You might also like
- Case Presentation 2Document53 pagesCase Presentation 2Hussain AzharNo ratings yet
- Case Study Presentation On Diabetic Foot UlcerDocument61 pagesCase Study Presentation On Diabetic Foot UlcerBindu GC100% (1)
- Chronic Kidney Disease Case PresentationDocument14 pagesChronic Kidney Disease Case PresentationEmi EspinoNo ratings yet
- Case Study of Renal FailurDocument15 pagesCase Study of Renal FailurYousef Jafar0% (1)
- Diabetes Melitus 2 DkaDocument104 pagesDiabetes Melitus 2 DkaLaiza Fatima LacsonNo ratings yet
- Dyspepsia (Gastritis) Case StudiesDocument9 pagesDyspepsia (Gastritis) Case StudiesJessica Nurin Graman100% (1)
- DM - Case Pres 1aDocument59 pagesDM - Case Pres 1abon clayNo ratings yet
- Case Study DMDocument48 pagesCase Study DMBenj Villanueva100% (1)
- Case Study Liver CirrhosisDocument55 pagesCase Study Liver CirrhosisJoseph Emmanuel CandaNo ratings yet
- A Case Study of Pulmonary TuberculosisDocument28 pagesA Case Study of Pulmonary TuberculosisDyanne BautistaNo ratings yet
- ThalassemiaDocument32 pagesThalassemiaBinal JoshiNo ratings yet
- Case PresentationDocument31 pagesCase PresentationYogaPratayogaMNo ratings yet
- Chronic Renal Failure - Case Study (Group)Document35 pagesChronic Renal Failure - Case Study (Group)Coleen Mae CamaristaNo ratings yet
- Case Study ThyroidectomyDocument8 pagesCase Study Thyroidectomyapi-347153077No ratings yet
- Case Study 1 (Pneumonia)Document13 pagesCase Study 1 (Pneumonia)Kate EscotonNo ratings yet
- Upper Gastrointestinal BleedingDocument69 pagesUpper Gastrointestinal Bleedingeliza luisNo ratings yet
- Individual Case Study Acute GlomerulonephritisDocument26 pagesIndividual Case Study Acute GlomerulonephritisBatrisyia HalimsNo ratings yet
- Case Study OsteoporosisDocument17 pagesCase Study Osteoporosistarikeops50% (2)
- NephrolithiasisDocument87 pagesNephrolithiasissuwash100% (1)
- Chronic Renal FailureDocument28 pagesChronic Renal FailurePatricia Nadine Sarcadio NeffeNo ratings yet
- Case Presentation On Chronic Kidney Disease1Document18 pagesCase Presentation On Chronic Kidney Disease1d100% (1)
- Cholelithiasis Case StudyDocument6 pagesCholelithiasis Case StudySarah DentyNo ratings yet
- Pancreatic CancerDocument15 pagesPancreatic CancerMutiana Muspita JeliNo ratings yet
- Lipoma Excision Care Management GuideDocument56 pagesLipoma Excision Care Management Guideamier_s100% (1)
- Running Head: Acute Pancreatitis 1Document13 pagesRunning Head: Acute Pancreatitis 1Gitonga Moses GitongaNo ratings yet
- How Phototherapy WorksDocument4 pagesHow Phototherapy WorksmaramNo ratings yet
- Case Study (DM)Document28 pagesCase Study (DM)Jai - Ho100% (1)
- Case Study PresentationDocument44 pagesCase Study Presentationapi-31876231450% (2)
- Lived Experiences of Nurses On Nursing Shortage: Basis in Strengthening Nurses' Protection Advocacies and EducationDocument20 pagesLived Experiences of Nurses On Nursing Shortage: Basis in Strengthening Nurses' Protection Advocacies and EducationPsychology and Education: A Multidisciplinary JournalNo ratings yet
- Case Study 18Document4 pagesCase Study 18api-271284613No ratings yet
- Diarrhea: DefinitionDocument13 pagesDiarrhea: Definitionudaybujji100% (1)
- Case StudyDocument49 pagesCase StudyLennie Marie B Pelaez100% (1)
- Macaraig Brillo Final Case Study HypertensionDocument67 pagesMacaraig Brillo Final Case Study HypertensionMarie Kelsey Acena MacaraigNo ratings yet
- Drug Profile - AmantadinDocument14 pagesDrug Profile - AmantadinAna TanNo ratings yet
- Anatomy and Physiology DMDocument3 pagesAnatomy and Physiology DMJisel-Apple Bulan100% (3)
- Diabetes Mellitus Case StudyDocument5 pagesDiabetes Mellitus Case StudyRainier Rhett Concha86% (7)
- Nursing Case AuditDocument53 pagesNursing Case AuditJhean MeansNo ratings yet
- Grand Case PresentationDocument50 pagesGrand Case PresentationJean Michelle100% (1)
- Nursing Care for a Child with Severe Malaria (39 charactersDocument39 pagesNursing Care for a Child with Severe Malaria (39 charactersokelue kingsleyNo ratings yet
- Presentation-on-Long-Case (Retinal Detachment)Document33 pagesPresentation-on-Long-Case (Retinal Detachment)Niloy Basak100% (1)
- Typhoid Fever Case StudyDocument27 pagesTyphoid Fever Case StudyColeen Mae CamaristaNo ratings yet
- Patient ProfileDocument9 pagesPatient ProfileValarmathiNo ratings yet
- Care Plan On: Submitted To: Submitted byDocument38 pagesCare Plan On: Submitted To: Submitted byMoonNo ratings yet
- DM Type II Case StudyDocument28 pagesDM Type II Case StudyRichard Sy67% (3)
- BSN3C 2E Case Presentation On Blunt Abdominal Trauma November 2021Document42 pagesBSN3C 2E Case Presentation On Blunt Abdominal Trauma November 2021Assasination Classroom100% (1)
- Fracture Closed Complete Displaced Middle Third Femur Right Secondary To FallDocument102 pagesFracture Closed Complete Displaced Middle Third Femur Right Secondary To FallRaidis PangilinanNo ratings yet
- Case Study PP - AdhdDocument21 pagesCase Study PP - Adhdapi-482726932100% (1)
- I Patient Assessment Data BaseDocument12 pagesI Patient Assessment Data BaseJanice_Fernand_1603No ratings yet
- Drug StudyDocument10 pagesDrug StudyBandana RajpootNo ratings yet
- CASE Study PTB 2Document53 pagesCASE Study PTB 2Hedda Xyza PascuaNo ratings yet
- Case Study CLD 1Document12 pagesCase Study CLD 1MoonNo ratings yet
- Case Study On Chronic Kidney Disease by G Arunaj From Srilanka BSC in NursingDocument39 pagesCase Study On Chronic Kidney Disease by G Arunaj From Srilanka BSC in NursingKetheesaran LingamNo ratings yet
- Hemorrhoidectomy Case StudyDocument19 pagesHemorrhoidectomy Case StudyJoyJoy Tabada CalunsagNo ratings yet
- Case Study Diabetes MellitusDocument31 pagesCase Study Diabetes Mellitusrmarty_35No ratings yet
- AML Case StudyDocument66 pagesAML Case StudyNoel Christian PeraltaNo ratings yet
- Murari Lal Memorial School and College of Nursing, SolanDocument18 pagesMurari Lal Memorial School and College of Nursing, SolanSimran ChauhanNo ratings yet
- Case Study 2Document27 pagesCase Study 2Hal00mNo ratings yet
- Saint Louis University Nursing Students' Drug StudyDocument7 pagesSaint Louis University Nursing Students' Drug StudyMyraNo ratings yet
- Nursing Care PlanDocument7 pagesNursing Care PlanJane LiNo ratings yet
- Case Study 2Document51 pagesCase Study 2Lilly PattersonNo ratings yet
- Movie AnalysisDocument4 pagesMovie AnalysisMyles Filomeno FieldadNo ratings yet
- Marria NeDocument1 pageMarria NeSanti MooreNo ratings yet
- KetoanaloguesDocument4 pagesKetoanaloguesSanti MooreNo ratings yet
- Assessment Diagnosis Planning Nursing Intervention Rationale EvaluationDocument7 pagesAssessment Diagnosis Planning Nursing Intervention Rationale EvaluationSanti MooreNo ratings yet
- Psychosocial Problems and Self-esteem of Grade 12 StudentsDocument12 pagesPsychosocial Problems and Self-esteem of Grade 12 StudentsSanti MooreNo ratings yet
- Providing Student Support in University DormitoriesDocument10 pagesProviding Student Support in University DormitoriesSanti MooreNo ratings yet
- CHN 3 Action Plan Research TypeDocument5 pagesCHN 3 Action Plan Research TypeSanti MooreNo ratings yet
- Student'S Profile: Juan Dela Cruz BSN Ii-ADocument20 pagesStudent'S Profile: Juan Dela Cruz BSN Ii-ARyrey Abraham PacamanaNo ratings yet
- Planning Intervention Rationale Evaluation: Assessment DiagnosisDocument4 pagesPlanning Intervention Rationale Evaluation: Assessment DiagnosisSanti MooreNo ratings yet
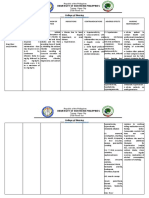
- College of Nursing: University of Northern PhilippinesDocument8 pagesCollege of Nursing: University of Northern PhilippinesSanti MooreNo ratings yet
- How Am I Going To Live An Ethical LifeDocument1 pageHow Am I Going To Live An Ethical LifeSanti MooreNo ratings yet
- Patient'S Data 1. Name of Patient 2. PINDocument4 pagesPatient'S Data 1. Name of Patient 2. PINSanti MooreNo ratings yet
- Celiac DiseaseDocument5 pagesCeliac DiseaseSanti MooreNo ratings yet
- Ethics FieldadDocument2 pagesEthics FieldadSanti MooreNo ratings yet
- Ethics FieldadDocument2 pagesEthics FieldadSanti MooreNo ratings yet
- Disaster Risk Reduction and Management AwarenessDocument39 pagesDisaster Risk Reduction and Management AwarenessSanti Moore100% (1)
- Proper urine collection maximizes lab test diagnosisDocument26 pagesProper urine collection maximizes lab test diagnosisClaryse EroyNo ratings yet
- Autosomal Recessive InheritanceDocument8 pagesAutosomal Recessive InheritanceShatasree MazumdarNo ratings yet
- 273 Health Science 6 12Document47 pages273 Health Science 6 12المعتزبالله جاب اللهNo ratings yet
- K - Birth Plan ChecklistDocument2 pagesK - Birth Plan ChecklistPatrick LinNo ratings yet
- Bwcs Feedback Final September 2023Document56 pagesBwcs Feedback Final September 2023Babloo50% (2)
- Complementary and Alternative MedicineDocument68 pagesComplementary and Alternative MedicineGr3y D3ngu3100% (1)
- Role of Family Planning in Responsible Parent HoodDocument40 pagesRole of Family Planning in Responsible Parent HoodJason Jimmy Lee PillayNo ratings yet
- Social and Behavior Change for Family Planning TrainingDocument166 pagesSocial and Behavior Change for Family Planning TrainingMulugeta DagneNo ratings yet
- Notification: of TheDocument4 pagesNotification: of TheSushma DeviNo ratings yet
- Community-Based Approach For Dengue Prevention and Control in Sta. Cruz, Laguna, PhilippinesDocument7 pagesCommunity-Based Approach For Dengue Prevention and Control in Sta. Cruz, Laguna, PhilippinesBella LifindraNo ratings yet
- Nursing ResponsibilitiesDocument4 pagesNursing ResponsibilitiesMaureen Joy Cascayan EspirituNo ratings yet
- Department of Health - National Practice Standards For The Mental Health Workforce 2013Document1 pageDepartment of Health - National Practice Standards For The Mental Health Workforce 2013catalinauroraNo ratings yet
- BIOL 380 Course OutlineDocument6 pagesBIOL 380 Course OutlineOliverNo ratings yet
- D) Dissociative Identity DisorderDocument4 pagesD) Dissociative Identity DisorderANEESA ANSERNo ratings yet
- Health Benefits of CucumbersDocument6 pagesHealth Benefits of Cucumbersver_at_workNo ratings yet
- Respiratory System Upper Respiratory DiseasesDocument32 pagesRespiratory System Upper Respiratory DiseasesPrince Rener Velasco Pera100% (1)
- Dental Hygiene Resume - No ReferencesDocument2 pagesDental Hygiene Resume - No Referencesapi-313829416No ratings yet
- What Are The Benefits of Family Planning in The PhilippinesDocument2 pagesWhat Are The Benefits of Family Planning in The PhilippinesdodonggwapoNo ratings yet
- Postpartum Care and Breastfeeding GuidanceDocument2 pagesPostpartum Care and Breastfeeding GuidanceArjay EllaNo ratings yet
- Disease Prevention and Control: Dr.K.Arulanandem Lecturer/CoordinatorDocument30 pagesDisease Prevention and Control: Dr.K.Arulanandem Lecturer/Coordinatorv_vijayakanth7656No ratings yet
- Agency ProjectDocument14 pagesAgency Projectapi-304517936No ratings yet
- American Medical AbbreviationDocument11 pagesAmerican Medical AbbreviationJacquelineNo ratings yet
- "Mayroong Namuong Dugo Sa Utak Niya Kaya Hindi Maayos Ang Daloy NG Dugo Rito" As Verbalized by The Patient'sDocument4 pages"Mayroong Namuong Dugo Sa Utak Niya Kaya Hindi Maayos Ang Daloy NG Dugo Rito" As Verbalized by The Patient'sAllisson BeckersNo ratings yet
- Adhd InfographicDocument1 pageAdhd Infographicapi-666361680No ratings yet
- Dakota Horizons BrochureDocument2 pagesDakota Horizons Brochurekatie_krebsbach_1No ratings yet
- Ethical Principle S: Joy Lyzette Reguyal Carreon, RN, ManDocument26 pagesEthical Principle S: Joy Lyzette Reguyal Carreon, RN, ManRomelyn Duque DellomesNo ratings yet
- Biosafety and BiosecurityDocument39 pagesBiosafety and BiosecurityAlliah Angelica NavalNo ratings yet
- Sterility and Its TreaerrrtmentDocument11 pagesSterility and Its TreaerrrtmentFares EL DeenNo ratings yet
- 00 Chest NotesDocument38 pages00 Chest NotesENINE RESTAURANT CompanyNo ratings yet