You might also like
- Dysphagia Evaluation and Collaborative ManagementDocument10 pagesDysphagia Evaluation and Collaborative ManagementVerry YudhanaNo ratings yet
- Atlas of Feline Anatomy For VeterinariansDocument275 pagesAtlas of Feline Anatomy For VeterinariansДибензол Ксазепин100% (4)
- What To Do Following A Workplace AccidentDocument5 pagesWhat To Do Following A Workplace AccidentMona DeldarNo ratings yet
- Diagnosis and Treatment of Neurogenic Oropharyngeal DysphagiaFrom EverandDiagnosis and Treatment of Neurogenic Oropharyngeal DysphagiaNo ratings yet
- Common Health Problems That Develop During Infancy MPNDocument14 pagesCommon Health Problems That Develop During Infancy MPNShaii Whomewhat GuyguyonNo ratings yet
- Gastroenterology PDFDocument18 pagesGastroenterology PDFSijo SunnyNo ratings yet
- Geology Harn v1 2Document17 pagesGeology Harn v1 2vze100% (1)
- Roto Fix 32 Service ManualDocument31 pagesRoto Fix 32 Service Manualperla_canto_150% (2)
- Energy Optimization of A Large Central Plant Chilled Water SystemDocument24 pagesEnergy Optimization of A Large Central Plant Chilled Water Systemmuoi2002No ratings yet
- Rigging: GuideDocument244 pagesRigging: Guideyusry72100% (11)
- PPC Production PlantDocument106 pagesPPC Production PlantAljay Neeson Imperial100% (1)
- SA01 GENXXX SDIN BSDS 0001 B04 A - Instrumentation Design Basis Sazeh CommentedDocument31 pagesSA01 GENXXX SDIN BSDS 0001 B04 A - Instrumentation Design Basis Sazeh Commentedamini_mohiNo ratings yet
- Nfpa 502 Critical Velocity Vs Fffs EffectsDocument5 pagesNfpa 502 Critical Velocity Vs Fffs Effectsamir shokrNo ratings yet
- Estimating The Outcome of Umbilical Diseases Based On Clinical Examination in Calves: 322 CasesDocument5 pagesEstimating The Outcome of Umbilical Diseases Based On Clinical Examination in Calves: 322 CasesFathurrahman Maulana RifqiNo ratings yet
- Gastric Dilatation Organoaxial Volvulus in A DogDocument6 pagesGastric Dilatation Organoaxial Volvulus in A DogKrlÖz Ändrz Hërëdîa ÖpzNo ratings yet
- Cricopharyngeal DysphagiaDocument8 pagesCricopharyngeal Dysphagiataner_soysurenNo ratings yet
- Diaphragmatic Hernia in A Cat Mimicking A Pulmonary MassDocument5 pagesDiaphragmatic Hernia in A Cat Mimicking A Pulmonary Massfernando martinezNo ratings yet
- Usg in CADocument3 pagesUsg in CAJasmine EffendiNo ratings yet
- Colonic Volvulus With Defects of The MesentericDocument5 pagesColonic Volvulus With Defects of The MesentericTiago PaixãoNo ratings yet
- Vet Radiology Ultrasound - 2023 - de Magistris - Ultrasonographic Features of Intestinal Lipogranulomatous Lymphangitis inDocument9 pagesVet Radiology Ultrasound - 2023 - de Magistris - Ultrasonographic Features of Intestinal Lipogranulomatous Lymphangitis innerakyokNo ratings yet
- Comparison of RX Us For Diagnosing Small-Intestinal Mechanical Obstruction in Vomiting DogsDocument8 pagesComparison of RX Us For Diagnosing Small-Intestinal Mechanical Obstruction in Vomiting DogsVanesa CaceresNo ratings yet
- Crews (2009) JVIM - Clinical Ultrasonographic and Laboratory Findings Gallbladder Disease and RuptureDocument8 pagesCrews (2009) JVIM - Clinical Ultrasonographic and Laboratory Findings Gallbladder Disease and RuptureNick GoodyNo ratings yet
- Atresia EsofagusDocument7 pagesAtresia EsofagusTommysNo ratings yet
- Estudio Endoscopico-Patologico en Estenosis Pilorica Adquirida en GatosDocument8 pagesEstudio Endoscopico-Patologico en Estenosis Pilorica Adquirida en GatosTatiana Ramirez SibocheNo ratings yet
- LaryngectomyDocument7 pagesLaryngectomyŞahin ŞahinNo ratings yet
- Gastric Volvulus: Bang Chau, Susan DufelDocument2 pagesGastric Volvulus: Bang Chau, Susan DufelmustikaarumNo ratings yet
- Sildenafil Improves Clinical Signs andDocument6 pagesSildenafil Improves Clinical Signs andJuliana Ramos PereiraNo ratings yet
- Boysen, Vru, 2003Document9 pagesBoysen, Vru, 2003stylianos kontosNo ratings yet
- Gastrointestinal Disease in Cats and Dogs With Gastrointestinal Foreign BodiesDocument4 pagesGastrointestinal Disease in Cats and Dogs With Gastrointestinal Foreign BodiesRafiNo ratings yet
- Digestive Endoscopy - 2015 - Ohmiya - Obscure Gastrointestinal Bleeding Diagnosis and TreatmentDocument10 pagesDigestive Endoscopy - 2015 - Ohmiya - Obscure Gastrointestinal Bleeding Diagnosis and Treatmentpgomez156No ratings yet
- Ejm 21 1 50 51Document2 pagesEjm 21 1 50 51Ellie ChrétienNo ratings yet
- Open Cervical Surgery For Congenital H-Type Tracheoesophageal Fistulae - TOFDocument8 pagesOpen Cervical Surgery For Congenital H-Type Tracheoesophageal Fistulae - TOFHussein AhmedNo ratings yet
- Dejesus Et Al 2020 Ultrasonographic Evaluation of Cholecystoduodenostomy Sites in Six CatsDocument9 pagesDejesus Et Al 2020 Ultrasonographic Evaluation of Cholecystoduodenostomy Sites in Six CatscitratomNo ratings yet
- Pedsinreview 2021005196Document4 pagesPedsinreview 2021005196Claudio MontiNo ratings yet
- 10 53424-Balikesirsbd 1146243-2548313Document4 pages10 53424-Balikesirsbd 1146243-2548313obenimNo ratings yet
- Risk of Anesthesia Related Complications in Brachycephalic DogsDocument6 pagesRisk of Anesthesia Related Complications in Brachycephalic DogsAkın SeverNo ratings yet
- Cecocolic Intussusception and Cecal Torsion in Cattle: Clinical ReportsDocument5 pagesCecocolic Intussusception and Cecal Torsion in Cattle: Clinical Reportsallan felipeNo ratings yet
- Small Intestines and Appendix - AnnoDocument97 pagesSmall Intestines and Appendix - AnnoJuan Lorenzo RequironNo ratings yet
- Dental Root Canal Treatment Complicated by Foreign Body IngestionDocument4 pagesDental Root Canal Treatment Complicated by Foreign Body IngestionDr.O.R.GANESAMURTHINo ratings yet
- Surgical Correction of Idiopathic Megacolon in Cats: Feline Practice January 1992Document7 pagesSurgical Correction of Idiopathic Megacolon in Cats: Feline Practice January 1992Ayu DinaNo ratings yet
- Intestinal Atresia: A Case ReportDocument3 pagesIntestinal Atresia: A Case ReportOvamelia JulioNo ratings yet
- Gastric Foreign Bodies in DogsDocument4 pagesGastric Foreign Bodies in Dogsayiq_utariNo ratings yet
- Review On Enterocutaneous FistulaDocument31 pagesReview On Enterocutaneous FistulaAbu ZidaneNo ratings yet
- Top 5 Complications of GonadectomyDocument7 pagesTop 5 Complications of GonadectomyCabinet VeterinarNo ratings yet
- 161004acuteaof Gi - MadridDocument73 pages161004acuteaof Gi - MadridMAPACHE 91No ratings yet
- Laparoscopic Heller Myotomy For Achalasia: Robert N. Cacchione, M.D., Dan N. Tran, M.D., Diane H. Rhoden, M.DDocument5 pagesLaparoscopic Heller Myotomy For Achalasia: Robert N. Cacchione, M.D., Dan N. Tran, M.D., Diane H. Rhoden, M.Dgabriel martinezNo ratings yet
- Bloat in RabbitDocument4 pagesBloat in RabbitAmik DonissaNo ratings yet
- TVP 2017 0304 Feature Ear Disease FORWEBDocument7 pagesTVP 2017 0304 Feature Ear Disease FORWEBΝίκος ΚριτσοταλάκηςNo ratings yet
- Ashcraft's HPSDocument5 pagesAshcraft's HPSmiracle ktmNo ratings yet
- Trilogy of Foregut Midgut and Hindgut Atresias PreDocument5 pagesTrilogy of Foregut Midgut and Hindgut Atresias PreEriekafebriayana RNo ratings yet
- Perioperative Point-Of-Care Gastric Ultrasound: K. El-Boghdadly T. Wojcikiewicz and A. PerlasDocument8 pagesPerioperative Point-Of-Care Gastric Ultrasound: K. El-Boghdadly T. Wojcikiewicz and A. PerlaskamounthNo ratings yet
- 1 PBDocument6 pages1 PBrizalakbarsyaNo ratings yet
- Urological Emergencies and Diseases in Wilderness ExpeditionsDocument10 pagesUrological Emergencies and Diseases in Wilderness ExpeditionsrakaNo ratings yet
- Case Report Esophageal AtresiaDocument3 pagesCase Report Esophageal Atresiaadriani lawrenciaNo ratings yet
- Journal of Clinical Microbiology 2014 Balakrishnan 3447.fullDocument6 pagesJournal of Clinical Microbiology 2014 Balakrishnan 3447.fullPutri Nadia ReskiNo ratings yet
- Chronic Gastric Dilatation in Horses Diagnosis, Treatment and Feeding Management A Survey of 20 Clinical CasesDocument8 pagesChronic Gastric Dilatation in Horses Diagnosis, Treatment and Feeding Management A Survey of 20 Clinical CasesXp Julieth HernandezNo ratings yet
- Sas S2Document6 pagesSas S2Cyrille Jhane A GalvezNo ratings yet
- Gaschen 2008Document9 pagesGaschen 2008JesseNo ratings yet
- Appendix DuplicationDocument3 pagesAppendix DuplicationMario TrejoNo ratings yet
- VetSurg - 2021 Simpson - Cholecystectomy in 23 Cats 2005-2021Document8 pagesVetSurg - 2021 Simpson - Cholecystectomy in 23 Cats 2005-2021Silvia RoseNo ratings yet
- VetPractice 04 2014 Equine AprilDocument1 pageVetPractice 04 2014 Equine AprilsatriaarceusNo ratings yet
- Brunner's Gland Adenoma: Case ReportDocument3 pagesBrunner's Gland Adenoma: Case ReportasclepiuspdfsNo ratings yet
- Esophagus Symptoms and InvestigationDocument7 pagesEsophagus Symptoms and InvestigationJinNo ratings yet
- Spinal Epidural Abscess in Two CalvesDocument8 pagesSpinal Epidural Abscess in Two CalvesRachel AutranNo ratings yet
- Management of Jejunoileal Atresia: Our 5 Year ExperienceDocument4 pagesManagement of Jejunoileal Atresia: Our 5 Year ExperienceOvamelia JulioNo ratings yet
- Corpus Alienum EsophagusDocument3 pagesCorpus Alienum EsophagusTrhey Ahmilza DamaitaNo ratings yet
- EXOTİC-Urinary Badder Eversion in Rabbit DoesDocument5 pagesEXOTİC-Urinary Badder Eversion in Rabbit Doestaner_soysurenNo ratings yet
- Jsap 13286Document10 pagesJsap 13286AnaNo ratings yet
- Colitis: A Practical Approach to Colon and Ileum Biopsy InterpretationFrom EverandColitis: A Practical Approach to Colon and Ileum Biopsy InterpretationAnne Jouret-MourinNo ratings yet
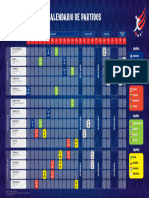
- CA2024 Calendario de Partidos - 2023.12.07 ESDocument1 pageCA2024 Calendario de Partidos - 2023.12.07 ESultramegathundertiger17No ratings yet
- The Romantic Piano Concerto 66: Howard ShelleyDocument14 pagesThe Romantic Piano Concerto 66: Howard ShelleyMarcelo SpeschaNo ratings yet
- Manzanas Con Manzanas: Immigrant Reception in An Era of Racial ColorblindnessDocument18 pagesManzanas Con Manzanas: Immigrant Reception in An Era of Racial ColorblindnessMarcelo SpeschaNo ratings yet
- Wisdomtooth ComplicationsinextractionDocument4 pagesWisdomtooth ComplicationsinextractionMarcelo SpeschaNo ratings yet
- Case Study: A Delayed and Severe Presentation of Coronectomy ComplicationDocument5 pagesCase Study: A Delayed and Severe Presentation of Coronectomy ComplicationMarcelo SpeschaNo ratings yet
- Intelligent Text Extraction From PDF Documents: December 2005Document4 pagesIntelligent Text Extraction From PDF Documents: December 2005Marcelo SpeschaNo ratings yet
- Full Test Bank For Health Economics and Policy 7Th Edition Henderson PDF Docx Full Chapter ChapterDocument34 pagesFull Test Bank For Health Economics and Policy 7Th Edition Henderson PDF Docx Full Chapter Chapterpeeepochaq15d100% (9)
- Calao Deliquente Diadi River SystemDocument15 pagesCalao Deliquente Diadi River SystemJason MalamugNo ratings yet
- BCA2006 BCA GuideDocument507 pagesBCA2006 BCA GuidePatrick LiaoNo ratings yet
- Online Games and Academic AchievementDocument25 pagesOnline Games and Academic AchievementJasmine GamoraNo ratings yet
- Group 5 - Ethical PrinciplesDocument11 pagesGroup 5 - Ethical Principlesvirgo paigeNo ratings yet
- 2020 Q2 CushWake Jakarta IndustrialDocument2 pages2020 Q2 CushWake Jakarta IndustrialCookiesNo ratings yet
- Chapter One - FiveDocument118 pagesChapter One - FivePrecious AnthonyNo ratings yet
- Hemostatic AgentsDocument18 pagesHemostatic AgentshariNo ratings yet
- Power Divider and Combiner: EE403-Microwave Engineering MTC, EE Dep., Electromagnetic Waves GroupDocument52 pagesPower Divider and Combiner: EE403-Microwave Engineering MTC, EE Dep., Electromagnetic Waves GroupHabibat El Rahman AshrafNo ratings yet
- MAOH600 Ropu 48 Presentation Script and ReferencesDocument10 pagesMAOH600 Ropu 48 Presentation Script and ReferencesFano AsiataNo ratings yet
- AERO241 Example 10Document4 pagesAERO241 Example 10Eunice CameroNo ratings yet
- Catalogue CV. Traka Abadi UniversalDocument15 pagesCatalogue CV. Traka Abadi UniversalHackers StevenNo ratings yet
- Notice of Privacy Practices (Generic)Document3 pagesNotice of Privacy Practices (Generic)cecilled_08No ratings yet
- 3 Ways To Take Isabgol - WikiHowDocument6 pages3 Ways To Take Isabgol - WikiHownasirNo ratings yet
- Adult Module 1 - Five Healthy Habits Handout (English) PDFDocument2 pagesAdult Module 1 - Five Healthy Habits Handout (English) PDFKennedy FadriquelanNo ratings yet
- Campus Sexual Violence - Statistics - RAINNDocument6 pagesCampus Sexual Violence - Statistics - RAINNJulisa FernandezNo ratings yet
- Chap 6 - Karen HorneyDocument95 pagesChap 6 - Karen HorneyDiana San JuanNo ratings yet
- Buss 37 ZemaljaDocument50 pagesBuss 37 ZemaljaOlga KovacevicNo ratings yet
- Emerging Re-Emerging Infectious Disease 2022Document57 pagesEmerging Re-Emerging Infectious Disease 2022marioNo ratings yet
- Paterno Report: Dr. Fred S. Berlin, M.D., PH.D Final Report 2-7-2013Document45 pagesPaterno Report: Dr. Fred S. Berlin, M.D., PH.D Final Report 2-7-2013The Morning CallNo ratings yet