You might also like
- Thyroid Hormones & DrugsDocument51 pagesThyroid Hormones & DrugsSUTHANNo ratings yet
- Anticoagulants Drug TableDocument1 pageAnticoagulants Drug TableNicole HoNo ratings yet
- Endocrine 160110083024Document65 pagesEndocrine 160110083024Ryan CracknellNo ratings yet
- Hypothyroidism in PregnancyDocument14 pagesHypothyroidism in PregnancyShajia ZafarNo ratings yet
- Hypothyroid in Pregnancy Andi CakraDocument32 pagesHypothyroid in Pregnancy Andi CakraCakraEkkyNo ratings yet
- Thyroid and InfertilityDocument36 pagesThyroid and InfertilitySairindri SahooNo ratings yet
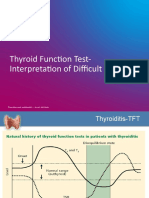
- TFT Interpretation of Difficult CasesDocument51 pagesTFT Interpretation of Difficult CasesAditya GautamNo ratings yet
- Pharmacology Notes (Chapter 20 and 21)Document2 pagesPharmacology Notes (Chapter 20 and 21)graycorypNo ratings yet
- Hyperthyroidsm: EpidemiologyDocument6 pagesHyperthyroidsm: EpidemiologyEllieNo ratings yet
- Gds137 Slide HyperthyroidismDocument30 pagesGds137 Slide HyperthyroidismLouie Kem Anthony BabaranNo ratings yet
- Side EffectsDocument2 pagesSide EffectsFahad AlkenaniNo ratings yet
- Sem 5/unit-3 Autocoids & Related DrugsDocument28 pagesSem 5/unit-3 Autocoids & Related DrugsDARSHAN BhirudNo ratings yet
- Thyroid DisordersDocument67 pagesThyroid DisordersMA 09No ratings yet
- Thyroid PathophysiologyDocument7 pagesThyroid PathophysiologyS RiarNo ratings yet
- (Pha) Le 5Document19 pages(Pha) Le 5Gabby TanNo ratings yet
- Drugs For Heart Failure: Drugs Catego Ry Drug Function Adverse Effect NoteDocument2 pagesDrugs For Heart Failure: Drugs Catego Ry Drug Function Adverse Effect NoteyukariNo ratings yet
- Abnormal Thyroid Function in PregnancyDocument54 pagesAbnormal Thyroid Function in Pregnancyasri khazaliNo ratings yet
- Lecture 29 30 Thyroid TherapeuticsDocument3 pagesLecture 29 30 Thyroid TherapeuticsAhmed MashalyNo ratings yet
- Graves' Hyperthyroidism in Pregnancy: A Clinical ReviewDocument22 pagesGraves' Hyperthyroidism in Pregnancy: A Clinical ReviewAnisa Dinda NurlianaNo ratings yet
- Pharmacology of Alcohol Management of Chronic Alcoholism Treatment of Alcoholic Liver DiseasesDocument41 pagesPharmacology of Alcohol Management of Chronic Alcoholism Treatment of Alcoholic Liver DiseasesVarsha Shende Khobragade100% (2)
- Calcium Metabolism (Pharmacology)Document28 pagesCalcium Metabolism (Pharmacology)Dr.U.P.Rathnakar.MD.DIH.PGDHMNo ratings yet
- Thyroid DX PXLDocument62 pagesThyroid DX PXLabduljebarNo ratings yet
- Therapeutics: Thyroid DisordersDocument24 pagesTherapeutics: Thyroid DisordersSharas FarhadNo ratings yet
- TB TreatmentDocument58 pagesTB TreatmentNdayisaba CorneilleNo ratings yet
- Antihyperglycemic Agents Comparison Chart PDFDocument9 pagesAntihyperglycemic Agents Comparison Chart PDFconcoz100% (1)
- Anti HypertensivesDocument15 pagesAnti HypertensivesFaye MillanesNo ratings yet
- Therapeutic IndexDocument8 pagesTherapeutic IndexMary Jennel RosNo ratings yet
- Pathophysiology of Endocrine SystemDocument64 pagesPathophysiology of Endocrine SystemTess MohamedNo ratings yet
- Thyroid Disorders During PregnancyDocument25 pagesThyroid Disorders During PregnancyA.H.ANo ratings yet
- Drug Recommendation GuideDocument6 pagesDrug Recommendation GuideGenNo ratings yet
- List of Look-Alike MedicationsDocument5 pagesList of Look-Alike MedicationsAhmad TaramsyNo ratings yet
- 34 Drugs Used in Coagulation and Bleeding DisordersDocument94 pages34 Drugs Used in Coagulation and Bleeding DisordersJeanneNo ratings yet
- Drug Interactions: What Is An Interaction?Document4 pagesDrug Interactions: What Is An Interaction?Leyla MajundaNo ratings yet
- Week 3 Pharmaco Part 2Document34 pagesWeek 3 Pharmaco Part 2Tiko JomidavaNo ratings yet
- Pharmacology of HypertensionDocument4 pagesPharmacology of HypertensionFlower100% (1)
- Anti-Gout DrugsDocument38 pagesAnti-Gout Drugsapi-306036754No ratings yet
- Biol 460 Case StudyDocument11 pagesBiol 460 Case Studyapi-353888678No ratings yet
- Anti-Depressant: Mohd Fikry Bin Mohamad Tahir (Student)Document19 pagesAnti-Depressant: Mohd Fikry Bin Mohamad Tahir (Student)fahmiNo ratings yet
- 3 Treatment of HypertensionDocument7 pages3 Treatment of HypertensiontiaraNo ratings yet
- Review Handouts For Medical Pharmacology: Terriann Crisp, PH.DDocument28 pagesReview Handouts For Medical Pharmacology: Terriann Crisp, PH.Dmus zaharaNo ratings yet
- FunctionTests Brochure PDFDocument2 pagesFunctionTests Brochure PDFArslan SaleemNo ratings yet
- AntiemeticsDocument25 pagesAntiemeticsPridho GaziansyahNo ratings yet
- Pharmacology Drug ChartDocument50 pagesPharmacology Drug ChartEssentialForLivingNo ratings yet
- Peptic Ulcer Drugs and Pharmcotherapy - DrdhritiDocument60 pagesPeptic Ulcer Drugs and Pharmcotherapy - Drdhritidbrahma100% (2)
- Antihyperglycemic Agents Comparison ChartDocument9 pagesAntihyperglycemic Agents Comparison ChartBonnieNo ratings yet
- Pharmacology of Cardiac Diseases MINEDocument3 pagesPharmacology of Cardiac Diseases MINEMitu Miressa تNo ratings yet
- 8B - Antianginal DrugsDocument70 pages8B - Antianginal Drugslalitrajindolia100% (1)
- Pemeriksaaan Laboratorium Kelainan Thyroid: DR - Budi Dermawan Lubis, SPPK DR - Siti Hajar, M.Ked, SPPKDocument12 pagesPemeriksaaan Laboratorium Kelainan Thyroid: DR - Budi Dermawan Lubis, SPPK DR - Siti Hajar, M.Ked, SPPKBonitavanyNo ratings yet
- Antidepressants: HistoryDocument8 pagesAntidepressants: HistoryTejus Murthy A GNo ratings yet
- NORADRENALINE (Norepinephrine) : Presentation DescriptionDocument3 pagesNORADRENALINE (Norepinephrine) : Presentation DescriptionMutiaraNo ratings yet
- 膚科Document191 pages膚科Sai TaiNo ratings yet
- Pharm C Exam 10 Drug ListDocument2 pagesPharm C Exam 10 Drug ListVokdadaNo ratings yet
- Antimicrobial DrugsDocument11 pagesAntimicrobial DrugsAudhrey BNo ratings yet
- MCQDocument17 pagesMCQpradeephdNo ratings yet
- Diabetes Topic DiscussionDocument9 pagesDiabetes Topic DiscussionSamNo ratings yet
- Anticholinergic DrugsDocument19 pagesAnticholinergic DrugseashshankarNo ratings yet
- HyperthyroidDocument12 pagesHyperthyroidChristine Joy PepitoNo ratings yet
- Clinical Practice Guidelines For Hypothyroidism in Adults: AACE and ATA 2012Document63 pagesClinical Practice Guidelines For Hypothyroidism in Adults: AACE and ATA 2012Nur Rakhma AkmaliaNo ratings yet
- TPO in PregnancyDocument18 pagesTPO in PregnancyRoxana TudorNo ratings yet
- Thyroid Disorders: DR Raghuveer ChoudharyDocument53 pagesThyroid Disorders: DR Raghuveer ChoudharyPhysiology by Dr RaghuveerNo ratings yet
- Frequency Rate of Thyroid DiseaseDocument118 pagesFrequency Rate of Thyroid DiseaseMustafa KhandgawiNo ratings yet
- Feedback Mechanism: Positive FeedbackDocument17 pagesFeedback Mechanism: Positive FeedbackJanielle Medina FajardoNo ratings yet
- Chapter 18 Endocrine SystemDocument40 pagesChapter 18 Endocrine SystemlolasparkleNo ratings yet
- Hyper Guidelines 2011Document65 pagesHyper Guidelines 2011wrocha2000No ratings yet
- Deepika.R:::: Patient Age / Sex 26 Y / Female BranchDocument2 pagesDeepika.R:::: Patient Age / Sex 26 Y / Female BranchkannanNo ratings yet
- Drugs Affecting The Endocrine SystemDocument76 pagesDrugs Affecting The Endocrine SystemClaudette Talamera CormaryNo ratings yet
- Diagnosis of HyperthyroidismDocument25 pagesDiagnosis of HyperthyroidismGuardito PequeñoNo ratings yet
- Chapter 16 The Endocrine System Chapter OutlineDocument23 pagesChapter 16 The Endocrine System Chapter OutlineMartina MicicNo ratings yet
- Endo Lect-2 Hypothalamus and Pituitary GlandDocument21 pagesEndo Lect-2 Hypothalamus and Pituitary GlanddoctorrfarrukhNo ratings yet
- Short Stature PDFDocument17 pagesShort Stature PDFNiranjan Hegde100% (1)
- Thyroid Disorders in Pregnancy FinalDocument60 pagesThyroid Disorders in Pregnancy Finalmonica caballes100% (1)
- Impact of Thyroid Hormone Dysfunction On Periodontal DiseaseDocument5 pagesImpact of Thyroid Hormone Dysfunction On Periodontal DiseaseNike WijayaNo ratings yet
- Hypothyroidism: Brief Definition Prevalence Risk FactorsDocument8 pagesHypothyroidism: Brief Definition Prevalence Risk FactorsJennifer BeguinwaNo ratings yet
- 3.3 Fertility TestingDocument57 pages3.3 Fertility Testing21 - Tuazon, AlliahNo ratings yet
- Radioactive Iodine 131Document4 pagesRadioactive Iodine 131Kamila Furqani DjibranNo ratings yet
- Hematology TestsDocument7 pagesHematology TestsVenkatesan VidhyaNo ratings yet
- TSH Accubind Elisa Rev 3Document0 pagesTSH Accubind Elisa Rev 3Rafael ZevallosNo ratings yet
- NCM 103 SyllabusDocument10 pagesNCM 103 SyllabuslouradelNo ratings yet
- H-046-003247-00 TT3 KIT (CLIA) Muti LaguageDocument14 pagesH-046-003247-00 TT3 KIT (CLIA) Muti LaguageSinari AlfatNo ratings yet
- Screening Tests For Thyroid Dysfunction Is TSH SufficientDocument12 pagesScreening Tests For Thyroid Dysfunction Is TSH SufficientGlobal Research and Development ServicesNo ratings yet
- Family Medicine NotesDocument32 pagesFamily Medicine Noteslalee704100% (8)
- H-046-003249-00 TSH (CLIA) English MindrayDocument2 pagesH-046-003249-00 TSH (CLIA) English MindrayТатьяна ИсаеваNo ratings yet
- Graves BrochureDocument2 pagesGraves BrochureSussy ListiarsasihNo ratings yet
- Pediatrics - Endocrine SystemDocument347 pagesPediatrics - Endocrine SystemMNo ratings yet
- Previous Exam by System FullDocument26 pagesPrevious Exam by System FullMostafa Mahmoud ElsebeyNo ratings yet
- Thyroid Gland An Diseases of Thyroid D Gland: Omc LectureDocument59 pagesThyroid Gland An Diseases of Thyroid D Gland: Omc LectureEdward MakemboNo ratings yet
- A Review of Endocrine Disorders in ThalassaemiaDocument10 pagesA Review of Endocrine Disorders in ThalassaemiaNiken RositaNo ratings yet
- Thyroid Function TestDocument2 pagesThyroid Function TestfarazenithNo ratings yet
- Thyroid Disorders Part I Hyperthyroidism Little 2006Document9 pagesThyroid Disorders Part I Hyperthyroidism Little 2006Jing XueNo ratings yet
- Anatomy and Physiology Foundations For The Health Professions 1st Edition Deborah Roiger Solutions Manual DownloadDocument30 pagesAnatomy and Physiology Foundations For The Health Professions 1st Edition Deborah Roiger Solutions Manual DownloadBruce Perkins100% (24)