You might also like
- Ibajay District Hospital Frontline Services GuidePERIOD TOCOVERPERSON TOAPPROACH1 minuteLaboratory Aide5 minutesLaboratory Aide5 minutesCashier10 minutesLab TechnicianDocument22 pagesIbajay District Hospital Frontline Services GuidePERIOD TOCOVERPERSON TOAPPROACH1 minuteLaboratory Aide5 minutesLaboratory Aide5 minutesCashier10 minutesLab TechnicianMary Jean GelitoNo ratings yet
- Adolescent Reproductive HealthDocument218 pagesAdolescent Reproductive HealthMarissa Fontanil100% (1)
- 20 Questions Pulmonology ReviewDocument13 pages20 Questions Pulmonology ReviewSunita Shah0% (1)
- Wilderness First Aid ScenariosDocument6 pagesWilderness First Aid Scenariosapi-545836706No ratings yet
- Summer Training Guide For Pharmacy Students-1Document132 pagesSummer Training Guide For Pharmacy Students-1Rania T. Sabri100% (2)
- PAFP Clinical Pathway For The Diagnosis and Management of Patients With COVID 19 in Family Practice PDFDocument35 pagesPAFP Clinical Pathway For The Diagnosis and Management of Patients With COVID 19 in Family Practice PDFZaqueo Gutierrez FajardoNo ratings yet
- Typhoid Fever and AmoebiasisDocument37 pagesTyphoid Fever and Amoebiasisibnbasheer100% (4)
- A Detailed Lesson Plan in English IV I. ObjectivesDocument8 pagesA Detailed Lesson Plan in English IV I. ObjectivesMontanez Gorre DionvheeNo ratings yet
- 4 GAD MandatesDocument86 pages4 GAD MandatesKristiNo ratings yet
- Post - Natal Case ProformaDocument4 pagesPost - Natal Case Proformakavya sriNo ratings yet
- Report on Earthquake and Fire Drill ConductDocument3 pagesReport on Earthquake and Fire Drill ConductJanet Latorre Tamor100% (1)
- WOMEN AND CHILD PROTECTIONDocument5 pagesWOMEN AND CHILD PROTECTIONMikaela Eris CortelloNo ratings yet
- Policy and Guidelines On Protecting Children in School From Abuse Longos ES 2Document19 pagesPolicy and Guidelines On Protecting Children in School From Abuse Longos ES 2Michael BaltazarNo ratings yet
- Respitide DXM PDFDocument62 pagesRespitide DXM PDFImmanuel Jeffri PaianNo ratings yet
- Asthma and Inhaler 20201203Document29 pagesAsthma and Inhaler 20201203松山內科部No ratings yet
- Asma Gina 2019Document19 pagesAsma Gina 2019ninisNo ratings yet
- Bronchial Asthma: GINA Guidelines 2020Document17 pagesBronchial Asthma: GINA Guidelines 2020The Telugu DoctorNo ratings yet
- Drugs for Pulmonary Disorders 2023Document22 pagesDrugs for Pulmonary Disorders 2023aguilarjanicaNo ratings yet
- Childhood Asthma Diagnosis and TreatmentDocument26 pagesChildhood Asthma Diagnosis and TreatmentShwetika BarmanNo ratings yet
- GINA 2022 Whats New SlidesDocument52 pagesGINA 2022 Whats New SlidesadindaNo ratings yet
- Global Initiative For Asthma (GINA) What's New in GINA 2019?Document32 pagesGlobal Initiative For Asthma (GINA) What's New in GINA 2019?Jamie ParkNo ratings yet
- GINA 2022 Whats New SlidesDocument52 pagesGINA 2022 Whats New SlidesYulia DevinaNo ratings yet
- GINA 2022 Whats New SlidesDocument52 pagesGINA 2022 Whats New Slidesaniqahmed6565No ratings yet
- Paediatric AsthmaDocument3 pagesPaediatric AsthmaDr Roelien JefferysNo ratings yet
- Skema Terapi AsthmaDocument1 pageSkema Terapi AsthmaPaulus AnungNo ratings yet
- DS 2ND SemDocument8 pagesDS 2ND SemRhobic ManansalaNo ratings yet
- Asma 2018Document3 pagesAsma 2018gheaNo ratings yet
- BTS and SIGN Management of Asthma in Adults: Ve Control A S Needed APYDocument1 pageBTS and SIGN Management of Asthma in Adults: Ve Control A S Needed APYtesttestNo ratings yet
- Pan Trop Razo LeDocument2 pagesPan Trop Razo LeBeatrizz P GellaNo ratings yet
- Passo A Passo "Management" Farmacoterapia Da Asma: Updated!Document1 pagePasso A Passo "Management" Farmacoterapia Da Asma: Updated!Eduardo PalmaNo ratings yet
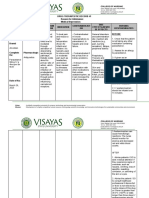
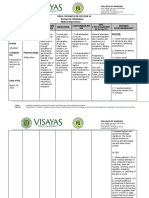
- Drug Name Drug Class Mechanism of Action Indications Contra-Indications Side Effects/ Adverse Effects Nursing ConsiderationDocument9 pagesDrug Name Drug Class Mechanism of Action Indications Contra-Indications Side Effects/ Adverse Effects Nursing ConsiderationJhucyl Mae GalvezNo ratings yet
- 65 - Approach To Patients With CancerDocument1 page65 - Approach To Patients With CancerRica Alyssa PepitoNo ratings yet
- Pharmacotherapy ChartsDocument28 pagesPharmacotherapy ChartsDr AUNo ratings yet
- DSDSSDDocument10 pagesDSDSSDkrischaniNo ratings yet
- Nursing Care Management 109 NotesDocument9 pagesNursing Care Management 109 NotesJanelle Cabida SupnadNo ratings yet
- DivalproexDocument2 pagesDivalproexeefrheelNo ratings yet
- Drug Study ICUDocument2 pagesDrug Study ICUErryl Justine AdvinculaNo ratings yet
- HPN Drug StudyDocument4 pagesHPN Drug StudyJohn Haider Colorado GamolNo ratings yet
- Drug Study AmpicillinDocument3 pagesDrug Study AmpicillinChristine NocomuraNo ratings yet
- Refrat Asma Eksaserbasi - Dr. Retna, Sp. PDocument24 pagesRefrat Asma Eksaserbasi - Dr. Retna, Sp. PWaskito Setiaji100% (1)
- Drug study-FOURTH TWO MEDICAL WARDDocument2 pagesDrug study-FOURTH TWO MEDICAL WARDErryl Justine AdvinculaNo ratings yet
- Pharm 2017 Final - REVMGDocument108 pagesPharm 2017 Final - REVMGSbNo ratings yet
- Postpartum NCPDocument2 pagesPostpartum NCPGershom Perez AcaboNo ratings yet
- CNS: Headach E, Dizzines S, Vertigo, Nerve Root Lesion, Asthenia, InsomniDocument8 pagesCNS: Headach E, Dizzines S, Vertigo, Nerve Root Lesion, Asthenia, InsomniHsintan HsuNo ratings yet
- Urdaneta City University College of Health Sciences: Bachelor of Science in NursingDocument3 pagesUrdaneta City University College of Health Sciences: Bachelor of Science in NursingRara GandaNo ratings yet
- Asma BronquialDocument131 pagesAsma BronquialNeil Arón Paz-CamposNo ratings yet
- Medication: Drug Type Description ExamplesDocument8 pagesMedication: Drug Type Description ExamplesRyrey Abraham PacamanaNo ratings yet
- DiazepamDocument4 pagesDiazepamElyhna Mara U. GonzalesNo ratings yet
- Asthma Interactive0712Document87 pagesAsthma Interactive0712Putri AyuNo ratings yet
- Screenshot 2023-05-16 at 6.30.09 PMDocument29 pagesScreenshot 2023-05-16 at 6.30.09 PMNoor Rateb AlmajaliNo ratings yet
- Drug Study RosillosaDocument4 pagesDrug Study RosillosaJb RosillosaNo ratings yet
- Diazepam and Midazolam Nursing ConsiderationsDocument11 pagesDiazepam and Midazolam Nursing ConsiderationsP BNo ratings yet
- JD Drug-1-2Document2 pagesJD Drug-1-2RON PEARL ANGELIE CADORNANo ratings yet
- Drug Study 1Document13 pagesDrug Study 1Basema HashhashNo ratings yet
- JD DrugDocument6 pagesJD DrugRON PEARL ANGELIE CADORNANo ratings yet
- Drug Study Morphine and ProtonixDocument3 pagesDrug Study Morphine and ProtonixHarvey Lampa SelimNo ratings yet
- Drug Study: La Salle UniversityDocument3 pagesDrug Study: La Salle UniversityJb RosillosaNo ratings yet
- Nicolas, Krizha-Drug StudyDocument12 pagesNicolas, Krizha-Drug StudyKrizha Angela NicolasNo ratings yet
- I. Drug Study: Drug Mechanism of Action Indications Contraindication Side Effects Nursing ConsiderationsDocument3 pagesI. Drug Study: Drug Mechanism of Action Indications Contraindication Side Effects Nursing Considerationscyn yana0723No ratings yet
- M.I. (Losartan) Drug Study)Document2 pagesM.I. (Losartan) Drug Study)Angelica Marie MacaslingNo ratings yet
- Drug Study SampleDocument2 pagesDrug Study SampleRoselle Oquiton FuertesNo ratings yet
- Drug Study of Case Presentation 2Document6 pagesDrug Study of Case Presentation 2banana cueNo ratings yet
- CelecoxibDocument2 pagesCelecoxibmimi2188No ratings yet
- Final exam review head to toe assessmentDocument50 pagesFinal exam review head to toe assessmentLou EscobarNo ratings yet
- Final exam review head to toe assessmentDocument50 pagesFinal exam review head to toe assessmentLou EscobarNo ratings yet
- Study Guide for Dermatology ExamDocument92 pagesStudy Guide for Dermatology ExamLou Escobar100% (1)
- Brain Dump SheetDocument2 pagesBrain Dump SheetLou EscobarNo ratings yet
- NR 509 Midterm Interview TechniquesDocument76 pagesNR 509 Midterm Interview TechniquesLou EscobarNo ratings yet
- Clinical Practice GuidelinesDocument9 pagesClinical Practice GuidelinesIntel AtomNo ratings yet
- Skin Rash Station Worksheet and HandoutDocument5 pagesSkin Rash Station Worksheet and HandoutLou EscobarNo ratings yet
- ECG Immersion Station Student Handouts Updated 3.1.19Document4 pagesECG Immersion Station Student Handouts Updated 3.1.19Lou EscobarNo ratings yet
- Asthma CURRENT Medical Diagnosis and Treatment 2022Document7 pagesAsthma CURRENT Medical Diagnosis and Treatment 2022Lou EscobarNo ratings yet
- Asthma CURRENT Medical Diagnosis and Treatment 2022Document7 pagesAsthma CURRENT Medical Diagnosis and Treatment 2022Lou EscobarNo ratings yet
- Course Out Line EH MSCPH LESSON 1Document42 pagesCourse Out Line EH MSCPH LESSON 1Muhubo MusseNo ratings yet
- ACEP Ketamine Guideline 2011Document13 pagesACEP Ketamine Guideline 2011Daniel Crook100% (1)
- NAC Asthma COPD Medications Chart 2022 - A4 - WebDocument1 pageNAC Asthma COPD Medications Chart 2022 - A4 - WebkanemuraaNo ratings yet
- AsthmaDocument8 pagesAsthmaJade DeopidoNo ratings yet
- Stress: and The IndividualDocument9 pagesStress: and The Individualsamon sumulongNo ratings yet
- Improve Wellbeing with Hand Mudra PositionsDocument9 pagesImprove Wellbeing with Hand Mudra PositionsmsharisaiNo ratings yet
- Beta-Blockers: Friend or Foe in Asthma?: International Journal of General Medicine DoveDocument7 pagesBeta-Blockers: Friend or Foe in Asthma?: International Journal of General Medicine DoveastriedamaliaamanatNo ratings yet
- Medical Nutrition Therapy in Pulmonary DiseaseDocument86 pagesMedical Nutrition Therapy in Pulmonary DiseaseyufapipiNo ratings yet
- ASTHMADocument51 pagesASTHMAMOSES M CHILALANo ratings yet
- Antiasthamatic DrugsDocument72 pagesAntiasthamatic DrugsDeepak kumarNo ratings yet
- Unit Test - Fourth QuarterDocument2 pagesUnit Test - Fourth QuartergretchelleNo ratings yet
- Asthma and COPDDocument47 pagesAsthma and COPDSamuelVilbrunNo ratings yet
- Diagnosis of Bronchial AsthmaDocument12 pagesDiagnosis of Bronchial AsthmaVineet Mariyappan100% (1)
- Number 1Document3 pagesNumber 1Michael HostiadiNo ratings yet
- New Treatments For Severe Treatment-Resistant Asthma - Lancet Resp Med 2013Document14 pagesNew Treatments For Severe Treatment-Resistant Asthma - Lancet Resp Med 2013Azan Al RasyidNo ratings yet
- GPS Submittal PDFDocument32 pagesGPS Submittal PDFshankar05No ratings yet
- Marwan PDDocument251 pagesMarwan PDLaura GranadosNo ratings yet
- Jurnal KesehatanDocument16 pagesJurnal KesehatanIndar WahyuniNo ratings yet
- Chronic Illness Module OutcomesDocument12 pagesChronic Illness Module OutcomesOmar IzzoNo ratings yet
- NCM 112 Lecture Notes (Respiratory System and Its Diseases)Document9 pagesNCM 112 Lecture Notes (Respiratory System and Its Diseases)Kyle FernandezNo ratings yet
- Spirometry Interpretation MCAS Miramar 4-7-10Document73 pagesSpirometry Interpretation MCAS Miramar 4-7-10Henry WojtczakNo ratings yet
- Drugs For AsthmaDocument7 pagesDrugs For Asthmaapi-3736350No ratings yet
- AEBADocument6 pagesAEBAAtirah AaNo ratings yet
- Artículo Epoc Gold 2023Document26 pagesArtículo Epoc Gold 2023SMIBA MedicinaNo ratings yet
- AsthmaDocument18 pagesAsthmaKainanNo ratings yet
- Hamza DissertDocument108 pagesHamza DissertMobin Ur Rehman KhanNo ratings yet
- Asthma Thesis StatementDocument4 pagesAsthma Thesis Statementfjnev0hc100% (2)