You might also like
- Dysphagia Evaluation and Collaborative ManagementDocument10 pagesDysphagia Evaluation and Collaborative ManagementVerry YudhanaNo ratings yet
- Anaerobic Methane Biodigester (Tulum Limpio EN)Document10 pagesAnaerobic Methane Biodigester (Tulum Limpio EN)Antonio Found100% (1)
- En ZRT600 - ZRT850 - 20210913-1 (Icm7100)Document39 pagesEn ZRT600 - ZRT850 - 20210913-1 (Icm7100)Mustafa TamNo ratings yet
- Material Testing 1. Tension TestingDocument5 pagesMaterial Testing 1. Tension TestingcarolineNo ratings yet
- Aseptanios HP 50: Airborne DisinfectantDocument2 pagesAseptanios HP 50: Airborne Disinfectanttantra100% (1)
- Contraindications For ExtractionDocument3 pagesContraindications For ExtractionZhuoYuan How100% (4)
- VW JETTA 2006 - 1.9l Diesel Engine, BRM - Wiring Diagrams, Pin Connector, LocationDocument36 pagesVW JETTA 2006 - 1.9l Diesel Engine, BRM - Wiring Diagrams, Pin Connector, LocationOscar MoralesNo ratings yet
- Gagging Review JPD 2004Document9 pagesGagging Review JPD 2004Pavan PreethamNo ratings yet
- Liposomes 3Document63 pagesLiposomes 3Rohit SardaNo ratings yet
- Soil-Structure Interaction Analysis For Bridge Caisson FoundationDocument10 pagesSoil-Structure Interaction Analysis For Bridge Caisson FoundationarslanpasaNo ratings yet
- The Derivation Formula, Calculus Revision Notes From A-Level Maths TutorDocument4 pagesThe Derivation Formula, Calculus Revision Notes From A-Level Maths TutorA-level Maths TutorNo ratings yet
- Oral HabitsDocument22 pagesOral HabitsZhuoYuan How100% (4)
- Jaw RelationsDocument12 pagesJaw RelationsZhuoYuan HowNo ratings yet
- PMF-015-HSE-120 v2DRAFT HSE Guideline For Construction Sites Manual HandlingDocument14 pagesPMF-015-HSE-120 v2DRAFT HSE Guideline For Construction Sites Manual HandlingmerinofalNo ratings yet
- Dysphagia in The Elderly 2015Document11 pagesDysphagia in The Elderly 2015Nutriologo Luis Garcia CampechanoNo ratings yet
- Dysphagia From A Neurogeriatric Point of ViewDocument6 pagesDysphagia From A Neurogeriatric Point of ViewVanessaCarrilloNo ratings yet
- Etiology and Management of Gag Re Ex in The Prosthodontic Clinic: A ReviewDocument5 pagesEtiology and Management of Gag Re Ex in The Prosthodontic Clinic: A ReviewJavaria IftekharNo ratings yet
- Etiology and Management of Gag Re Ex in The Prosthodontic Clinic: A ReviewDocument5 pagesEtiology and Management of Gag Re Ex in The Prosthodontic Clinic: A ReviewAceNo ratings yet
- Gaggers and Its ManagementDocument58 pagesGaggers and Its ManagementAwani GuptaNo ratings yet
- ART02Document10 pagesART02henry manrriqueNo ratings yet
- 30 - Gag Reflex - Causes and ManagementDocument4 pages30 - Gag Reflex - Causes and ManagementNadiyah Rizqi ANo ratings yet
- Frontal Lobe Epilepsy CasesDocument3 pagesFrontal Lobe Epilepsy CasesGautham sirivallaNo ratings yet
- Gagging Part 1Document6 pagesGagging Part 1Hamad KayaniNo ratings yet
- Gag ReflexDocument5 pagesGag Reflexmfaheemuddin85No ratings yet
- 1.gagging and Its Management in Prosthodontic PatientsDocument25 pages1.gagging and Its Management in Prosthodontic PatientsMithileshwari Patil100% (1)
- Articol 1Document5 pagesArticol 1Oana AsafteiNo ratings yet
- Aga: Clinical Practice UpdateDocument12 pagesAga: Clinical Practice UpdatextineNo ratings yet
- Laryngeal Manifestations of Gastroesophageal Reflux DiseaseDocument7 pagesLaryngeal Manifestations of Gastroesophageal Reflux DiseaseAna BrankovićNo ratings yet
- Oropharyngeal On UGI CGH19Document6 pagesOropharyngeal On UGI CGH19Nikhil BhangaleNo ratings yet
- Adenoid Hypertrophy FixDocument7 pagesAdenoid Hypertrophy FixWidi Yuli HariantoNo ratings yet
- AFP Clinical Nasal ObstructionDocument5 pagesAFP Clinical Nasal ObstructionTri OktarinaNo ratings yet
- Anticholinergic Medication Use Is Associated With Globus Pharyngeus (HAFT 2016)Document5 pagesAnticholinergic Medication Use Is Associated With Globus Pharyngeus (HAFT 2016)DANDYNo ratings yet
- Buccofacial Apraxia, Oropharyngeal Dysphagia, and Dementia Severity in Community-Dwelling Elderly PatientsDocument6 pagesBuccofacial Apraxia, Oropharyngeal Dysphagia, and Dementia Severity in Community-Dwelling Elderly PatientsAashish G. ShresthaNo ratings yet
- 560-Article Text-1066-1-10-20171231 PDFDocument6 pages560-Article Text-1066-1-10-20171231 PDFKrupali JainNo ratings yet
- Original Article: Pedicle Tongue Flap Surgery in Oral Submucous FibrosisDocument4 pagesOriginal Article: Pedicle Tongue Flap Surgery in Oral Submucous FibrosisZuzu FinusNo ratings yet
- GAG ReflexDocument4 pagesGAG Reflexdrgayen6042No ratings yet
- Presentation Chronic AspirationDocument9 pagesPresentation Chronic AspirationTemitope AdeosunNo ratings yet
- Symptoms Dysphagia Neurologically: SignsDocument9 pagesSymptoms Dysphagia Neurologically: SignsmelaniaNo ratings yet
- Brede No Ord 2013Document10 pagesBrede No Ord 2013Jonathan ArifputraNo ratings yet
- Changes in Salivary Flow Rate and PH in Stressful ConditionsDocument6 pagesChanges in Salivary Flow Rate and PH in Stressful ConditionsNgọc Kim Bảo NguyễnNo ratings yet
- Gag PDFDocument6 pagesGag PDFAlka Rose JamesNo ratings yet
- Original Articles: Proton Pump Inhibitor Therapy For Chronic Laryngo-Pharyngitis: A Randomized Placebo-Control TrialDocument9 pagesOriginal Articles: Proton Pump Inhibitor Therapy For Chronic Laryngo-Pharyngitis: A Randomized Placebo-Control TrialAnonymous iM2totBrNo ratings yet
- Oropharyngeal DysphagiaDocument6 pagesOropharyngeal Dysphagianevelle4667No ratings yet
- Gagging: Dr. Sajda A. ElhagDocument41 pagesGagging: Dr. Sajda A. ElhagmarwaNo ratings yet
- Grand Rounds Index UTMB Otolaryngology Home PageDocument12 pagesGrand Rounds Index UTMB Otolaryngology Home Pagegdudex118811No ratings yet
- Imp in Compromised CndnsDocument34 pagesImp in Compromised CndnsswatiNo ratings yet
- Altered LocDocument19 pagesAltered Locgeeeelzy07No ratings yet
- Tutor 7 Blok 9 Skenario 3Document18 pagesTutor 7 Blok 9 Skenario 3Alifa AnatayaNo ratings yet
- Examination of Dental PatientDocument51 pagesExamination of Dental PatientClaritashaAdiendaNo ratings yet
- Laryngopharyngeal Reflux Disease - LPRD: Professional PaperDocument4 pagesLaryngopharyngeal Reflux Disease - LPRD: Professional PaperAndi Tiara S. AdamNo ratings yet
- Sequelae of A Treated Stevens Johnson SyndromeA Case ReportDocument3 pagesSequelae of A Treated Stevens Johnson SyndromeA Case ReportInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Salivary Gland Dysfunction: Etiology, Epidemiology, Clinical Manifestations, Diagnosis, and TreatmentDocument20 pagesSalivary Gland Dysfunction: Etiology, Epidemiology, Clinical Manifestations, Diagnosis, and TreatmentMonaNo ratings yet
- 42 2161 PDFDocument7 pages42 2161 PDFEsha JainNo ratings yet
- Evaluación de La Deglución Con Nasofibroscopía en Pacientes HospitalizadosDocument7 pagesEvaluación de La Deglución Con Nasofibroscopía en Pacientes HospitalizadosDANIELA IGNACIA FERNÁNDEZ LEÓNNo ratings yet
- Accepted Publicationdoes Sphincter Pharyngoplasty Improve Speech Hypernasality in Cleft Patients With Velopharyngeal Incompetence?Document4 pagesAccepted Publicationdoes Sphincter Pharyngoplasty Improve Speech Hypernasality in Cleft Patients With Velopharyngeal Incompetence?basem.t.jamalNo ratings yet
- 10 1002@lary 27106 PDFDocument3 pages10 1002@lary 27106 PDFheltaNo ratings yet
- HIRSCHSPRUNG's DISEASE (Aganglionic Megacolon) Definition Presence of Large, Non-Functional DistalDocument3 pagesHIRSCHSPRUNG's DISEASE (Aganglionic Megacolon) Definition Presence of Large, Non-Functional Distalkhadzx100% (2)
- Videostroboscopy in Laryngopharengeal RefluxDocument5 pagesVideostroboscopy in Laryngopharengeal RefluxLilia ScutelnicNo ratings yet
- Diagnosis and Management of Gastroesophageal Reflux Disease: Dyah Ayu Larasati, S.KedDocument10 pagesDiagnosis and Management of Gastroesophageal Reflux Disease: Dyah Ayu Larasati, S.KedAndhee Whoelank ZiyeangtaecgmhueerymhuerryeNo ratings yet
- Advances in Gerd: Management of Dysphagia in Stroke PatientsDocument3 pagesAdvances in Gerd: Management of Dysphagia in Stroke PatientsFeliciaNo ratings yet
- Investigations For Diseases of The Tongue A Review PDFDocument6 pagesInvestigations For Diseases of The Tongue A Review PDFShantanu DixitNo ratings yet
- Oropharyngeal Dysphagia HNCDocument15 pagesOropharyngeal Dysphagia HNCKhumaira SantaNo ratings yet
- Alam M FakirDocument4 pagesAlam M FakirCut Nanda FitriNo ratings yet
- Alicandri Ciufelli2012Document6 pagesAlicandri Ciufelli2012kraya.sahla.mahlaNo ratings yet
- Why So Many Patients With Dysphagia Have Normal Esophageal Function TestingDocument13 pagesWhy So Many Patients With Dysphagia Have Normal Esophageal Function Testingdraanalordonezv1991No ratings yet
- Adj 12392Document7 pagesAdj 12392Fahad AliNo ratings yet
- Chemotherapy-Associated Oral Sequelae in Patients With Cancers Outside The Head and Neck RegionDocument10 pagesChemotherapy-Associated Oral Sequelae in Patients With Cancers Outside The Head and Neck RegionNndaydnaNo ratings yet
- Background: Reflux LaryngitisDocument5 pagesBackground: Reflux LaryngitisElisa Vina JayantiNo ratings yet
- DentHypotheses6119-844557 232735Document4 pagesDentHypotheses6119-844557 232735JouleAlSBNo ratings yet
- Unit 1 Disorders of Upper Gastrointestinal Tract: StructureDocument18 pagesUnit 1 Disorders of Upper Gastrointestinal Tract: StructureShubhendu ChattopadhyayNo ratings yet
- Management of MicrognathiaDocument9 pagesManagement of MicrognathiaAnnisa SugiyantiNo ratings yet
- Antibiotic Prophylaxis For Infective EndocarditisDocument74 pagesAntibiotic Prophylaxis For Infective EndocarditisZhuoYuan HowNo ratings yet
- Behaviour Science and Its Application in Pediatric DentistryDocument17 pagesBehaviour Science and Its Application in Pediatric DentistryZhuoYuan How0% (1)
- Chapter 5 Perception Ans SensationDocument4 pagesChapter 5 Perception Ans SensationPing Ping TanNo ratings yet
- Ket - Gambar Wiring BOMAKDocument3 pagesKet - Gambar Wiring BOMAKEka SukandaNo ratings yet
- Biocontrol Agents in Co-Inoculation Manages Root Knot Nemtode and Enhances Essential Oil Content in Ocimum Basilicum L.Document10 pagesBiocontrol Agents in Co-Inoculation Manages Root Knot Nemtode and Enhances Essential Oil Content in Ocimum Basilicum L.Belén TapiaNo ratings yet
- FAO: Classification and Illustrated Definition of Fishing GearsDocument110 pagesFAO: Classification and Illustrated Definition of Fishing GearsSapriyun SNo ratings yet
- Arduino ADS1115 Module Getting Started TutorialDocument7 pagesArduino ADS1115 Module Getting Started Tutorialjoeragan 20060% (1)
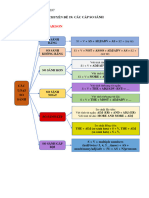
- CHUYÊN ĐỀ 19 - CÁC CẤP SO SÁNH - GRade B1,b2Document10 pagesCHUYÊN ĐỀ 19 - CÁC CẤP SO SÁNH - GRade B1,b2Thành Nam NguyễnNo ratings yet
- Kinship As Logic of SpaceDocument25 pagesKinship As Logic of Spacedorina pllumbiNo ratings yet
- Heart of The Whau - Part 5 The Rise of The Shopping MallDocument25 pagesHeart of The Whau - Part 5 The Rise of The Shopping MallStorm Gerome100% (1)
- Prepared byDocument12 pagesPrepared byaboemadaldeenNo ratings yet
- EcoStruxure Machine ExpertDocument19 pagesEcoStruxure Machine Expertjack.wj86No ratings yet
- The Radiation MechanismDocument2 pagesThe Radiation MechanismKote Bhanu PrakashNo ratings yet
- Vibhor Bishwas 27Document44 pagesVibhor Bishwas 27vibhors751No ratings yet
- Homework 4Document3 pagesHomework 4DavidMuñozNo ratings yet
- New HSK 6 Vocabulary ListDocument44 pagesNew HSK 6 Vocabulary ListValencia AngeliNo ratings yet
- Multi-Storey Steel Building SolutionsDocument16 pagesMulti-Storey Steel Building SolutionsvannethnyNo ratings yet
- Lab Report 1 (E21A0482)Document3 pagesLab Report 1 (E21A0482)Fatihah AlhataNo ratings yet
- Water Resources Planning in HP-1 Karnataka Surface WaterDocument48 pagesWater Resources Planning in HP-1 Karnataka Surface WaterHydrologywebsiteNo ratings yet
- Sergei Bulgakov: Eastern Orthodoxy Engaging The Modern WorldDocument10 pagesSergei Bulgakov: Eastern Orthodoxy Engaging The Modern Worldmatrik88No ratings yet
- Cutler-Hammer ATC400 AG Switch ManualDocument38 pagesCutler-Hammer ATC400 AG Switch ManualTom LeonardNo ratings yet
- Sabine Feedback Exterminator (Power Q ADF4000)Document67 pagesSabine Feedback Exterminator (Power Q ADF4000)Adrian GardnerNo ratings yet