathogenesis of
increased prevalence of Graves’ disease). Graves’ disease occurs in thyroid-associated ophthalmopathy remains unclear, there is mounting
up to 2% of women but is one-tenth as frequent in men. The disorder evidence that the TSH-R is a shared autoantigen that is expressed in the
orbit; this would explain the close association with autoimmune thy-
TABLE 377-1 Causes of Thyrotoxicosis roid disease. Increased fat is an additional cause of retrobulbar tissue
Primary Hyperthyroidism expansion. The increase in intraorbital pressure can lead to proptosis,
Graves’ disease diplopia, and optic neuropathy.
Toxic multinodular goiter Clinical Manifestations Signs and symptoms include features
Toxic adenoma that are common to any cause of thyrotoxicosis (Table 377-2) as well
Functioning thyroid carcinoma metastases as those specific for Graves’ disease. The clinical presentation depends
Activating mutation of the TSH receptor on the severity of thyrotoxicosis, the duration of disease, individual
Activating mutation of GSα (McCune-Albright syndrome) susceptibility to excess thyroid hormone, and the patient’s age. In
Struma ovarii
the elderly, features of thyrotoxicosis may be subtle or masked, and
patients may present mainly with fatigue and weight loss, a condition
Drugs: iodine excess (Jod-Basedow phenomenon)
known as apathetic thyrotoxicosis.
Thyrotoxicosis without Hyperthyroidism
Subacute thyroiditis TABLE 377-2 Signs and Symptoms of Thyrotoxicosis (Descending
Silent thyroiditis Order of Frequency)
Other causes of thyroid destruction: amiodarone, radiation, infarction of SYMPTOMS SIGNSa
adenoma Hyperactivity, irritability, dysphoria Tachycardia; atrial fibrillation in the
Ingestion of excess thyroid hormone (thyrotoxicosis factitia) or thyroid tissue Heat intolerance and sweating elderly
Secondary Hyperthyroidism Palpitations Tremor
TSH-secreting pituitary adenoma Fatigue and weakness Goiter
Thyroid hormone resistance syndrome: occasional patients may have features Weight loss with increased appetite Warm, moist skin
of thyrotoxicosis Diarrhea Muscle weakness, proximal myopathy
Chorionic gonadotropin-secreting tumorsa Polyuria Lid retraction or lag
Gestational thyrotoxicosisa Oligomenorrhea, loss of libido Gynecomastia
Circulating TSH levels are low in these forms of secondary hyperthyroidism.
a
a
Excludes the signs of ophthalmopathy and dermopathy specific for Graves’
Abbreviation: TSH, thyroid-stimulating hormone. disease.
Harrisons_20e_Part12_p2649-p3024.indd 2703 6/1/18 3:27 PM
2704 Thyrotoxicosis may cause unexplained weight loss, despite an
enhanced appetite, due to the increased metabolic rate. Weight gain
occurs in 5% of patients, however, because of increased food intake.
Other prominent features include hyperactivity, nervousness, and
irritability, ultimately leading to a sense of easy fatigability in some
patients. Insomnia and impaired concentration are common; apathetic
thyrotoxicosis may be mistaken for depression in the elderly. Fine
tremor is a frequent finding, best elicited by having patients stretch
out their fingers while feeling the fingertips with the palm. Common
neurologic manifestations include hyperreflexia, muscle wasting, and
proximal myopathy without fasciculation. Chorea is rare. Thyrotox-
icosis is sometimes associated with a form of hypokalemic periodic
PART 12
paralysis; this disorder is particularly common in Asian males with A B
thyrotoxicosis, but it occurs in other ethnic groups as well.
The most common cardiovascular manifestation is sinus tachycardia,
often associated with palpitations, occasionally caused by supraven-
Endocrinology and Metabolism
tricular tachycardia. The high cardiac output produces a bounding
pulse, widened pulse pressure, and an aortic systolic murmur and can
lead to worsening of angina or heart failure in the elderly or those with
preexisting heart disease. Atrial fibrillation is more common in patients
>50 years of age. Treatment of the thyrotoxic state alone converts atrial
fibrillation to normal sinus rhythm in about half of patients, suggesting
the existence of an underlying cardiac problem in the remainder.
The skin is usually warm and moist, and the patient may complain
C
of sweating and heat intolerance, particularly during warm weather.
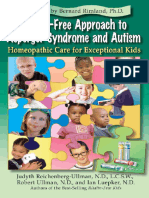
Palmar erythema, onycholysis, and, less commonly, pruritus, urticaria, FIGURE 377-1 Features of Graves’ disease. A. Ophthalmopathy in Graves’
and diffuse hyperpigmentation may be evident. Hair texture may disease; lid retraction, periorbital edema, conjunctival injection, and proptosis are
marked. B. Thyroid dermopathy over the lateral aspects of the shins. C. Thyroid
become fine, and a diffuse alopecia occurs in up to 40% of patients, acropachy.
persisting for months after restoration of euthyroidism. Gastrointes-
tinal transit time is decreased, leading to increased stool frequency,
often with diarrhea and occasionally mild steatorrhea. Women fre- serious manifestation is compression of the optic nerve at the apex of
quently experience oligomenorrhea or amenorrhea; in men, there may the orbit, leading to papilledema; peripheral field defects; and, if left
be impaired sexual function and, rarely, gynecomastia. The direct untreated, permanent loss of vision.
effect of thyroid hormones on bone resorption leads to osteopenia The “NO SPECS” scoring system to evaluate ophthalmopathy is an
in long-standing thyrotoxicosis; mild hypercalcemia occurs in up acronym derived from the following changes:
to 20% of patients, but hypercalciuria is more common. There is a
small increase in fracture rate in patients with a previous history of 0 = No signs or symptoms
thyrotoxicosis. 1 = Only signs (lid retraction or lag), no symptoms
In Graves’ disease, the thyroid is usually diffusely enlarged to two 2 = Soft tissue involvement (periorbital edema)
to three times its normal size. The consistency is firm, but not nodular. 3 = Proptosis (>22 mm)
There may be a thrill or bruit, best detected at the inferolateral margins 4 = Extraocular muscle involvement (diplopia)
of the thyroid lobes, due to the increased vascularity of the gland and 5 = Corneal involvement
the hyperdynamic circulation. 6 = Sight loss
Lid retraction, causing a staring appearance, can occur in any Although useful as a mnemonic, the NO SPECS scheme is inade-
form of thyrotoxicosis and is the result of sympathetic overactivity. quate to describe the eye disease fully, and patients do not necessarily
However, Graves’ disease is associated with specific eye signs that progress from one class to another; alternative scoring systems (e.g.,
comprise Graves’ ophthalmopathy (Fig. 377-1A). This condition is also the EUGOGO system developed by the European Group On Graves’
called thyroid-associated ophthalmopathy, because it occurs in the absence Orbitopathy) that assess disease activity are preferable for monitoring
of hyperthyroidism in 10% of patients. Most of these individuals and treatment purposes. When Graves’ eye disease is active and severe,
have autoimmune hypothyroidism or thyroid antibodies. The onset referral to an ophthalmologist is indicated and objective measurements
of Graves’ ophthalmopathy occurs within the year before or after are needed, such as lid-fissure width; corneal staining with fluores-
the diagnosis of thyrotoxicosis in 75% of patients but can sometimes cein; and evaluation of extraocular muscle function (e.g., Hess chart),
precede or follow thyrotoxicosis by several years, accounting for some intraocular pressure and visual fields, acuity, and color vision.
cases of euthyroid ophthalmopathy. Thyroid dermopathy occurs in <5% of patients with Graves’ disease
Some patients with Graves’ disease have little clinical evidence of (Fig. 377-1B), almost always in the presence of moderate or severe
ophthalmopathy. However, the enlarged extraocular muscles typical of ophthalmopathy. Although most frequent over the anterior and lat-
the disease, and other subtle features, can be detected in most patients eral aspects of the lower leg (hence the term pretibial myxedema), skin
when investigated by ultrasound or computed tomography (CT) imag- changes can occur at other sites, particularly after trauma. The typical
ing of the orbits. Unilateral signs are found in up to 10% of patients. lesion is a noninflamed, indurated plaque with a deep pink or purple
The earliest manifestations of ophthalmopathy are usually a sensation color and an “orange skin” appearance. Nodular involvement can
of grittiness, eye discomfort, and excess tearing. About one-third of occur, and the condition can rarely extend over the whole lower leg
patients have proptosis, best detected by visualization of the sclera and foot, mimicking elephantiasis. Thyroid acropachy refers to a form of
between the lower border of the iris and the lower eyelid, with the clubbing found in <1% of patients with Graves’ disease (Fig. 377-1C).
eyes in the primary position. Proptosis can be measured using an exo- It is so strongly associated with thyroid dermopathy that an alternative
phthalmometer. In severe cases, proptosis may cause corneal exposure cause of clubbing should be sought in a Graves’ patient without coin-
and damage, especially if the lids fail to close during sleep. Periorbital cident skin and orbital involvement.
edema, scleral injection, and chemosis are also frequent. In 5–10% of
patients, the muscle swelling is so severe that diplopia results, typically, Laboratory Evaluation Investigations used to determine the
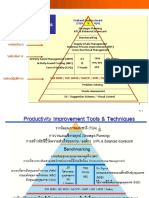
but not exclusively, when the patient looks up and laterally. The most existence and cause of thyrotoxicosis are summarized in Fig. 377-2. In
Harrisons_20e_Part12_p2649-p3024.indd 2704 6/1/18 3:27 PM
2705
EVALUATION OF THYROTOXICOSIS
Measure TSH, unbound T4
TSH low, unbound TSH low, unbound TSH normal or increased, TSH and unbound
T4 high T4 normal high unbound T4 T4 normal
Primary Measure TSH-secreting
thyrotoxicosis unbound T3 pituitary adenoma
or thyroid hormone
resistance syndrome
CHAPTER 377 Hyperthyroidism
High Normal
T3 toxicosis Subclinical No further tests
hyperthyroidism
Features of Follow up in
Graves’ diseasea? 6-12 weeks
Yes No
Graves’ disease Multinodular goiter or toxic adenomab?
Yes No
Toxic nodular hyperthyroidism Low radionuclide uptake?
Yes No
Destructive thyroiditis, iodine excess Rule out other causes including stimulation
or excess thyroid hormone by chorionic gonadotropin
FIGURE 377-2 Evaluation of thyrotoxicosis. aDiffuse goiter, positive TPO antibodies or TRAb, ophthalmopathy, dermopathy. bCan be confirmed by radionuclide scan.
TSH, thyroid-stimulating hormone.
Graves’ disease, the TSH level is suppressed, and total and unbound Clinical Course Clinical features generally worsen without treat-
thyroid hormone levels are increased. In 2–5% of patients (and more ment; mortality was 10–30% before the introduction of satisfactory
in areas of borderline iodine intake), only T3 is increased (T3 toxicosis). therapy. Some patients with mild Graves’ disease experience spontane-
The converse state of T4 toxicosis, with elevated total and unbound ous relapses and remissions. Rarely, there may be fluctuation between
T4 and normal T3 levels, is occasionally seen when hyperthyroidism hypo- and hyperthyroidism due to changes in the functional activity
is induced by excess iodine, providing surplus substrate for thyroid of TSH-R antibodies. About 15% of patients who enter remission after
hormone synthesis. Measurement of TPO antibodies or TBII may be treatment develop hypothyroidism 10–15 years later as a result of the
useful if the diagnosis is unclear clinically but is not needed routinely. destructive autoimmune process.
Associated abnormalities that may cause diagnostic confusion in thy- The clinical course of ophthalmopathy does not follow that of the
rotoxicosis include elevation of bilirubin, liver enzymes, and ferritin. thyroid disease, although thyroid dysfunction can worsen eye signs.
Microcytic anemia and thrombocytopenia may occur. Ophthalmopathy typically worsens over the initial 3–6 months, fol-
lowed by a plateau phase over the next 12–18 months, and then some
Differential Diagnosis Diagnosis of Graves’ disease is straight- spontaneous improvement, particularly in the soft tissue changes.
forward in a patient with biochemically confirmed thyrotoxicosis, However, the course is more fulminant in up to 5% of patients, requir-
diffuse goiter on palpation, ophthalmopathy, and often a personal or ing intervention in the acute phase if there is optic nerve compression
family history of autoimmune disorders. For patients with thyrotox- or corneal ulceration. Diplopia may appear late in the disease due to
icosis who lack these features, the diagnosis is generally established fibrosis of the extraocular muscles. Radioiodine treatment for hyper-
by a radionuclide (99mTc, 123I, or 131I) scan and uptake of the thyroid, thyroidism worsens the eye disease in a small proportion of patients
which will distinguish the diffuse, high uptake of Graves’ disease from (especially smokers). Antithyroid drugs or surgery have no adverse
destructive thyroiditis, ectopic thyroid tissue, and factitious thyrotox- effects on the clinical course of ophthalmopathy. Thyroid dermopathy,
icosis, as well as diagnosing a toxic adenoma or toxic MNG. Alterna- when it occurs, usually appears 1–2 years after the development of
tively, TRAb measurement can be used to diagnose Graves’ disease and Graves’ hyperthyroidism; it may improve spontaneously.
color-flow Doppler ultrasonography may distinguish between hyper-
thyroidism (with increased blood flow) and destructive thyroiditis. In
secondary hyperthyroidism due to a TSH-secreting pituitary tumor,
there is also a diffuse goiter. The presence of a nonsuppressed TSH TREATMENT
level and the finding of a pituitary tumor on CT or magnetic resonance Graves’ Disease
imaging (MRI) scan suggest this diagnosis.
Clinical features of thyrotoxicosis can mimic certain aspects of other The hyperthyroidism of Graves’ disease is treated by reducing thy-
disorders, including panic attacks, mania, pheochromocytoma, and roid hormone synthesis, using an antithyroid drug, or reducing
weight loss associated with malignancy. The diagnosis of thyrotoxi- the amount of thyroid tissue with radioiodine (131I) treatment or by
cosis can be easily excluded if the TSH and unbound T4 and T3 levels thyroidectomy. Antithyroid drugs are the predominant therapy in
are normal. A normal TSH also excludes Graves’ disease as a cause of many centers in Europe, Latin America, and Japan, whereas radioio-
diffuse goiter. dine is more often the first line of treatment in North America. These
Harrisons_20e_Part12_p2649-p3024.indd 2705 6/1/18 3:27 PM
2706 differences reflect the fact that no single approach is optimal and adrenergic symptoms, especially in the early stages before antithy-
that patients may require multiple treatments to achieve remission. roid drugs take effect. Beta blockers are also useful in patients with
The main antithyroid drugs are thionamides; propylthiouracil, thyrotoxic periodic paralysis, pending correction of thyrotoxicosis.
carbimazole (not available in the United States), and the active In consultation with a cardiologist, anticoagulation with warfarin
metabolite of the latter, methimazole. All inhibit the function of TPO, should be considered in all patients with atrial fibrillation; there is
reducing oxidation and organification of iodide. These drugs also often spontaneous reversion to sinus rhythm with control of hyper-
reduce thyroid antibody levels by mechanisms that remain unclear, thyroidism, and long-term anticoagulation is not usually needed.
and they appear to enhance spontaneous rates of remission. Pro- Decreased warfarin doses are required when patients are thyrotoxic.
pylthiouracil inhibits deiodination of T4 → T3. However, this effect If digoxin is used, increased doses are often needed in the thyrotoxic
is of minor benefit, except in the most severe thyrotoxicosis, and is state.
offset by the much shorter half-life of this drug (90 min) compared to Radioiodine causes progressive destruction of thyroid cells and
methimazole (6 h). Due to the hepatotoxicity of propylthiouracil, the can be used as initial treatment or for relapses after a trial of antithy-
PART 12
U.S. Food and Drug Administration (FDA) has limited indications roid drugs. There is a small risk of thyrotoxic crisis (see below)
for its use to the first trimester of pregnancy, the treatment of thyroid after radioiodine, which can be minimized by pretreatment with
storm, and patients with minor adverse reactions to methimazole. antithyroid drugs for at least a month before treatment. Antecedent
If propylthiouracil is used, monitoring of liver function tests is treatment with an antithyroid drug and a beta blocker should be
Endocrinology and Metabolism
recommended. considered for all elderly patients or for those with cardiac prob-
There are many variations of antithyroid drug regimens. The lems. Carbimazole or methimazole must be stopped 2–3 days before
initial dose of carbimazole or methimazole is usually 10–20 mg radioiodine administration to achieve optimum iodine uptake, and
every 8 or 12 h, but once-daily dosing is possible after euthyroidism can be restarted 3–7 days after radioiodine in those at risk of com-
is restored. Propylthiouracil is given at a dose of 100–200 mg every plications from worsening thyrotoxicosis. Propylthiouracil appears
6–8 h, and divided doses are usually given throughout the course. to have a prolonged radioprotective effect and should be stopped
Lower doses of each drug may suffice in areas of low iodine intake. for a longer period before radioiodine is given, or a larger dose of
The starting dose of an antithyroid drug can be gradually reduced radioiodine will be necessary.
(titration regimen) as thyrotoxicosis improves. Less commonly, high Efforts to calculate an optimal dose of radioiodine that achieves
doses may be given combined with levothyroxine supplementation euthyroidism without a high incidence of relapse or progression to
(block-replace regimen) to avoid drug-induced hypothyroidism. hypothyroidism have not been successful. Some patients inevitably
The titration regimen is preferred to minimize the dose of antithy- relapse after a single dose because the biologic effects of radiation
roid drug and provide an index of treatment response. vary between individuals, and hypothyroidism cannot be uniformly
Thyroid function tests and clinical manifestations are reviewed avoided even using accurate dosimetry. A practical strategy is to
4–6 weeks after starting treatment, and the dose is titrated based give a fixed dose based on clinical features, such as the severity of
on unbound T4 levels. Most patients do not achieve euthyroidism thyrotoxicosis, the size of the goiter (increases the dose needed),
until 6–8 weeks after treatment is initiated. TSH levels often remain and the level of radioiodine uptake (decreases the dose needed). 131I
suppressed for several months and therefore do not provide a sen- dosage generally ranges between 370 MBq (10 mCi) and 555 MBq
sitive index of treatment response. The usual daily maintenance (15 mCi). Most authorities favor an approach aimed at thyroid abla-
doses of antithyroid drugs in the titration regimen are 2.5–10 mg tion (as opposed to euthyroidism), given that levothyroxine replace-
of carbimazole or methimazole and 50–100 mg of propylthiouracil. ment is straightforward and most patients ultimately progress to
In the block-replace regimen, the initial dose of antithyroid drug is hypothyroidism over 5–10 years, frequently with some delay in the
held constant, and the dose of levothyroxine is adjusted to maintain diagnosis of hypothyroidism.
normal unbound T4 levels. When TSH suppression is alleviated, Certain radiation safety precautions are necessary in the first
TSH levels can also be used to monitor therapy. few days after radioiodine treatment, but the exact guidelines vary
Maximum remission rates (up to 30–60% in some populations) depending on local protocols. In general, patients need to avoid
are achieved by 12–18 months for the titration regimen and are close, prolonged contact with children and pregnant women for
higher in patients where TRAb levels are no longer detected, than 5–7 days because of possible transmission of residual isotope and
in those with TRAb persistence. For unclear reasons, remission rates exposure to radiation emanating from the gland. Rarely, there may
appear to vary in different geographic regions. Younger patients, be mild pain due to radiation thyroiditis 1–2 weeks after treatment.
males, smokers, and patients with a history of allergy, severe hyper- Hyperthyroidism can persist for 2–3 months before radioiodine
thyroidism or large goiters are most likely to relapse when treatment takes full effect. For this reason, β-adrenergic blockers or antithy-
stops, but outcomes are difficult to predict. All patients should be roid drugs can be used to control symptoms during this interval.
followed closely for relapse during the first year after treatment and Persistent hyperthyroidism can be treated with a second dose of
at least annually thereafter. radioiodine, usually 6 months after the first dose. The risk of hypo-
The common minor side effects of antithyroid drugs are rash, thyroidism after radioiodine depends on the dosage but is at least
urticaria, fever, and arthralgia (1–5% of patients). These may resolve 10–20% in the first year and 5% per year thereafter. Patients should
spontaneously or after substituting an alternative antithyroid drug; be informed of this possibility before treatment and require close
rashes may respond to an antihistamine. Rare but major side effects follow-up during the first year followed by annual thyroid function
include hepatitis (especially with propylthiouracil; avoid use in testing.
children) and cholestasis (methimazole and carbimazole); vasculi- Pregnancy and breast-feeding are absolute contraindications to
tis; and, most important, agranulocytosis (<1%). It is essential that radioiodine treatment, but patients can conceive safely 6 months
antithyroid drugs are stopped and not restarted if a patient develops after treatment. The presence of ophthalmopathy, especially in
major side effects. Written instructions should be provided regard- smokers, requires caution. Prednisone, 30 mg/d, at the time of
ing the symptoms of possible agranulocytosis (e.g., sore throat, radioiodine treatment, tapered over 6–8 weeks may prevent exac-
fever, mouth ulcers) and the need to stop treatment pending an erbation of ophthalmopathy, but radioiodine should generally be
urgent complete blood count to confirm that agranulocytosis is not avoided in those with active moderate to severe eye disease. The
present. Management of agranulocytosis is described in Chap. 98. overall risk of cancer after radioiodine treatment in adults is not
It is not useful to monitor blood counts prospectively, because the increased. Although many physicians avoid radioiodine in children
onset of agranulocytosis is idiosyncratic and abrupt. and adolescents because of the theoretical risks of malignancy,
Propranolol (20–40 mg every 6 h) or longer-acting selective emerging evidence suggests that radioiodine can be used safely in
β1 receptor blockers such as atenolol may be helpful to control older children.
Harrisons_20e_Part12_p2649-p3024.indd 2706 6/1/18 3:27 PM
Total or near-total thyroidectomy is an option for patients who propylthiouracil, stable iodide (5 drops SSKI every 6 h) is given to 2707
relapse after antithyroid drugs and prefer this treatment to radioio- block thyroid hormone synthesis via the Wolff-Chaikoff effect (the
dine. Some experts recommend surgery in young individuals, delay allows the antithyroid drug to prevent the excess iodine from
particularly when the goiter is very large. Careful control of thy- being incorporated into new hormone). Propranolol should also be
rotoxicosis with antithyroid drugs, followed by potassium iodide given to reduce tachycardia and other adrenergic manifestations
(1–2 drops SSKI orally tid for 10 days), is needed prior to surgery to (60–80 mg PO every 4 h; or 2 mg IV every 4 h). Although other
avoid thyrotoxic crisis and to reduce the vascularity of the gland. The β-adrenergic blockers can be used, high doses of propranolol decrease
major complications of surgery—bleeding, laryngeal edema, hypo- T4 → T3 conversion, and the doses can be easily adjusted. Caution
parathyroidism, and damage to the recurrent laryngeal nerves—are is needed to avoid acute negative inotropic effects, but controlling
unusual when the procedure is performed by highly experienced the heart rate is important, as some patients develop a form of high-
surgeons. Recurrence rates in the best series are <2%, but the rate of output heart failure. Short-acting IV esmolol can be used to decrease
CHAPTER 377 Hyperthyroidism
hypothyroidism is similar to that following radioiodine treatment, heart rate while monitoring for signs of heart failure. Additional
especially with the current trend away from subtotal thyroidectomy. therapeutic measures include glucocorticoids (e.g., hydrocortisone
Antithyroid drugs should be used to manage Graves’ disease 300 mg IV bolus, then 100 mg every 8 h), antibiotics if infection is
in pregnancy. Because transplacental passage of these drugs may present, cholestyramine to sequester thyroid hormones, cooling,
produce fetal hypothyroidism and goiter if the maternal dose is oxygen, and IV fluids.
excessive, maternal antithyroid dose titration should target serum Ophthalmopathy requires no active treatment when it is mild
free or total T4 levels at or just above the pregnancy reference range. or moderate, because there is usually spontaneous improvement.
If available, propylthiouracil should be used until 14–16 weeks’ General measures include meticulous control of thyroid hormone
gestation because of the association of rare cases of methimazole/ levels, cessation of smoking, and an explanation of the natural his-
carbimazole embryopathy, including aplasia cutis and other defects, tory of ophthalmopathy. Discomfort can be relieved with artificial
such as choanal atresia and tracheoesophageal fistulae. Because of tears (e.g., hypromellose 0.3% or carbomer 0.2% ophthalmic gel)
the potential for teratogenic effects, recent recommendations sug- paraffin-based eye ointment, and the use of dark glasses with side
gest discontinuation of antithyroid medication in a newly pregnant frames. Periorbital edema may respond to a more upright sleeping
woman with Graves’ disease, who is euthyroid on a low dose of position or a diuretic. Corneal exposure during sleep can be avoided
methimazole (<5–10 mg/day) or PTU (<100–200 mg/day), after by using patches or taping the eyelids shut. Minor degrees of diplo-
evaluating recent thyroid function tests, disease history, goiter size, pia improve with prisms fitted to spectacles. Some authorities also
duration of therapy, and TRAb measurement. Following cessation, advocate selenium 100 μg bd. Severe ophthalmopathy, with optic
careful monitoring of maternal thyroid function tests is essential. On nerve involvement or chemosis resulting in corneal damage, is an
the other hand, for women at high risk of developing thyrotoxicosis emergency requiring joint management with an ophthalmologist.
if antithyroid drugs are discontinued (large goiter, requirement for Pulse therapy with IV methylprednisolone (e.g., 500 mg of meth-
higher antithyroid drug dosage), continued therapy is necessary, ylprednisolone once weekly for 6 weeks, then 250 mg once weekly
with PTU (if available) administration in the first trimester. But, for 6 weeks) is preferable to oral glucocorticoids, which are used
because of its rare association with hepatotoxicity, propylthiouracil for moderately active disease. When glucocorticoids are ineffective,
should be limited to the first trimester and then maternal therapy orbital decompression can be achieved by removing bone from any
should be converted to methimazole (or carbimazole) at a ratio of wall of the orbit, thereby allowing displacement of fat and swol-
15–20 mg of propylthiouracil to 1 mg of methimazole. It is often len extraocular muscles. The transantral route is used most often
possible to stop treatment in the last trimester because TSIs tend because it requires no external incision. Proptosis recedes an average
to decline in pregnancy. Nonetheless, the transplacental transfer of 5 mm, but there may be residual or even worsened diplopia. Once
of these antibodies if present at levels 3 times higher than the the eye disease has stabilized, surgery may be indicated for relief of
normative range rarely causes fetal or neonatal thyrotoxicosis. Poor diplopia and correction of the appearance. External beam radiother-
intrauterine growth, a fetal heart rate of >160 beats/min, advanced apy of the orbits has been used for many years, but the efficacy of
bone age, fetal goiter, and high levels of maternal TSI after 26 weeks this therapy remains unclear, and it is best reserved for those with
gestation may herald this complication. Antithyroid drugs given moderately active disease who have failed or are not candidates
to the mother can be used to treat the fetus and may be needed for for glucocorticoid therapy. Other immunosuppressive agents such
1–3 months after delivery, until the maternal antibodies disappear as rituximab have shown some benefit, but their role is yet to be
from the baby’s circulation. The postpartum period is a time of major established.
risk for relapse of Graves’ disease. Breast-feeding is safe with low Thyroid dermopathy does not usually require treatment, but it can
doses of antithyroid drugs. Graves’ disease in children is usually man- cause cosmetic problems or interfere with the fit of shoes. Surgical
aged initially with methimazole or carbimazole (avoid propylthioura- removal is not indicated. If necessary, treatment consists of topical,
cil), often given as a prolonged course of the titration regimen. Surgery high-potency glucocorticoid ointment under an occlusive dressing.
or radioiodine may be indicated for severe or relapsing disease. Octreotide may be beneficial in some cases.
Thyrotoxic crisis, or thyroid storm, is rare and presents as a
life-threatening exacerbation of hyperthyroidism, accompanied by ■■OTHER CAUSES OF THYROTOXICOSIS
fever, delirium, seizures, coma, vomiting, diarrhea, and jaundice. Destructive thyroiditis (subacute or silent thyroiditis) typically presents
The mortality rate due to cardiac failure, arrhythmia, or hyper- with a short thyrotoxic phase due to the release of preformed thyroid
thermia is as high as 30%, even with treatment. Thyrotoxic cri- hormones and catabolism of Tg (see “Subacute Thyroiditis,” below).
sis is usually precipitated by acute illness (e.g., stroke, infection, True hyperthyroidism is absent, as demonstrated by a low radionuclide
trauma, diabetic ketoacidosis), surgery (especially on the thyroid), or uptake. Circulating Tg levels are typically increased. Other causes of
radioiodine treatment of a patient with partially treated or untreated thyrotoxicosis with low or absent thyroid radionuclide uptake include
hyperthyroidism. Management requires intensive monitoring and thyrotoxicosis factitia, iodine excess, and, rarely, ectopic thyroid tissue,
supportive care, identification and treatment of the precipitating particularly teratomas of the ovary (struma ovarii) and functional
cause, and measures that reduce thyroid hormone synthesis. Large metastatic follicular carcinoma. Whole-body radionuclide studies can
doses of propylthiouracil (500–1000 mg loading dose and 250 mg demonstrate ectopic thyroid tissue, and thyrotoxicosis factitia can be
every 4 h) should be given orally or by nasogastric tube or per distinguished from destructive thyroiditis by the clinical features and
rectum; the drug’s inhibitory action on T4 → T3 conversion makes low levels of Tg. Amiodarone treatment is associated with thyrotoxico-
it the antithyroid drug of choice. If not available, methimazole can
sis in up to 10% of patients, particularly in areas of low iodine intake
be used in doses of 20 mg every 6 h. One hour after the first dose of
(see below).
Harrisons_20e_Part12_p2649-p3024.indd 2707 6/1/18 3:27 PM
2708 TSH-secreting pituitary adenoma is a rare cause of thyrotoxicosis. coxsackie, influenza, adenoviruses, and echoviruses, but attempts to
It is characterized by the presence of an inappropriately normal or identify the virus in an individual patient are often unsuccessful and
increased TSH level in a patient with hyperthyroidism, diffuse goi- do not influence management. The diagnosis of subacute thyroiditis is
ter, and elevated T4 and T3 levels (Chap. 373). Elevated levels of the often overlooked because the symptoms can mimic pharyngitis. The
α-subunit of TSH, released by the TSH-secreting adenoma, support peak incidence occurs at 30–50 years, and women are affected three
this diagnosis, which can be confirmed by demonstrating the pituitary times more frequently than men.
tumor on MRI or CT scan. A combination of transsphenoidal surgery,
sella irradiation, and octreotide may be required to normalize TSH,
Pathophysiology The thyroid shows a characteristic patchy
inflammatory infiltrate with disruption of the thyroid follicles and
because many of these tumors are large and locally invasive at the time
multinucleated giant cells within some follicles. The follicular changes
of diagnosis. Radioiodine or antithyroid drugs can be used to control
progress to granulomas accompanied by fibrosis. Finally, the thyroid
thyrotoxicosis.
returns to normal, usually several months after onset. During the ini-
Thyrotoxicosis caused by toxic MNG and hyperfunctioning solitary
PART 12
tial phase of follicular destruction, there is release of Tg and thyroid
nodules is discussed below.
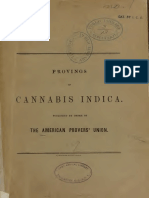
hormones, leading to increased circulating T4 and T3 and suppression
THYROIDITIS of TSH (Fig. 377-3). During this destructive phase, radioactive iodine
A clinically useful classification of thyroiditis is based on the onset and uptake is low or undetectable. After several weeks, the thyroid is
depleted of stored thyroid hormone and a phase of hypothyroidism
Endocrinology and Metabolism
duration of disease (Table 377-3).
typically occurs, with low unbound T4 (and sometimes T3) and moder-
■■ACUTE THYROIDITIS ately increased TSH levels. Radioactive iodine uptake returns to nor-
Acute thyroiditis is rare and due to suppurative infection of the thy- mal or is even increased as a result of the rise in TSH. Finally, thyroid
roid. In children and young adults, the most common cause is the pres- hormone and TSH levels return to normal as the disease subsides.
ence of a piriform sinus, a remnant of the fourth branchial pouch that
Clinical Manifestations The patient usually presents with a
connects the oropharynx with the thyroid. Such sinuses are predomi-
painful and enlarged thyroid, sometimes accompanied by fever. There
nantly left-sided. A long-standing goiter and degeneration in a thyroid
may be features of thyrotoxicosis or hypothyroidism, depending on
malignancy are risk factors in the elderly. The patient presents with
the phase of the illness. Malaise and symptoms of an upper respiratory
thyroid pain, often referred to the throat or ears, and a small, tender
tract infection may precede the thyroid-related features by several
goiter that may be asymmetric. Fever, dysphagia, and erythema over
weeks. In other patients, the onset is acute, severe, and without obvious
the thyroid are common, as are systemic symptoms of a febrile illness
antecedent. The patient typically complains of a sore throat, and exami-
and lymphadenopathy.
nation reveals a small goiter that is exquisitely tender. Pain is often
The differential diagnosis of thyroid pain includes subacute or, rarely,
referred to the jaw or ear. Complete resolution is the usual outcome,
chronic thyroiditis; hemorrhage into a cyst; malignancy including
but late-onset permanent hypothyroidism occurs in 15% of cases, par-
lymphoma; and, rarely, amiodarone-induced thyroiditis or amyloi-
ticularly in those with coincidental thyroid autoimmunity. A prolonged
dosis. However, the abrupt presentation and clinical features of acute
course over many months, with one or more relapses, occurs in a small
thyroiditis rarely cause confusion. The erythrocyte sedimentation rate
percentage of patients.
(ESR) and white cell count are usually increased, but thyroid function
is normal. Fine-needle aspiration (FNA) biopsy shows infiltration by Laboratory Evaluation As depicted in Fig. 377-3, thyroid func-
polymorphonuclear leukocytes; culture of the sample can identify tion tests characteristically evolve through three distinct phases over
the organism. Caution is needed in immunocompromised patients about 6 months: (1) thyrotoxic phase, (2) hypothyroid phase, and (3)
as fungal, mycobacterial, or Pneumocystis thyroiditis can occur in this recovery phase. In the thyrotoxic phase, T4 and T3 levels are increased,
setting. Antibiotic treatment is guided initially by Gram stain and, reflecting their discharge from the damaged thyroid cells, and TSH is
subsequently, by cultures of the FNA biopsy. Surgery may be needed suppressed. The T4/T3 ratio is greater than in Graves’ disease or thy-
to drain an abscess, which can be localized by CT scan or ultrasound. roid autonomy, in which T3 is often disproportionately increased. The
Tracheal obstruction, septicemia, retropharyngeal abscess, mediastini- diagnosis is confirmed by a high ESR and low uptake of radioiodine
tis, and jugular venous thrombosis may complicate acute thyroiditis (<5%) or 99mTc pertechnetate (as compared to salivary gland pertech-
but are uncommon with prompt use of antibiotics. netate concentration). The white blood cell count may be increased,
■■SUBACUTE THYROIDITIS
This is also termed de Quervain’s thyroiditis, granulomatous thyroiditis, or 100 40 50
viral thyroiditis. Many viruses have been implicated, including mumps, ESR
TSH
30
TABLE 377-3 Causes of Thyroiditis UT4
5
UT4 (pmol/L)
TSH (mU/L)
ESR (mm/h)
Acute
50 20
Bacterial infection: especially Staphylococcus, Streptococcus, and Enterobacter
Fungal infection: Aspergillus, Candida, Coccidioides, Histoplasma, and
Pneumocystis 10 0.5
Radiation thyroiditis after 131I treatment
Amiodarone (may also be subacute or chronic)
Subacute 0 0 0.01
0 6 12 18
Viral (or granulomatous) thyroiditis Time (weeks)
Silent thyroiditis (including postpartum thyroiditis)
Mycobacterial infection Thyrotoxic Hypothyroid Recovery
Drug induced (interferon, amiodarone) Clinical Phases
Chronic FIGURE 377-3 Clinical course of subacute thyroiditis. The release of thyroid
hormones is initially associated with a thyrotoxic phase and suppressed thyroid-
Autoimmunity: focal thyroiditis, Hashimoto’s thyroiditis, atrophic thyroiditis stimulating hormone (TSH). A hypothyroid phase then ensues, with low T4 and
Riedel’s thyroiditis TSH levels that are initially low but gradually increase. During the recovery phase,
Parasitic thyroiditis: echinococcosis, strongyloidiasis, cysticercosis increased TSH levels combined with resolution of thyroid follicular injury lead to
Traumatic: after palpation normalization of thyroid function, often several months after the beginning of the
illness. ESR, erythrocyte sedimentation rate; UT4, free or unbound T4.
Harrisons_20e_Part12_p2649-p3024.indd 2708 6/1/18 3:27 PM
and thyroid antibodies are negative. If the diagnosis is in doubt, FNA The goiter is hard, nontender, often asymmetric, and fixed, leading 2709
biopsy may be useful, particularly to distinguish unilateral involve- to suspicion of a malignancy. Diagnosis requires open biopsy as FNA
ment from bleeding into a cyst or neoplasm. biopsy is usually inadequate. Treatment is directed to surgical relief of
compressive symptoms. Tamoxifen may also be beneficial. There is an
association between Riedel’s thyroiditis and IgG4-related disease caus-
TREATMENT ing idiopathic fibrosis at other sites (retroperitoneum, mediastinum,
Subacute Thyroiditis biliary tree, lung, and orbit).
Relatively large doses of aspirin (e.g., 600 mg every 4–6 h) or non-
steroidal anti-inflammatory drugs (NSAIDs) are sufficient to control SICK EUTHYROID SYNDROME
symptoms in many cases. If this treatment is inadequate, or if the (NONTHYROIDAL ILLNESS)
CHAPTER 377 Hyperthyroidism
patient has marked local or systemic symptoms, glucocorticoids Any acute, severe illness can cause abnormalities of circulating TSH or
should be given. The usual starting dose is 15–40 mg of prednisone, thyroid hormone levels in the absence of underlying thyroid disease,
depending on severity. The dose is gradually tapered over 6–8 weeks, making these measurements potentially misleading. The major cause
in response to improvement in symptoms and the ESR. If a relapse of these hormonal changes is the release of cytokines such as IL-6.
occurs during glucocorticoid withdrawal, the dosage should be Unless a thyroid disorder is strongly suspected, the routine testing of
increased and then withdrawn more gradually. Thyroid function thyroid function should be avoided in acutely ill patients.
should be monitored every 2–4 weeks using TSH and unbound T4 The most common hormone pattern in sick euthyroid syndrome
levels. Symptoms of thyrotoxicosis improve spontaneously but may (SES), also called nonthyroidal illness (NTI), is a decrease in total and
be ameliorated by β-adrenergic blockers; antithyroid drugs play no unbound T3 levels (low T3 syndrome) with normal levels of T4 and
role in treatment of the thyrotoxic phase. Levothyroxine replacement TSH. The magnitude of the fall in T3 correlates with the severity of the
may be needed if the hypothyroid phase is prolonged, but doses illness. T4 conversion to T3 via peripheral 5′ (outer ring) deiodination is
should be low enough (50–100 μg daily) to allow TSH-mediated impaired, leading to increased reverse T3 (rT3). Since rT3 is metabolized
recovery. by 5′ deiodination, its clearance is also reduced. Thus, decreased clear-
ance rather than increased production is the major basis for increased
■■SILENT THYROIDITIS rT3. Also, T4 is alternately metabolized to the hormonally inactive
Painless thyroiditis, or “silent” thyroiditis, occurs in patients with under- T3 sulfate. It is generally assumed that this low T3 state is adaptive,
lying autoimmune thyroid disease and has a clinical course similar because it can be induced in normal individuals by fasting. Teleologi-
to that of subacute thyroiditis. The condition occurs in up to 5% of cally, the fall in T3 may limit catabolism in starved or ill patients.
women 3–6 months after pregnancy and is then termed postpartum Very sick patients may exhibit a dramatic fall in total T4 and T3
thyroiditis. Typically, patients have a brief phase of thyrotoxicosis last- levels (low T4 syndrome). With decreased tissue perfusion, muscle and
ing 2–4 weeks, followed by hypothyroidism for 4–12 weeks, and then liver expression of the type 3 deiodinase leads to accelerated T4 and
resolution; often, however, only one phase is apparent. The condition T3 metabolism. This state has a poor prognosis. Another key factor in
is associated with the presence of TPO antibodies antepartum, and it is the fall in T4 levels is altered binding to thyroxine-binding globulin
three times more common in women with type 1 diabetes mellitus. As (TBG). The commonly used free T4 assays are subject to artifact when
in subacute thyroiditis, the uptake of 99mTc pertechnetate or radioactive serum binding proteins are low and underestimate the true free T4
iodine is initially suppressed. In addition to the painless goiter, silent level. Fluctuation in TSH levels also creates challenges in the interpre-
thyroiditis can be distinguished from subacute thyroiditis by a normal tation of thyroid function in sick patients. TSH levels may range from
ESR and the presence of TPO antibodies. Glucocorticoid treatment is <0.1 mIU/L in very ill patients, especially with dopamine or glucocor-
not indicated for silent thyroiditis. Severe thyrotoxic symptoms can be ticoid therapy, to >20 mIU/L during the recovery phase of SES. The
managed with a brief course of propranolol, 20–40 mg three or four exact mechanisms underlying the subnormal TSH seen in 10% of sick
times daily. Thyroxine replacement may be needed for the hypothy- patients and the increased TSH seen in 5% remain unclear but may be
roid phase but should be withdrawn after 6–9 months, as recovery is mediated by cytokines including IL-12 and IL-18.
the rule. Annual follow-up thereafter is recommended, because a pro- Any severe illness can induce changes in thyroid hormone levels,
portion of these individuals develop permanent hypothyroidism. The but certain disorders exhibit a distinctive pattern of abnormalities.
condition may recur in subsequent pregnancies. Acute liver disease is associated with an initial rise in total (but not
unbound) T3 and T4 levels due to TBG release; these levels become
■■DRUG-INDUCED THYROIDITIS subnormal with progression to liver failure. A transient increase in total
Patients receiving cytokines, such as IFN-α or IL-2, or tyrosine kinase and unbound T4 levels, usually with a normal T3 level, is seen in 5–30%
inhibitors may develop painless thyroiditis. IFN-α, which is used to of acutely ill psychiatric patients. TSH values may be transiently low,
treat chronic hepatitis B or C and hematologic and skin malignancies, normal, or high in these patients. In the early stage of HIV infection, T3
causes thyroid dysfunction in up to 5% of treated patients. It has been and T4 levels rise, even if there is weight loss. T3 levels fall with progres-
associated with painless thyroiditis, hypothyroidism, and Graves’ sion to AIDS, but TSH usually remains normal. Renal disease is often
disease, and is most common in women with TPO antibodies prior to accompanied by low T3 concentrations, but with normal rather than
treatment. For discussion of amiodarone, see “Amiodarone Effects on increased rT3 levels, due to an unknown factor that increases uptake
Thyroid Function,” below. of rT3 into the liver.
The diagnosis of SES is challenging. Historic information may be
■■CHRONIC THYROIDITIS limited, and patients often have multiple metabolic derangements.
Focal thyroiditis is present in 20–40% of euthyroid autopsy cases and Useful features to consider include previous history of thyroid disease
is associated with serologic evidence of autoimmunity, particularly and thyroid function tests, evaluation of the severity and time course
the presence of TPO antibodies. The most common clinically apparent of the patient’s acute illness, documentation of medications that may
cause of chronic thyroiditis is Hashimoto’s thyroiditis, an autoimmune affect thyroid function or thyroid hormone levels, and measurements
disorder that often presents as a firm or hard goiter of variable size of rT3 together with unbound thyroid hormones and TSH. The diag-
(see above). Riedel’s thyroiditis is a rare disorder that typically occurs in nosis of SES is frequently presumptive, given the clinical context and
middle-aged women. It presents with an insidious, painless goiter with pattern of laboratory values; only resolution of the test results with
local symptoms due to compression of the esophagus, trachea, neck clinical recovery can clearly establish this disorder. Treatment of SES
veins, or recurrent laryngeal nerves. Dense fibrosis disrupts normal with thyroid hormone (T4 and/or T3) is controversial, but most author-
gland architecture and can extend outside the thyroid capsule. Despite ities recommend monitoring the patient’s thyroid function tests during
these extensive histologic changes, thyroid dysfunction is uncommon. recovery, without administering thyroid hormone, unless there is
Harrisons_20e_Part12_p2649-p3024.indd 2709 6/1/18 3:27 PM
2710 historic or clinical evidence suggestive of hypothyroidism. Sufficiently every 6 h, has been used to reduce thyroidal iodide content. Perchlorate
large randomized controlled trials using thyroid hormone are unlikely treatment has been associated with agranulocytosis, although the risk
to resolve this therapeutic controversy in the near future, because clin- appears relatively low with short-term use. Glucocorticoids, as admin-
ical presentations and outcomes are highly variable. istered for subacute thyroiditis, have modest benefit in type 2 AIT.
Lithium blocks thyroid hormone release and can also provide some
AMIODARONE EFFECTS ON THYROID benefit. Near-total thyroidectomy rapidly decreases thyroid hormone
FUNCTION levels and may be the most effective long-term solution if the patient
Amiodarone is a commonly used type III antiarrhythmic agent can undergo the procedure safely.
(Chap. 247). It is structurally related to thyroid hormone and contains
39% iodine by weight. Thus, typical doses of amiodarone (200 mg/d) ■■FURTHER READING
are associated with very high iodine intake, leading to greater than for- Biondi B et al: The 2015 European Thyroid Association Guidelines on
tyfold increases in plasma and urinary iodine levels. Moreover, because diagnosis and treatment of endogenous subclinical hyperthyroidism.
PART 12
amiodarone is stored in adipose tissue, high iodine levels persist for Eur Thyroid J 4:149, 2015.
>6 months after discontinuation of the drug. Amiodarone inhibits De Leo S et al: Hyperthyroidism. Lancet 388:906, 2016.
deiodinase activity, and its metabolites function as weak antagonists Hanley P et al: Thyroid disorders in children and adolescents: A
of thyroid hormone action. Amiodarone has the following effects on review. JAMA Pediatr 170:1008, 2016.
Ross DS et al: 2016 American Thyroid Association guidelines for
Endocrinology and Metabolism
thyroid function: (1) acute, transient suppression of thyroid function;
(2) hypothyroidism in patients susceptible to the inhibitory effects of a diagnosis and management of hyperthyroidism and other causes of
high iodine load; and (3) thyrotoxicosis that may be caused by either thyrotoxicosis. Thyroid 26:1343, 2016.
a Jod-Basedow effect from the iodine load, in the setting of MNG or Wiersinga WM: Advances in treatment of active, moderate-to-severe
incipient Graves’ disease, or a thyroiditis-like condition. Graves’ ophthalmopathy. Lancet Diabetes Endocrinol 5:134, 2017.
The initiation of amiodarone treatment is associated with a tran-
sient decrease of T4 levels, reflecting the inhibitory effect of iodine
378
on T4 release. Soon thereafter, most individuals escape from iodide-
dependent suppression of the thyroid (Wolff-Chaikoff effect), and the Thyroid Nodular Disease
inhibitory effects on deiodinase activity and thyroid hormone receptor
action become predominant. These events lead to the following pattern
and Thyroid Cancer
of thyroid function tests: increased T4, decreased T3, increased rT3, and J. Larry Jameson, Susan J. Mandel,
a transient TSH increase (up to 20 mIU/L). TSH levels normalize or are Anthony P. Weetman
slightly suppressed within 1–3 months.
The incidence of hypothyroidism from amiodarone varies geo-
graphically, apparently correlating with iodine intake. Hypothyroidism
occurs in up to 13% of amiodarone-treated patients in iodine-replete ■■GOITER AND NODULAR THYROID DISEASE
countries, such as the United States, but is less common (<6% inci- Goiter refers to an enlarged thyroid gland. Biosynthetic defects, iodine
dence) in areas of lower iodine intake, such as Italy or Spain. The deficiency, autoimmune disease, and nodular diseases can each lead
pathogenesis appears to involve an inability of the thyroid gland to to goiter, although by different mechanisms. Biosynthetic defects and
escape from the Wolff-Chaikoff effect in autoimmune thyroiditis. Con- iodine deficiency are associated with reduced efficiency of thyroid
sequently, amiodarone-associated hypothyroidism is more common hormone synthesis, leading to increased thyroid-stimulating hormone
in women and individuals with positive TPO antibodies. It is usually (TSH), which stimulates thyroid growth as a compensatory mecha-
unnecessary to discontinue amiodarone for this side effect, because nism to overcome the block in hormone synthesis. Graves’ disease
levothyroxine can be used to normalize thyroid function. TSH levels and Hashimoto’s thyroiditis are also associated with goiter. In Graves’
should be monitored, because T4 levels are often increased for the rea- disease, the goiter results mainly from the TSH-R–mediated effects
sons described above. of thyroid-stimulating immunoglobulins. The goitrous form of
The management of amiodarone-induced thyrotoxicosis (AIT) is Hashimoto’s thyroiditis occurs because of acquired defects in hormone
complicated by the fact that there are different causes of thyrotoxicosis synthesis, leading to elevated levels of TSH and its consequent growth
and because the increased thyroid hormone levels exacerbate underly- effects. Lymphocytic infiltration and immune system–induced growth
ing arrhythmias and coronary artery disease. Amiodarone treatment factors also contribute to thyroid enlargement in Hashimoto’s thyroiditis.
causes thyrotoxicosis in 10% of patients living in areas of low iodine Thyroid nodular disease is characterized by the disordered growth
intake and in 2% of patients in regions of high iodine intake. There of thyroid cells, which can be either hyperplastic or neoplastic. A
are two major forms of AIT, although some patients have features of patient may have a multinodular goiter (MNG) in which thyroid nod-
both. Type 1 AIT is associated with an underlying thyroid abnormal- ules (generally hyperplastic) replace the majority of the normal thyroid
ity (preclinical Graves’ disease or nodular goiter). Thyroid hormone parenchyma; this presentation is more common in areas of borderline
synthesis becomes excessive as a result of increased iodine exposure iodine deficiency. Or, the thyroid gland may be normal in size and
(Jod-Basedow phenomenon). Type 2 AIT occurs in individuals with no contain discrete thyroid nodules. Because the management of goiter
intrinsic thyroid abnormalities and is the result of drug-induced lysoso- depends on the etiology, the detection of thyroid enlargement on phys-
mal activation leading to destructive thyroiditis with histiocyte accu- ical examination should prompt further evaluation to identify its cause.
mulation in the thyroid; the incidence rises as cumulative amiodarone Nodular thyroid disease is common, occurring in about 3–7% of
dosage increases. Mild forms of type 2 AIT can resolve spontaneously adults when assessed by physical examination. Using ultrasound,
or can occasionally lead to hypothyroidism. Color-flow Doppler ultra- nodules are present in up to 50% of adults, with the majority being
sonography shows increased vascularity in type 1 AIT but decreased <1 cm in diameter. Thyroid nodules may be solitary or multiple, and
vascularity in type 2 AIT. Thyroid scintiscans are difficult to interpret in they may be functional or nonfunctional.
this setting because the high endogenous iodine levels diminish tracer ■■DIFFUSE NONTOXIC (SIMPLE) GOITER
uptake. However, the presence of normal or rarely increased uptake
favors type 1 AIT. Etiology and Pathogenesis When diffuse enlargement of the
In AIT, the drug should be stopped, if possible, although this is often thyroid occurs in the absence of nodules and hyperthyroidism, it is
impractical because of the underlying cardiac disorder. Discontinua- referred to as a diffuse nontoxic goiter. This is sometimes called simple
tion of amiodarone will not have an acute effect because of its storage goiter, because of the absence of nodules, or colloid goiter, because of the
and prolonged half-life. High doses of antithyroid drugs can be used presence of uniform follicles that are filled with colloid. Worldwide,
in type 1 AIT but are often ineffective. Potassium perchlorate, 200 mg diffuse goiter is most commonly caused by iodine deficiency and is
Harrisons_20e_Part12_p2649-p3024.indd 2710 6/1/18 3:27 PM
You might also like
- Hypothyroidism: Progressive Weight Gain and Decreased AppetiteDocument5 pagesHypothyroidism: Progressive Weight Gain and Decreased AppetiteKrisianne Mae Lorenzo Francisco100% (2)
- Endocrinology HandbookDocument75 pagesEndocrinology Handbookhirsi200518No ratings yet
- Cowperitis Remedy Characteristics Symptoms Patient Worse by Patient Better by A State of Fear Anxiety Anguish of Mind and BodyDocument5 pagesCowperitis Remedy Characteristics Symptoms Patient Worse by Patient Better by A State of Fear Anxiety Anguish of Mind and Bodymadhavkrishna gargNo ratings yet
- The Homeopathy Handbook For Children Didier Grandgeorge.10732 - 1Document41 pagesThe Homeopathy Handbook For Children Didier Grandgeorge.10732 - 1DrAbhay Meghaji ChhedaNo ratings yet
- Give The Rubrics-Mansoor 1.1Document18 pagesGive The Rubrics-Mansoor 1.1Aditya uniyalNo ratings yet
- Ascendant TableDocument2 pagesAscendant TableToby RoblesNo ratings yet
- Dr.H.O.GUNEWARDENE (Folder)Document38 pagesDr.H.O.GUNEWARDENE (Folder)Ian GardnerNo ratings yet
- Homeopathy For Plants - Yeah, Right!Document22 pagesHomeopathy For Plants - Yeah, Right!Chandrashekhar ShivyogiNo ratings yet
- 100 Drugs by Sayeed FinalDocument108 pages100 Drugs by Sayeed FinalAyeshik ChakrabortyNo ratings yet
- PSORADocument19 pagesPSORAJayesh TalekarNo ratings yet
- Bell A DonaDocument21 pagesBell A Donaarun.saivarajan2917No ratings yet
- Materia Medica Drug List (Old & New Regulations) PDFDocument5 pagesMateria Medica Drug List (Old & New Regulations) PDFSamwellNo ratings yet
- Practical Technique For RepertorizationDocument25 pagesPractical Technique For RepertorizationVryug PatelNo ratings yet
- The Australian Medical JournalDocument33 pagesThe Australian Medical JournalFLoYDBaNN3RNo ratings yet
- Articles of BERRIDGE, Edward WDocument11 pagesArticles of BERRIDGE, Edward WMuhammad Ata Ul MustafaNo ratings yet
- RDocument140 pagesRmessam110No ratings yet
- Clinical Rubrics in BogerDocument2 pagesClinical Rubrics in BogerVirag PatilNo ratings yet
- Spider GroupDocument48 pagesSpider GroupAnjum Abbasi100% (1)
- Bowel Nosode MatrixDocument2 pagesBowel Nosode MatrixN P SinghNo ratings yet
- Gentry RepertoryDocument17 pagesGentry RepertoryMaine LandNo ratings yet
- Repertorial Representation of RanunculaceaeDocument2 pagesRepertorial Representation of RanunculaceaeImran Munir100% (1)
- Anacardiaceae Family Homeopathy Remedies - Homeopathy ResourceDocument8 pagesAnacardiaceae Family Homeopathy Remedies - Homeopathy ResourceMuhammad ArshadNo ratings yet
- Mind.: Lachesis Mutus Bushmaster or Surucucu (Lachesis)Document2 pagesMind.: Lachesis Mutus Bushmaster or Surucucu (Lachesis)TariqMahmoodNo ratings yet
- A Drug-Free Approach To Asperger Syndrome and Autism - Homeopathic Care For Exceptional Kids (PDFDrive)Document224 pagesA Drug-Free Approach To Asperger Syndrome and Autism - Homeopathic Care For Exceptional Kids (PDFDrive)Umm AbdullahNo ratings yet
- Ophthalmic Diseases and Therapeutics PDFDocument373 pagesOphthalmic Diseases and Therapeutics PDFkondababu moyillaNo ratings yet
- A Brief Note On Plants of Medicinal Importance To LivestockDocument84 pagesA Brief Note On Plants of Medicinal Importance To LivestockSunil100% (1)
- Bashirmahmudellias - Blogspot.in-Hepatitis B and Its Permanent Cure With Homeopathic MedicineDocument4 pagesBashirmahmudellias - Blogspot.in-Hepatitis B and Its Permanent Cure With Homeopathic MedicineairtelNo ratings yet
- Pharmacographia IndicaDocument615 pagesPharmacographia IndicaSatish Vaidya100% (1)
- Group of Homeopathy RemediesDocument3 pagesGroup of Homeopathy RemediesAjay IyerNo ratings yet
- PULSATILLA From Materia Medica by James Tyler Kent. Homeopathy - PDFDocument10 pagesPULSATILLA From Materia Medica by James Tyler Kent. Homeopathy - PDFpksNo ratings yet
- CANDO Pillar Audit Check SheetDocument2 pagesCANDO Pillar Audit Check SheetharpreetmuditNo ratings yet
- Role of Homeopathy in Infectious Diseases Rajeev Saxena.03949 - 1contents PDFDocument4 pagesRole of Homeopathy in Infectious Diseases Rajeev Saxena.03949 - 1contents PDFTaani ChakrabortyNo ratings yet
- News - EN Radar Opus UpdateDocument2 pagesNews - EN Radar Opus UpdateghinsavitNo ratings yet
- 04-2552310121752-Sirirat-1 Productivity Improvement Tools & StandardsDocument32 pages04-2552310121752-Sirirat-1 Productivity Improvement Tools & StandardsKampol HarnkittisakulNo ratings yet
- Sayre Materia Medica-6Document79 pagesSayre Materia Medica-6ven_bams5840100% (2)
- Competitive AnalysisDocument8 pagesCompetitive AnalysisJonelle Morris-DawkinsNo ratings yet
- Formica RufaDocument2 pagesFormica Rufanitkol100% (1)
- Hirudo OfficianalisDocument2 pagesHirudo OfficianalisnitkolNo ratings yet
- The Miasms Peter D Drew.01757 - 2Document6 pagesThe Miasms Peter D Drew.01757 - 2Kancharana ManasaNo ratings yet
- Representation of The Planets in Indian Astrology PDFDocument19 pagesRepresentation of The Planets in Indian Astrology PDFcha072No ratings yet
- Group Study MedicineDocument8 pagesGroup Study MedicineRavi ChandarNo ratings yet
- A Case of Hemorrhagic Ovarian Cyst Treated With HomoeopathyDocument4 pagesA Case of Hemorrhagic Ovarian Cyst Treated With HomoeopathyHomoeopathic PulseNo ratings yet
- Hahnemann'S Miasm Theory and Miasm Remedies: Peter MorrellDocument10 pagesHahnemann'S Miasm Theory and Miasm Remedies: Peter MorrellBhaskar DattaNo ratings yet
- The Homeopathic ExaminerDocument575 pagesThe Homeopathic ExaminerMorgan Cabrera0% (1)
- Materia Medica of CañabaisDocument22 pagesMateria Medica of CañabaisMariela AlvarezNo ratings yet
- Nash Leaders in TyphoidDocument25 pagesNash Leaders in TyphoidhompatNo ratings yet
- Flower EncyclopediaDocument26 pagesFlower Encyclopediabadbrad1975No ratings yet
- Brain Tumor CaseDocument9 pagesBrain Tumor CaseDr. Hafiz Shahid HameedNo ratings yet
- Exclusive Interview With Dr. N. C. ChatterjeeDocument5 pagesExclusive Interview With Dr. N. C. ChatterjeeHomoeopathic Pulse100% (1)
- Argentum NitricumDocument7 pagesArgentum NitricumRaveendra MungaraNo ratings yet
- Fluoric Acid Comparison PDFDocument17 pagesFluoric Acid Comparison PDFSurjeet100% (2)
- HeritageDocument116 pagesHeritageVarshaNo ratings yet
- Forskolin HomoeopathicDocument5 pagesForskolin HomoeopathicMiroslav IlicNo ratings yet
- Pulsatilla NigricansDocument20 pagesPulsatilla NigricansastronayanNo ratings yet
- Thyrotoxicosis 2Document7 pagesThyrotoxicosis 2ayuhati siregarNo ratings yet
- Enfermedad Tiroidea AutoinmuneDocument8 pagesEnfermedad Tiroidea AutoinmunemarceloperezrubinNo ratings yet
- Diabetes and Thyroid Disease A Common Association With Clinical ConsequencesDocument4 pagesDiabetes and Thyroid Disease A Common Association With Clinical Consequenceseliana suxoNo ratings yet
- Thyroid-Associated Ophthalmopathy: ReviewDocument12 pagesThyroid-Associated Ophthalmopathy: Reviewkevin_jawanNo ratings yet
- Thyroiditis: Review ArticleDocument10 pagesThyroiditis: Review Articlexander trujilloNo ratings yet
- Seminar: Simone de Leo, Sun Y Lee, Lewis E BravermanDocument13 pagesSeminar: Simone de Leo, Sun Y Lee, Lewis E BravermanJames Cojab SacalNo ratings yet
- Graves' Disease: Graves' Disease Is An Autoimmune Disease Where The Thyroid IsDocument6 pagesGraves' Disease: Graves' Disease Is An Autoimmune Disease Where The Thyroid IsMoof06No ratings yet
- Complementary and Alternative Medical Lab Testing Part 14: ImmunologyFrom EverandComplementary and Alternative Medical Lab Testing Part 14: ImmunologyNo ratings yet
- Near Infrared Therapy-3 PDFDocument6 pagesNear Infrared Therapy-3 PDFCookie Aruj Laguda100% (3)
- Thyroid Function TestsDocument24 pagesThyroid Function Testspavani valluriNo ratings yet
- HypothyroidismDocument10 pagesHypothyroidismRodica GheorghiuNo ratings yet
- Psychoimmunology Essay by DR Romesh Senewiratne-Alagaratnam (MD)Document32 pagesPsychoimmunology Essay by DR Romesh Senewiratne-Alagaratnam (MD)Dr Romesh Arya Chakravarti100% (2)
- Case DDocument7 pagesCase Dqxr.maeNo ratings yet
- Management of Hypothyroidism and Hypothyroxinemia During Pregnancy-AaceDocument8 pagesManagement of Hypothyroidism and Hypothyroxinemia During Pregnancy-Aacegu mail100% (1)
- Patient Type: OPD: TSH Test ReportDocument1 pagePatient Type: OPD: TSH Test ReportVeenu SehrawatNo ratings yet
- St. Attri Public School: "Genes and Genetic Disorders"Document25 pagesSt. Attri Public School: "Genes and Genetic Disorders"Sai PrintersNo ratings yet
- CretinismDocument9 pagesCretinismBrendan chukwunonsoNo ratings yet
- Pathogenesis of Hyperthyroidism: Diffuse Toxic Goiter (Grave's Disease) Autoimmune Condition Secodary ToDocument6 pagesPathogenesis of Hyperthyroidism: Diffuse Toxic Goiter (Grave's Disease) Autoimmune Condition Secodary ToronaNo ratings yet
- Protocol For Congenital HypothyroidismDocument1 pageProtocol For Congenital HypothyroidismAgnimitra ChoudhuryNo ratings yet
- Family Medicine Case FilesDocument44 pagesFamily Medicine Case FilesTazan VoNo ratings yet
- Suguna LabDocument3 pagesSuguna LabSuguna LabsNo ratings yet
- Hypothyroidism and Pregnancy Vol.2Document9 pagesHypothyroidism and Pregnancy Vol.2RakhiNo ratings yet
- Hara Diagnosis 2015Document38 pagesHara Diagnosis 2015nepretip100% (1)
- PROPYLTHIOURACILDocument35 pagesPROPYLTHIOURACILMagdy Ali ELsherbenyNo ratings yet
- Prof Banundari - Endocrinology Update Jogja FinalDocument78 pagesProf Banundari - Endocrinology Update Jogja FinalEldo TaufilaNo ratings yet
- DishormogénesisDocument28 pagesDishormogénesisFrank BermudezNo ratings yet
- Alsangedy Bullets For Paces: AcromegalyDocument20 pagesAlsangedy Bullets For Paces: AcromegalyIgor BatistaNo ratings yet
- Ak 17121723Document1 pageAk 17121723raghavremNo ratings yet
- Medical Record Summary Template (Disability)Document17 pagesMedical Record Summary Template (Disability)Alipit Jr. D. ArmanNo ratings yet
- Causes of Endocrine DisordersDocument8 pagesCauses of Endocrine DisordersKrystel Mae GarciaNo ratings yet
- Neuro General Neuro: Proptosis/ Exophthalmos ChemosisDocument4 pagesNeuro General Neuro: Proptosis/ Exophthalmos ChemosisShakina FareedNo ratings yet
- MCQs Endo FinalDocument6 pagesMCQs Endo Finalhassan qureshiNo ratings yet
- Care of Adults 26 Endocrine ManagementDocument26 pagesCare of Adults 26 Endocrine ManagementGaras AnnaBerniceNo ratings yet
- Under The Guidance Of:: Dr. Sandeep Tandon Professor and Head of Dept. of PedodonticsDocument79 pagesUnder The Guidance Of:: Dr. Sandeep Tandon Professor and Head of Dept. of PedodonticsMarivic DianoNo ratings yet
- Hormones and Related DrugsDocument42 pagesHormones and Related DrugsRamya PrabhuNo ratings yet
- UWorld Step 3 DARKDocument43 pagesUWorld Step 3 DARKfreddawes100% (2)