You might also like
- How To Start Calisthenics Workout - The Beginners Ultimate Calisthenics Workout Plan and Body Building Routine For A Healthy Lifestyle. - D, Fryer (2021)Document33 pagesHow To Start Calisthenics Workout - The Beginners Ultimate Calisthenics Workout Plan and Body Building Routine For A Healthy Lifestyle. - D, Fryer (2021)Gustavo Gonzalez ServaNo ratings yet
- Ucm 423806Document69 pagesUcm 423806Rahman Mukti AjiNo ratings yet
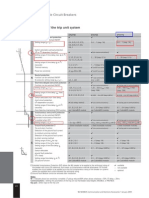
- ETU 776 TripDocument1 pageETU 776 TripbhaskarinvuNo ratings yet
- Standard Operating Procedure: Validation of Heating Ventilation and Air Conditioning (Hvac) SystemDocument20 pagesStandard Operating Procedure: Validation of Heating Ventilation and Air Conditioning (Hvac) SystemMaryanthony Namyalo100% (3)
- Unit 4 - Site PlanningDocument22 pagesUnit 4 - Site PlanningvgdarchNo ratings yet
- Bojar PediatricDocument123 pagesBojar PediatricLuqman AlwiNo ratings yet
- Filter Integrity Test MachineDocument4 pagesFilter Integrity Test MachineAtul SharmaNo ratings yet
- Quality Operating Process: Manual of Operations Care of PatientsDocument4 pagesQuality Operating Process: Manual of Operations Care of PatientsPrabhat KumarNo ratings yet
- ADAB Member List Provides Contact Details for Development OrganizationsDocument8 pagesADAB Member List Provides Contact Details for Development OrganizationsShipon GhoshNo ratings yet
- Water SprayDocument2 pagesWater SpraySaba SamankanNo ratings yet
- Endocarditis in The Elderly: Clinical, Echocardiographic, and Prognostic FeaturesDocument8 pagesEndocarditis in The Elderly: Clinical, Echocardiographic, and Prognostic FeaturesMehdi285858No ratings yet
- OkeeaeDocument6 pagesOkeeaeZulqi SusiloNo ratings yet
- Khan 2023 Outcomes of Surgical Repair of Tetralogy of Fallot child and adultDocument6 pagesKhan 2023 Outcomes of Surgical Repair of Tetralogy of Fallot child and adultElfrida AuliaNo ratings yet
- Prediktor Kegagalan Intervensi Koroner Perkutan Pada Oklusi Total Di Pusat Jantung Nasional, IndonesiaDocument9 pagesPrediktor Kegagalan Intervensi Koroner Perkutan Pada Oklusi Total Di Pusat Jantung Nasional, IndonesiaNining AnjarwatiNo ratings yet
- JET4Document8 pagesJET4fufuka fukalifuNo ratings yet
- Bernard D. Prendergast and Pilar Tornos: Surgery For Infective Endocarditis: Who and When?Document26 pagesBernard D. Prendergast and Pilar Tornos: Surgery For Infective Endocarditis: Who and When?om mkNo ratings yet
- 10 3389@fsurg 2020 00047Document9 pages10 3389@fsurg 2020 00047Hana Nuraisa BasyaNo ratings yet
- Study 3Document7 pagesStudy 3OstazNo ratings yet
- PIIS1078588419310755Document7 pagesPIIS1078588419310755zeeshan qurbanNo ratings yet
- Surgical Outcomes of DVAPTRepairDocument11 pagesSurgical Outcomes of DVAPTRepairJose YoveraNo ratings yet
- Brief Reports: Outcome of Chest Pain Patients Discharged From A French Emergency Department: A 60-Day Prospective StudyDocument4 pagesBrief Reports: Outcome of Chest Pain Patients Discharged From A French Emergency Department: A 60-Day Prospective StudyDiana LoloiuNo ratings yet
- High Lactate Levels Are Predictors of Major Complications After Cardiac SurgeryDocument6 pagesHigh Lactate Levels Are Predictors of Major Complications After Cardiac SurgeryMuhammad RizqiNo ratings yet
- Short - and Long-Term Outcomes at A Single InstitutionDocument7 pagesShort - and Long-Term Outcomes at A Single InstitutionJonathan Frimpong AnsahNo ratings yet
- Atm 08 23 1626Document12 pagesAtm 08 23 1626Susana MalleaNo ratings yet
- 70-Article Text-127-2-10-20200403Document7 pages70-Article Text-127-2-10-20200403rifalNo ratings yet
- Diagnostic Value of Three Dimensional EchocardiogrDocument3 pagesDiagnostic Value of Three Dimensional EchocardiogrAmilkar VazquezNo ratings yet
- DownloadDocument6 pagesDownloadDoraNo ratings yet
- Total Anomalous Pulmonary Venous Drainage Repair: Redefining The Long-Term ExpectationsDocument4 pagesTotal Anomalous Pulmonary Venous Drainage Repair: Redefining The Long-Term Expectationswiyay34652ceoshubcomNo ratings yet
- cimitarraDocument7 pagescimitarracindy beltranNo ratings yet
- Late Surgical Treatment of Tetralogy of FallotDocument3 pagesLate Surgical Treatment of Tetralogy of FallotBryan NguyenNo ratings yet
- Article - Surgical Management of Infective Endocarditis - Early Predictors of Short-Term Morbidity and MortalityDocument6 pagesArticle - Surgical Management of Infective Endocarditis - Early Predictors of Short-Term Morbidity and Mortalityfluid_man_brazilNo ratings yet
- Castle AfDocument11 pagesCastle AfgustavoNo ratings yet
- Improvement After Surgical Closure of Secundum Atrial Septal Defects in Adults 2155 9880 1000493Document7 pagesImprovement After Surgical Closure of Secundum Atrial Septal Defects in Adults 2155 9880 1000493Riani NazilaNo ratings yet
- Jurnal THTDocument3 pagesJurnal THTValentina AdindaNo ratings yet
- Mawaqit Makani, Ndaru Setyaningrum : Corresponding Author. Email: Ndaru - Setyaningrum@uii - Ac.idDocument12 pagesMawaqit Makani, Ndaru Setyaningrum : Corresponding Author. Email: Ndaru - Setyaningrum@uii - Ac.idGita wulandariNo ratings yet
- Articulo Referencia CX EndovadcularDocument7 pagesArticulo Referencia CX EndovadcularGabriel Santiago Cano PerdomoNo ratings yet
- Tga Jurnal NcbiDocument30 pagesTga Jurnal NcbiMYMANo ratings yet
- Catheter Ablationin in AF With CHFDocument11 pagesCatheter Ablationin in AF With CHFKristian Sudana HartantoNo ratings yet
- DIAB10.1002@ccd.28194 4Document9 pagesDIAB10.1002@ccd.28194 4marsim92No ratings yet
- Elaxim ResearchDocument6 pagesElaxim ResearchMayukh BanerjeeNo ratings yet
- Early and Late Results of The Modified Fontan Operation For Heterotaxy SyndromeDocument5 pagesEarly and Late Results of The Modified Fontan Operation For Heterotaxy SyndromeJacob Trisusilo SaleanNo ratings yet
- Long-Term Outcomes of Patients With Tetralogy of Fallot Repaired in Young Infants and ToddlersDocument8 pagesLong-Term Outcomes of Patients With Tetralogy of Fallot Repaired in Young Infants and ToddlersResiden KardiologiNo ratings yet
- Articulo VMDocument8 pagesArticulo VMapi-629928343No ratings yet
- Carotid UltrasoundDocument9 pagesCarotid UltrasoundLora LefterovaNo ratings yet
- Early and Late Postoperative Tachyarrhythmias in Children and Young Adults Undergoing Congenital Heart Disease SurgeryDocument13 pagesEarly and Late Postoperative Tachyarrhythmias in Children and Young Adults Undergoing Congenital Heart Disease SurgeryYar ZepolNo ratings yet
- Pediatr Transplant 2016 Pundi - 1Document6 pagesPediatr Transplant 2016 Pundi - 1bm1No ratings yet
- TurkeyGMJ 62 200 enDocument6 pagesTurkeyGMJ 62 200 enCocoNo ratings yet
- Hema Gayathri Arunachalam, Et AlDocument8 pagesHema Gayathri Arunachalam, Et Aluswatun khasanahNo ratings yet
- Korean QX Total Pulm Veins 2010Document5 pagesKorean QX Total Pulm Veins 2010Dr. LicónNo ratings yet
- CIRCULATIONAHA. Incidence, Management, and Immediate- and Long-Term Outcomes After Iatrogenic Aortic Dissection DuringDocument6 pagesCIRCULATIONAHA. Incidence, Management, and Immediate- and Long-Term Outcomes After Iatrogenic Aortic Dissection DuringSajjad HussainNo ratings yet
- IE New 1Document5 pagesIE New 1Kelik WagiyantoNo ratings yet
- Red Cell Distribution Width Is Associated With Acute Myocardial Infarction in Young PatientsDocument6 pagesRed Cell Distribution Width Is Associated With Acute Myocardial Infarction in Young PatientsMentari FaisalNo ratings yet
- Nejmoa 2026141Document14 pagesNejmoa 2026141Matheus FelipeNo ratings yet
- PreventDocument14 pagesPreventfelipeNo ratings yet
- Anesthesia For Major Surgery in NeonatesDocument18 pagesAnesthesia For Major Surgery in NeonatesfulkifadhilaNo ratings yet
- Cardiac Interventions in Neonates WiDocument11 pagesCardiac Interventions in Neonates WiimNo ratings yet
- Nihms 979441Document33 pagesNihms 979441infatuatingsweetserenadeNo ratings yet
- Pi Is 0007091217540015Document10 pagesPi Is 0007091217540015Yoga WibowoNo ratings yet
- Art TaaDocument7 pagesArt TaaCristinaNo ratings yet
- Nennyelyaniginting,+7 +Yoani+Maria+Vianney+Bita+AtyDocument10 pagesNennyelyaniginting,+7 +Yoani+Maria+Vianney+Bita+AtyBayu IsmoyoNo ratings yet
- CourageDocument14 pagesCourageSuryaNo ratings yet
- Outcomes of Cardiopulmonary Resuscitation in The Emergency DepartmentDocument4 pagesOutcomes of Cardiopulmonary Resuscitation in The Emergency DepartmentSteve aokiNo ratings yet
- Management of Penetrating Wounds of The HeartDocument2 pagesManagement of Penetrating Wounds of The HeartInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- E2 Journal of Hypertension Vol 35, E-Supplement 3, November 2017Document1 pageE2 Journal of Hypertension Vol 35, E-Supplement 3, November 2017Sadam_fasterNo ratings yet
- Follow-Up Transcatheter Closure of Atrial Septal Defect in Young Children: Results andDocument7 pagesFollow-Up Transcatheter Closure of Atrial Septal Defect in Young Children: Results andKholid KuNo ratings yet
- A Minimalistic Approach of Device Closure of Atrial Septal Defect: Analysis of Cases Over Five YearsDocument10 pagesA Minimalistic Approach of Device Closure of Atrial Septal Defect: Analysis of Cases Over Five YearsajmrdNo ratings yet
- New Prognostic Classification and Managements in Infants With Esophageal AtresiaDocument8 pagesNew Prognostic Classification and Managements in Infants With Esophageal AtresiaAnisa GayatriNo ratings yet
- Cardaic ResynchronizationDocument11 pagesCardaic ResynchronizationSamatha BiotechNo ratings yet
- HHS Public Access: The Use of Del Nido Cardioplegia in Adult Cardiac Surgery: A Prospective Randomized TrialDocument18 pagesHHS Public Access: The Use of Del Nido Cardioplegia in Adult Cardiac Surgery: A Prospective Randomized Trialcem berkay duranNo ratings yet
- Critical Care for Potential Liver Transplant CandidatesFrom EverandCritical Care for Potential Liver Transplant CandidatesDmitri BezinoverNo ratings yet
- 03 TOEFL ITP BYOP Test Taker Procedures FinalDocument20 pages03 TOEFL ITP BYOP Test Taker Procedures FinalAmilia DeviNo ratings yet
- Pulmonary Function TestDocument39 pagesPulmonary Function TestLuqman AlwiNo ratings yet
- Pulmonary Function TestDocument39 pagesPulmonary Function TestLuqman AlwiNo ratings yet
- Adult Fallot Mortality in IndonesiaDocument6 pagesAdult Fallot Mortality in IndonesiaLuqman AlwiNo ratings yet
- Mitral Valve Repair, How I Teach ItDocument5 pagesMitral Valve Repair, How I Teach ItLuqman AlwiNo ratings yet
- Suture Material LectureDocument35 pagesSuture Material LectureLuqman AlwiNo ratings yet
- Management Arteriosclerosis and ClaudicationDocument41 pagesManagement Arteriosclerosis and ClaudicationLuqman AlwiNo ratings yet
- APACHEIIDocument1 pageAPACHEIIFailasuf WibisonoNo ratings yet
- Manouguian Technique PDFDocument6 pagesManouguian Technique PDFLuqman AlwiNo ratings yet
- Jurnal Mba Sari 1Document44 pagesJurnal Mba Sari 1PitoAdhiNo ratings yet
- AKUT ABDOMEN Rev2Document77 pagesAKUT ABDOMEN Rev2Luqman AlwiNo ratings yet
- VaricoceleDocument14 pagesVaricoceleLuqman AlwiNo ratings yet
- IpssDocument1 pageIpssIka FairuzaNo ratings yet
- Abdominal Wall Defects GuideDocument42 pagesAbdominal Wall Defects GuideLuqman AlwiNo ratings yet
- Surat Perjanjian Non HumanDocument1 pageSurat Perjanjian Non HumanLuqman AlwiNo ratings yet
- Skin Graft and Flap GuideDocument11 pagesSkin Graft and Flap GuideLuqman AlwiNo ratings yet
- The Effect Administration of Phaleria Macrocarpa To Cell Proliferation - JoseDocument19 pagesThe Effect Administration of Phaleria Macrocarpa To Cell Proliferation - JoseLuqman AlwiNo ratings yet
- Hernia of Umbilical Cord: Report of Three Unusual Cases: Ase SeriesDocument4 pagesHernia of Umbilical Cord: Report of Three Unusual Cases: Ase SeriesLuqman AlwiNo ratings yet
- Ethnomusicology in Times of TroubleDocument15 pagesEthnomusicology in Times of TroubleLéo Corrêa BomfimNo ratings yet
- Text CDocument1,100 pagesText CAli NofalNo ratings yet
- Common Admission Test (CAT) 2020 Admit Card: BarcodeDocument2 pagesCommon Admission Test (CAT) 2020 Admit Card: BarcodeViraaj ThakurNo ratings yet
- Journal Review - Philosophical and Contextual Issue in Nursing Theory DevelopmentDocument4 pagesJournal Review - Philosophical and Contextual Issue in Nursing Theory DevelopmentJULIE ANN PARANo ratings yet
- Argumentative Essay-Nursing HomesDocument1 pageArgumentative Essay-Nursing HomesHM TanNo ratings yet
- Observation of Unknown SpectrumDocument3 pagesObservation of Unknown SpectrumOmar HusseinNo ratings yet
- Concrete Exposures ClassesDocument4 pagesConcrete Exposures ClasseshamidkarimpourNo ratings yet
- UG TRB Physical Education Study MaterialDocument17 pagesUG TRB Physical Education Study Materialசண்முக சுந்தரம் குருசாமி100% (2)
- Comparative Study of Soaps of Hul P Amp G Godrej Nirma and Johnson Amp Johnson 130410234307 Phpapp01 PDFDocument71 pagesComparative Study of Soaps of Hul P Amp G Godrej Nirma and Johnson Amp Johnson 130410234307 Phpapp01 PDFdheeraj agarwalNo ratings yet
- Product Data Sheet GC 120 LDocument5 pagesProduct Data Sheet GC 120 LYohanes Meinata PermanaNo ratings yet
- Breast CancerDocument1 pageBreast CancerAdang FirmansyahNo ratings yet
- Chapter 1 F&B ManagementDocument59 pagesChapter 1 F&B ManagementMohd Faizal Bin AyobNo ratings yet
- Instructional Materials: For K12Document17 pagesInstructional Materials: For K12Ram Jacob LevitaNo ratings yet
- Effects of Restorative Materials On Dental PulpDocument32 pagesEffects of Restorative Materials On Dental PulpUpasana BhandariNo ratings yet
- Match Jobs Pictures Sentences Verbs Phrases HobbiesDocument4 pagesMatch Jobs Pictures Sentences Verbs Phrases HobbiesJose ArreagaNo ratings yet
- Predictor PlatesDocument40 pagesPredictor PlatesrambabuNo ratings yet
- De Thi Thu Vao 10 Mon Tieng Anh Quan Dong Da Ha NoiDocument5 pagesDe Thi Thu Vao 10 Mon Tieng Anh Quan Dong Da Ha NoiTrang VuongNo ratings yet
- NCM 120Document5 pagesNCM 120Tiffany AdriasNo ratings yet
- Solutions: Key Words and ConceptsDocument4 pagesSolutions: Key Words and ConceptsSamuel Enrique Cano PatocNo ratings yet
- Quality Management System at Pharmaceutical IndustryDocument85 pagesQuality Management System at Pharmaceutical IndustryTissa Novida Aulia ZahraNo ratings yet
- Can You Distinguish Neutral, Formal and Informal Among The Following Groups of WordsDocument3 pagesCan You Distinguish Neutral, Formal and Informal Among The Following Groups of WordsВікторія РудаNo ratings yet
- Joshua Gonzalez - ResumeDocument2 pagesJoshua Gonzalez - Resumeapi-483760707No ratings yet