You might also like
- Am Wise Neuroxen RX Report 260921 - 03.00 PMDocument4 pagesAm Wise Neuroxen RX Report 260921 - 03.00 PMarifpharmjuNo ratings yet
- Week 8Document12 pagesWeek 8arifpharmjuNo ratings yet
- BPH 3206 - Lecture 7 - Pharmacy Law & EthicsDocument14 pagesBPH 3206 - Lecture 7 - Pharmacy Law & EthicsarifpharmjuNo ratings yet
- Budget Approval Format - For Shahinur Akter Payel, LaksamDocument2 pagesBudget Approval Format - For Shahinur Akter Payel, LaksamarifpharmjuNo ratings yet
- Chapter 1 - Introduction - The Nature of Drugs & Amp Drug Development & Amp RegulationDocument27 pagesChapter 1 - Introduction - The Nature of Drugs & Amp Drug Development & Amp RegulationarifpharmjuNo ratings yet
- Cefuroxime & AmoxicillinDocument6 pagesCefuroxime & AmoxicillinarifpharmjuNo ratings yet
- Diazoxide 50mg Tab DCC SummeryDocument1 pageDiazoxide 50mg Tab DCC SummeryarifpharmjuNo ratings yet
- Chapter 1 - Introduction - The Nature of Drugs & Amp Drug Development & Amp RegulationDocument27 pagesChapter 1 - Introduction - The Nature of Drugs & Amp Drug Development & Amp RegulationarifpharmjuNo ratings yet
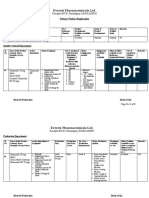
- Primary Product Registration: Butamirate CitrateDocument5 pagesPrimary Product Registration: Butamirate CitratearifpharmjuNo ratings yet
- Mug 10.10 Pm-4lhtyg4kwtghp7xDocument3,135 pagesMug 10.10 Pm-4lhtyg4kwtghp7xarifpharmjuNo ratings yet
- Diazoxide 50mg DatasheetDocument6 pagesDiazoxide 50mg DatasheetarifpharmjuNo ratings yet
- NRG SBRT Physics Nov2016Document19 pagesNRG SBRT Physics Nov2016arifpharmjuNo ratings yet
- Pharmacological Research: SciencedirectDocument20 pagesPharmacological Research: SciencedirectarifpharmjuNo ratings yet
- Diazoxide Recipe Evaluation-1Document2 pagesDiazoxide Recipe Evaluation-1arifpharmjuNo ratings yet
- Molnupiravir 400mg Capsule-RecipeDocument6 pagesMolnupiravir 400mg Capsule-Recipearifpharmju0% (2)
- EASL Clinical Practice Guidelines: Management of Chronic Hepatitis B Virus InfectionDocument19 pagesEASL Clinical Practice Guidelines: Management of Chronic Hepatitis B Virus InfectionarifpharmjuNo ratings yet
- NRG Protocol Radiation Therapy Template: Disease Site: Sub-ComponentDocument11 pagesNRG Protocol Radiation Therapy Template: Disease Site: Sub-ComponentarifpharmjuNo ratings yet
- NRG - ESO - Template - Revised April 2020finalizedDocument15 pagesNRG - ESO - Template - Revised April 2020finalizedarifpharmjuNo ratings yet
- NRG Protocol Radiation Therapy Template - GYN - Endometrial Cancer - FinalDocument12 pagesNRG Protocol Radiation Therapy Template - GYN - Endometrial Cancer - FinalarifpharmjuNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5796)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Mocap 15% Granular Nematicide Insecticide: Restricted Use PesticideDocument15 pagesMocap 15% Granular Nematicide Insecticide: Restricted Use PesticideRayon MorganNo ratings yet
- Constitutionalist: Asa My Concern Is The True Meaning and Application of The ConstitutionDocument15 pagesConstitutionalist: Asa My Concern Is The True Meaning and Application of The ConstitutionGerrit Hendrik Schorel-HlavkaNo ratings yet
- Immature Schistosoma ReflexDocument2 pagesImmature Schistosoma Reflexpramod kumarNo ratings yet
- Darkness Visible: A Memoir of Madness IDocument4 pagesDarkness Visible: A Memoir of Madness ILucas ValdezNo ratings yet
- Metabolic Syndrome Thesis PDFDocument5 pagesMetabolic Syndrome Thesis PDFafknawjof100% (2)
- Health. Survey of The Scene and VictimsDocument27 pagesHealth. Survey of The Scene and VictimsAndrew ZafraNo ratings yet
- Amergy 222 SdsDocument12 pagesAmergy 222 Sdslicentaoffice2021No ratings yet
- Alpha Blockers: Sympatholytic Drugs (Adrenergic Antagonists)Document4 pagesAlpha Blockers: Sympatholytic Drugs (Adrenergic Antagonists)Almabella GecoleNo ratings yet
- Health 8 - 2Q - 2bDocument18 pagesHealth 8 - 2Q - 2bERRALYN PEÑAFLORIDANo ratings yet
- DR Pallab Saha - EA & Public HealthDocument24 pagesDR Pallab Saha - EA & Public HealthDave SenNo ratings yet
- Long COVID or post-COVID-19 Syndrome Putative Pathophysiology, Risk FactorsDocument18 pagesLong COVID or post-COVID-19 Syndrome Putative Pathophysiology, Risk FactorsVane SchulzeNo ratings yet
- Q4 English 8 - Module 3Document31 pagesQ4 English 8 - Module 3Sarahglen Ganob Lumanao100% (1)
- Crimson Contagion 2019 Functional Exercise Draft After-Action Report - October 2019Document63 pagesCrimson Contagion 2019 Functional Exercise Draft After-Action Report - October 2019Eric L. VanDussenNo ratings yet
- Drug StudyDocument1 pageDrug StudyMarichu BajadoNo ratings yet
- Predictors of Unfavorable Treatment Outcome Among Childhood Tuberculosis Patients in Ede Town Health Centers, Sub-District of Osun, NigeriaDocument10 pagesPredictors of Unfavorable Treatment Outcome Among Childhood Tuberculosis Patients in Ede Town Health Centers, Sub-District of Osun, NigeriaInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Benefit of SportDocument6 pagesBenefit of SportNazmi JamilNo ratings yet
- Slaber Jaga Senin 3 Mei 2021Document7 pagesSlaber Jaga Senin 3 Mei 2021Louis MailuhuNo ratings yet
- The Global Deterioration Scale (GDS) For Assessment of Primary Degenerative DementiaDocument2 pagesThe Global Deterioration Scale (GDS) For Assessment of Primary Degenerative DementiaI.m. DanielNo ratings yet
- ThesisofAhmedMusheerAl KhdriDocument159 pagesThesisofAhmedMusheerAl KhdriRex DullitNo ratings yet
- Woodruff CVDocument56 pagesWoodruff CVThe State NewsNo ratings yet
- Sydenham's ChoreaDocument11 pagesSydenham's ChoreaKosi UdohNo ratings yet
- Educational Manual Masterword SCD English FINALDocument111 pagesEducational Manual Masterword SCD English FINALbranchardmushabeNo ratings yet
- Pointers To Review NMC CBTDocument2 pagesPointers To Review NMC CBTLouie Rudolf Kim67% (9)
- Lesson 13 The Aspect of Gene TherapyDocument3 pagesLesson 13 The Aspect of Gene TherapyJamesMarniel AludoNo ratings yet
- Algoritma Handling NyeriDocument21 pagesAlgoritma Handling Nyeriscan resepNo ratings yet
- PreviewDocument37 pagesPreviewDavid Teoh100% (1)
- Humalog Novolog Apidra: Type of Insulin & Brand Names Onset Peak Duration Role in Blood Sugar Management Rapid-ActingDocument2 pagesHumalog Novolog Apidra: Type of Insulin & Brand Names Onset Peak Duration Role in Blood Sugar Management Rapid-ActingkatrinasdNo ratings yet
- EINC - A Step-By-Step GuideDocument41 pagesEINC - A Step-By-Step GuideAlejandro Aricheta91% (11)
- GASTRECTOMYDocument3 pagesGASTRECTOMYMaria Ydela MeradoresNo ratings yet
- Diabetic Ketoacidosis: When To Suspect? How To Confirm?Document5 pagesDiabetic Ketoacidosis: When To Suspect? How To Confirm?Memory LastNo ratings yet