You might also like
- A Model Unit For Grade 2: Canadian Communities: The Canadian Community, Growth and Changes in AnimalsFrom EverandA Model Unit For Grade 2: Canadian Communities: The Canadian Community, Growth and Changes in AnimalsNo ratings yet
- Student-Application-Form CPE Lyon 2022-2023Document4 pagesStudent-Application-Form CPE Lyon 2022-2023Yasser MekhfiNo ratings yet
- A Model Unit For Grade 3: Attracting and Repelling: Connecting with Canadians, Forces That Attract and RepelFrom EverandA Model Unit For Grade 3: Attracting and Repelling: Connecting with Canadians, Forces That Attract and RepelNo ratings yet
- Learning Agreement ApprovalDocument2 pagesLearning Agreement ApprovalSinar Is'haqatNo ratings yet
- Prof Practice-Approval FormDocument2 pagesProf Practice-Approval FormKassadiNo ratings yet
- Lesson PlanDocument17 pagesLesson PlanMarwa ChNo ratings yet
- Prijepis Ocjena - Transcript of RecordsDocument2 pagesPrijepis Ocjena - Transcript of RecordsAlim100% (1)
- Student Application Form: ACADEMIC YEAR 20..... /20..... FIELD OF STUDY:................................................Document4 pagesStudent Application Form: ACADEMIC YEAR 20..... /20..... FIELD OF STUDY:................................................Sidra MuzaffarNo ratings yet
- Application Form For Exchange Students 2015-2016: 1. Home InstitutionDocument6 pagesApplication Form For Exchange Students 2015-2016: 1. Home InstitutionQian BahabobaNo ratings yet
- Cover Letter (For Application Letter) : Pass PhotoDocument3 pagesCover Letter (For Application Letter) : Pass PhotoAhmed ELfarhan Ibn MachRodjiNo ratings yet
- 638201058064118108ta Application FormDocument1 page638201058064118108ta Application FormGiang Nguyễn Thị CẩmNo ratings yet
- Allegato-4 Companyagreementform STUDENTIDocument7 pagesAllegato-4 Companyagreementform STUDENTIJacopo SoraniNo ratings yet
- Bachelor Master Preciosa Learning Agreement Tg2 Tg3Document4 pagesBachelor Master Preciosa Learning Agreement Tg2 Tg3Victor SosaNo ratings yet
- Gurukula Kangri Vishwavidyalaya: HARIDWAR - 249404 (U.K.)Document9 pagesGurukula Kangri Vishwavidyalaya: HARIDWAR - 249404 (U.K.)Deepak SinghalNo ratings yet
- ReceiptPrint UIE-9310 PDFDocument1 pageReceiptPrint UIE-9310 PDFNISHANT3950% (1)
- Form 02 - Thesis Proposal ReviewDocument2 pagesForm 02 - Thesis Proposal ReviewNè GiớpNo ratings yet
- ReceiptPrint_UIE-13703Document1 pageReceiptPrint_UIE-13703ThakurArjunSingh SrinetNo ratings yet
- Gurukula Kangri, HaridwarDocument18 pagesGurukula Kangri, HaridwarShera ThapaNo ratings yet
- Teacher Capacity Application Form 2020 FinalDocument7 pagesTeacher Capacity Application Form 2020 FinalannahmudzaNo ratings yet
- ReceiptPrint UIMTH 54166 4Document1 pageReceiptPrint UIMTH 54166 4Lakita KambojNo ratings yet
- Declaration Forms 2023Document2 pagesDeclaration Forms 2023hljuristsinternationalNo ratings yet
- Erasmus TranscriptDocument2 pagesErasmus TranscriptStrale993No ratings yet
- Ugc - Academic Staff College Pt. Ravishankar Shukla University, RaipurDocument2 pagesUgc - Academic Staff College Pt. Ravishankar Shukla University, RaipurKishori PatelNo ratings yet
- Grading Certificate-1 PDFDocument1 pageGrading Certificate-1 PDFmthabisi nyathiNo ratings yet
- Full Time Post Graduate - Application Form 2024Document4 pagesFull Time Post Graduate - Application Form 2024Young MaxxNo ratings yet
- BVRGA - Application FormDocument5 pagesBVRGA - Application FormNotbotNo ratings yet
- Application Letter & ResumeDocument3 pagesApplication Letter & ResumeAry SetiadiNo ratings yet
- Sastra ApplicationDocument8 pagesSastra ApplicationMaheshSrikakulamNo ratings yet
- Mauritius Local Government Application InsightsDocument6 pagesMauritius Local Government Application InsightsVom Samourais0% (1)
- University Project ProposalDocument5 pagesUniversity Project ProposalOurvashi ChinappenNo ratings yet
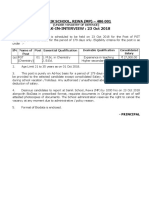
- WALK-IN-INTERVIEW: 23 Oct 2018: Sainik School, Rewa (MP) - 486 001Document3 pagesWALK-IN-INTERVIEW: 23 Oct 2018: Sainik School, Rewa (MP) - 486 001Dr ANIL KandardiyaNo ratings yet
- Student fee receiptDocument1 pageStudent fee receiptHarneet KaurNo ratings yet
- ReceiptPrint UIE-48416Document1 pageReceiptPrint UIE-48416Abhinandan Singh RanaNo ratings yet
- Daily Book 2nd VersionDocument16 pagesDaily Book 2nd VersionForlife StoreNo ratings yet
- GP Personal Details of StudentDocument2 pagesGP Personal Details of StudentNitin malikNo ratings yet
- Student Concession FormDocument1 pageStudent Concession FormAmulya GopalNo ratings yet
- Apply CSSL Student MembershipDocument1 pageApply CSSL Student MembershipRajee ThangenthiranNo ratings yet
- V.B.S. Purvanchal University, Jaunpur (U.P.) - 222203: Application Form For The Teaching PostsDocument14 pagesV.B.S. Purvanchal University, Jaunpur (U.P.) - 222203: Application Form For The Teaching Postsashish7185No ratings yet
- DDE Application 2018Document7 pagesDDE Application 2018ParveenMechNo ratings yet
- Tracer Study Questionnaire: Kgyanwali@tcioe - Edu.npDocument3 pagesTracer Study Questionnaire: Kgyanwali@tcioe - Edu.npKR BhattaNo ratings yet
- Acceptance Form RievyliaDocument2 pagesAcceptance Form RievyliaLenisccy87No ratings yet
- Industrial Training Placement FormDocument1 pageIndustrial Training Placement FormAleeya KamalNo ratings yet
- University of Ibadan Study Leave ApplicationDocument2 pagesUniversity of Ibadan Study Leave ApplicationOlanrewaju AhmedNo ratings yet
- Student hostel fee receiptDocument1 pageStudent hostel fee receiptshubham sahaniNo ratings yet
- HaizaDocument1 pageHaizaHAIZA FATHIMANo ratings yet
- Muhammad Zakri Akmaruddin Bin RidwanDocument1 pageMuhammad Zakri Akmaruddin Bin RidwanSAZALI BIN PATAHIR MoeNo ratings yet
- Utah Math Graduate Bulletin 2013-2014Document68 pagesUtah Math Graduate Bulletin 2013-2014Zia SilverNo ratings yet
- Teachers Contract CollegeDocument5 pagesTeachers Contract CollegeJULIUS ALBAYNo ratings yet
- SBP Merit Scholarship ApplicationDocument1 pageSBP Merit Scholarship ApplicationMasaab KhanNo ratings yet
- Application Form Trainee ProgramDocument4 pagesApplication Form Trainee Programkhoa_hoang_2No ratings yet
- ReceiptPrint_UIE-168414Document1 pageReceiptPrint_UIE-168414keshav popliNo ratings yet
- Print 8607Document31 pagesPrint 8607Zahid ImranNo ratings yet
- ReceiptPrint UIE-56553Document1 pageReceiptPrint UIE-56553Abhinandan Singh RanaNo ratings yet
- Project Proposal Academic Year 2010/2011: Candidate DetailsDocument7 pagesProject Proposal Academic Year 2010/2011: Candidate DetailsAselaJagodaNo ratings yet
- Application Letter & Resume SummaryDocument3 pagesApplication Letter & Resume SummaryRino NovaldoNo ratings yet
- Borang Tambah@Gugur KursusDocument1 pageBorang Tambah@Gugur KursusHaziana HamdanNo ratings yet
- lady shri ram college formDocument5 pageslady shri ram college formkaidogamer686No ratings yet
- Receipt 1Document1 pageReceipt 1kpopli2720No ratings yet
- Application FormDocument4 pagesApplication FormmahalutchmeeluchmunNo ratings yet
- AD Project Log BookDocument4 pagesAD Project Log BookbalqeshhhhNo ratings yet
- Admix Datasheet A4 DynaShearDocument2 pagesAdmix Datasheet A4 DynaShearGilles Roland KamgnoNo ratings yet
- Attestation Niveaux LanguesDocument2 pagesAttestation Niveaux LanguesGilles Roland KamgnoNo ratings yet
- L15 RSInMatlab HandoutDocument13 pagesL15 RSInMatlab HandoutGilles Roland KamgnoNo ratings yet
- GettingStarted en USDocument280 pagesGettingStarted en USDavid MartinNo ratings yet
- PLC WikiDocument2 pagesPLC WikiAdielNo ratings yet
- 3RH19211EA11 Datasheet enDocument4 pages3RH19211EA11 Datasheet enGilles Roland KamgnoNo ratings yet
- SIMATIC Working With Step 7 V5.5, Getting Started - 1Document112 pagesSIMATIC Working With Step 7 V5.5, Getting Started - 1paper2tapeNo ratings yet
- STEP 7 - Programming With STEP 7Document650 pagesSTEP 7 - Programming With STEP 7raveekornov100% (8)
- 6EP13331LD00 Datasheet enDocument3 pages6EP13331LD00 Datasheet enGilles Roland KamgnoNo ratings yet
- 3TY75611AA00 Datasheet enDocument3 pages3TY75611AA00 Datasheet enGilles Roland KamgnoNo ratings yet
- 3RW40361TB04 Datasheet enDocument5 pages3RW40361TB04 Datasheet enGilles Roland KamgnoNo ratings yet
- The Company: Job VacancyDocument2 pagesThe Company: Job VacancyGilles Roland KamgnoNo ratings yet
- Reminders Before Attending Online ClassesDocument13 pagesReminders Before Attending Online ClassesDhianne De GuzmanNo ratings yet
- Activity ED 9-DOLORDocument2 pagesActivity ED 9-DOLORJade DolorNo ratings yet
- "A Detailed Lesson Plan in Field Study 2" Grade and Subject: Grade 8 - English Quarter: Topic: Week: DateDocument8 pages"A Detailed Lesson Plan in Field Study 2" Grade and Subject: Grade 8 - English Quarter: Topic: Week: DateJobert SambitanNo ratings yet
- Unit 7 - WritingDocument13 pagesUnit 7 - WritingTrân HoàngNo ratings yet
- Exploring THE USA - de Cuong Van Hoa Anh MyDocument3 pagesExploring THE USA - de Cuong Van Hoa Anh Mylananh02122004No ratings yet
- MBA International Business Management & Leadership Kempten University of Applied Sciences - Kempten (Allgäu)Document8 pagesMBA International Business Management & Leadership Kempten University of Applied Sciences - Kempten (Allgäu)Hieu NguyenNo ratings yet
- NUS-ISS Short Course Opening ClosingDocument10 pagesNUS-ISS Short Course Opening ClosingslOwpOke13No ratings yet
- Examining Biases in TextDocument2 pagesExamining Biases in TextMaria Angela EduardoNo ratings yet
- MEP Book 1 SupportDocument32 pagesMEP Book 1 SupportElla CelineNo ratings yet
- GSCNHSSHS PR2Q2Mod2Document29 pagesGSCNHSSHS PR2Q2Mod2ROSEMARIE BAYHONNo ratings yet
- RMSA PresentationDocument28 pagesRMSA PresentationRamakrushna MohantyNo ratings yet
- ABP Ananda PDFDocument2 pagesABP Ananda PDFKazi AslamNo ratings yet
- Detech: (BachelorDocument5 pagesDetech: (BachelorVijay AnejaNo ratings yet
- Project Grade 12 Term 2 2024 FinalDocument17 pagesProject Grade 12 Term 2 2024 FinalNwabisa56% (9)
- UNIT 7: Skills Test A: Dictation ListeningDocument5 pagesUNIT 7: Skills Test A: Dictation ListeningAnna KryvkoNo ratings yet
- Directorate of Vocational Education and Training, Maharashtra StateDocument4 pagesDirectorate of Vocational Education and Training, Maharashtra StateAnil KaleNo ratings yet
- Advanced Gunsmithing Course Basic Gun Repair CourseDocument16 pagesAdvanced Gunsmithing Course Basic Gun Repair CourseLuis Otavio TrindadeNo ratings yet
- Application Form For GIIS Singapore ScholarshipDocument3 pagesApplication Form For GIIS Singapore ScholarshipmicrodotcdmNo ratings yet
- Department of Education: Republic of The PhilippinesDocument3 pagesDepartment of Education: Republic of The Philippinesnel baradiNo ratings yet
- Hasil To Perawat 30 Soal 8-7-2021Document36 pagesHasil To Perawat 30 Soal 8-7-2021ayu karimahNo ratings yet
- The Bacolod City College Dedicated to Affordable Quality EducationDocument4 pagesThe Bacolod City College Dedicated to Affordable Quality EducationSchool of Hospitality and Tourism ManagementNo ratings yet
- RPMS TRF T1 To T3Document9 pagesRPMS TRF T1 To T3Arlene ZonioNo ratings yet
- Librarian S Guide To Online Searching 3rd Edition 1Document91 pagesLibrarian S Guide To Online Searching 3rd Edition 1elclareanoNo ratings yet
- DAV-SM Fomra School - KelambakkamDocument4 pagesDAV-SM Fomra School - Kelambakkamsuree1252No ratings yet
- DGT Ministry of Skill Development Demonstration Plan TemplateDocument7 pagesDGT Ministry of Skill Development Demonstration Plan Templaterakesh19865No ratings yet
- Mod Math 4Document24 pagesMod Math 4Ana GolayNo ratings yet
- My Cassanova GangsterDocument454 pagesMy Cassanova GangsterMaria Shiela Mae BaratasNo ratings yet
- LESSON PLAN - Q2 M2 - SANCHEZ JAMES PHILIP L. 1 Checked and Updated RPB 3.01.2021Document8 pagesLESSON PLAN - Q2 M2 - SANCHEZ JAMES PHILIP L. 1 Checked and Updated RPB 3.01.2021Elio SanchezNo ratings yet
- Isd MemoDocument2 pagesIsd Memoapi-528299120No ratings yet
- Janssenville ES supports struggling learners through home visitsDocument2 pagesJanssenville ES supports struggling learners through home visitsJanette BolanteNo ratings yet