You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5806)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (842)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Zoloft Sertraline Drug CardDocument1 pageZoloft Sertraline Drug CardSheri490100% (1)
- Ashton Manual English PDFDocument58 pagesAshton Manual English PDFMalissa Bowen100% (2)
- PharmacotherapyDocument42 pagesPharmacotherapykhalid a.qazi100% (1)
- 21st Indo-US Flow Cytometry Workshop ManualDocument131 pages21st Indo-US Flow Cytometry Workshop ManualSunilkumar ByrnalliNo ratings yet
- EMP2 3 E12630Document25 pagesEMP2 3 E12630Briando Stevano LinelejanNo ratings yet
- ColoproctologyDocument8 pagesColoproctologyBriando Stevano LinelejanNo ratings yet
- Pouches and Stomas: Key PointsDocument6 pagesPouches and Stomas: Key PointsBriando Stevano LinelejanNo ratings yet
- Current Practices in Endotracheal Tube Size Selection For AdultsDocument5 pagesCurrent Practices in Endotracheal Tube Size Selection For AdultsBriando Stevano LinelejanNo ratings yet
- The American Journal of SurgeryDocument6 pagesThe American Journal of SurgeryBriando Stevano LinelejanNo ratings yet
- Contemporary Clinical Trials: SciencedirectDocument6 pagesContemporary Clinical Trials: SciencedirectBriando Stevano LinelejanNo ratings yet
- American Journal of Clinical HypnosisDocument6 pagesAmerican Journal of Clinical HypnosisBriando Stevano LinelejanNo ratings yet
- Navigation-Guided Reduction and Orbital Floor Reconstruction in The Treatment of Zygomatic-Orbital-Maxillary Complex FracturesDocument7 pagesNavigation-Guided Reduction and Orbital Floor Reconstruction in The Treatment of Zygomatic-Orbital-Maxillary Complex FracturesBriando Stevano LinelejanNo ratings yet
- Accepted Manuscript: Clinical NeurophysiologyDocument52 pagesAccepted Manuscript: Clinical NeurophysiologyBriando Stevano LinelejanNo ratings yet
- Humanimmunodeficiency Virusinitialassessmentand Routinefollow-UpDocument16 pagesHumanimmunodeficiency Virusinitialassessmentand Routinefollow-UpBriando Stevano LinelejanNo ratings yet
- Zygomatic Fractures: Classification and Complications: TveterasDocument7 pagesZygomatic Fractures: Classification and Complications: TveterasBriando Stevano LinelejanNo ratings yet
- List of EpidemicsDocument49 pagesList of EpidemicsBriando Stevano LinelejanNo ratings yet
- Evaluation of Treatment of Zygomatic Bone and Zygomatic Arch Fractures: A Retrospective Study of 10 YearsDocument6 pagesEvaluation of Treatment of Zygomatic Bone and Zygomatic Arch Fractures: A Retrospective Study of 10 YearsBriando Stevano LinelejanNo ratings yet
- Abdomen - KLP 10Document33 pagesAbdomen - KLP 10Briando Stevano LinelejanNo ratings yet
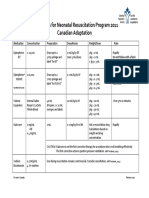
- Medications For Neonatal Resuscitation Program 2011 Canadian AdaptationDocument1 pageMedications For Neonatal Resuscitation Program 2011 Canadian AdaptationrubymayNo ratings yet
- Care For Client With Oxygenation Problem: OutcomesDocument19 pagesCare For Client With Oxygenation Problem: OutcomesPaul JacksonNo ratings yet
- Pathophysiology and Etiology of PCP: HIV InfectionDocument20 pagesPathophysiology and Etiology of PCP: HIV InfectionJehan Sendix100% (1)
- Operating Room Peri Operative Nursing: Are Prepared For Surgery, Undergo Surgical Procedures and RecoverDocument15 pagesOperating Room Peri Operative Nursing: Are Prepared For Surgery, Undergo Surgical Procedures and RecoverRackz Glova AmaroNo ratings yet
- ADV 11-12-15.9-FinalDocument1 pageADV 11-12-15.9-FinalWilliam Floyd School DistrictNo ratings yet
- 3 Giving Suggestion (About Health)Document7 pages3 Giving Suggestion (About Health)Iryana KusumaNo ratings yet
- Lung Cancer (Nursing Care)Document5 pagesLung Cancer (Nursing Care)heiyuNo ratings yet
- Essential Safety Requirements: Security Forces Hospital Program Makkah ESR GuideDocument24 pagesEssential Safety Requirements: Security Forces Hospital Program Makkah ESR GuideGummie Akalal SugalaNo ratings yet
- NCP FractureDocument2 pagesNCP FractureAi Rou100% (1)
- Aninditha. Buku Ajar Neurologi. Jakarta: Departemen Neurologi Fakultas Kedokteran Universitas Indonesia RS Cipto Mangunkusumo. 2017Document2 pagesAninditha. Buku Ajar Neurologi. Jakarta: Departemen Neurologi Fakultas Kedokteran Universitas Indonesia RS Cipto Mangunkusumo. 2017pelangiNo ratings yet
- STRDocument179 pagesSTRJatin AnandNo ratings yet
- RCDSO Guidelines Implant Dentistry PDFDocument16 pagesRCDSO Guidelines Implant Dentistry PDFl4j0b9No ratings yet
- Cenforceshops Com ...Document2 pagesCenforceshops Com ...davidssmith325No ratings yet
- Obstructive Sleep Apnea - An Overview - Prof. Siraj WaliDocument95 pagesObstructive Sleep Apnea - An Overview - Prof. Siraj WaliGhaida AlshehriNo ratings yet
- OSCE ProceduresDocument16 pagesOSCE ProceduresQueen ShNo ratings yet
- Microneedling & Nanopore PresentationDocument58 pagesMicroneedling & Nanopore PresentationkatherineNo ratings yet
- Cardiogenic Shock: BY Dr. M L Patel MD Associate Professor Deptt. of MedicineDocument19 pagesCardiogenic Shock: BY Dr. M L Patel MD Associate Professor Deptt. of MedicineDurgesh PushkarNo ratings yet
- GyN OBS Updated MANAGEMENT PROTOCOL MOHDocument223 pagesGyN OBS Updated MANAGEMENT PROTOCOL MOHyabsera mulatuNo ratings yet
- Exam 1 Outline Notes - Docx NewDocument4 pagesExam 1 Outline Notes - Docx NewHeather MoralesNo ratings yet
- Thyroid NodulesDocument7 pagesThyroid NodulesPravat SatpathyNo ratings yet
- A Study To Assess The Prevalence of TattDocument5 pagesA Study To Assess The Prevalence of Tatt高權梁No ratings yet
- Anatomy of The Coronary Arteries and VeinsDocument80 pagesAnatomy of The Coronary Arteries and Veinstreelife111No ratings yet
- ANESTHESIOLOGY 260 Endorsement PDFDocument4 pagesANESTHESIOLOGY 260 Endorsement PDFEunikaificationNo ratings yet
- Herbalage Products KnowledgeDocument25 pagesHerbalage Products Knowledgemail9246No ratings yet
- ECG QuizDocument3 pagesECG QuizRonnie LimNo ratings yet
- Test Bank For Medical Surgical Nursing 11th Edition Mariann M Harding Jeffrey Kwong Dottie Roberts Debra Hagler Courtney Reinisch DownloadDocument11 pagesTest Bank For Medical Surgical Nursing 11th Edition Mariann M Harding Jeffrey Kwong Dottie Roberts Debra Hagler Courtney Reinisch Downloadjenniferwilliamsonsoefnpykiz100% (23)