You might also like
- Jurnal PEIDocument4 pagesJurnal PEIMadonna Frozen100% (1)
- Extrapiramidal Symptom Rating Scale PDFDocument11 pagesExtrapiramidal Symptom Rating Scale PDFsisca satyaNo ratings yet
- Pedsql Module CardioDocument31 pagesPedsql Module CardioRatna100% (1)
- The Use of Visceral Proteins As Nutrition Markers: An ASPEN Position PaperDocument7 pagesThe Use of Visceral Proteins As Nutrition Markers: An ASPEN Position PaperAdrián LópezNo ratings yet
- Tatalaksana Awal Koreksi Cairan Pada Kasus Syok - Dr. Rudy K, SP - PDDocument60 pagesTatalaksana Awal Koreksi Cairan Pada Kasus Syok - Dr. Rudy K, SP - PDmuhammad benyNo ratings yet
- Telaah Kritis JurnalDocument13 pagesTelaah Kritis JurnalfebrinaNo ratings yet
- Daftar Kode Diagnosa & TindakanDocument7 pagesDaftar Kode Diagnosa & Tindakannovi andriyaniNo ratings yet
- Pemeriksaan Foto Thorax Pada Anak-AnakDocument29 pagesPemeriksaan Foto Thorax Pada Anak-AnakRenaldy PamungkasNo ratings yet
- PAT + Primary SurveyDocument33 pagesPAT + Primary Surveysalsa100% (1)
- Clabsi DR - RonaldDocument19 pagesClabsi DR - RonaldsilviNo ratings yet
- Cerebral Toxoplasmosis: Diagnosis & ManagementDocument32 pagesCerebral Toxoplasmosis: Diagnosis & ManagementShinta DianNo ratings yet
- Inotropic and Vasoactive Drugs in Pediatric ICUDocument6 pagesInotropic and Vasoactive Drugs in Pediatric ICUCandy RevolloNo ratings yet
- Graficas Sindrome Down Niños y AdolescentesDocument7 pagesGraficas Sindrome Down Niños y AdolescentesREYNANo ratings yet
- Extubation Criteria & Delayed EmergenceDocument3 pagesExtubation Criteria & Delayed EmergenceAnonymous OlS0WZwNo ratings yet
- Pembahasan CBT COMBO 3Document802 pagesPembahasan CBT COMBO 3Sari Dewi WiratsihNo ratings yet
- Sensitivitas Dan Spesifisitas Kriteria American College of Rheumatology (ACR) Dan Systemic Lupus International Collaborating Clinics Untuk Diagnosis Lupus Eritematosus SistemikDocument4 pagesSensitivitas Dan Spesifisitas Kriteria American College of Rheumatology (ACR) Dan Systemic Lupus International Collaborating Clinics Untuk Diagnosis Lupus Eritematosus Sistemikwidi kusumaNo ratings yet
- Syok Pada AnakDocument28 pagesSyok Pada AnakTaufik Abidin100% (1)
- Ross ScoreDocument7 pagesRoss Scoreradwika antyNo ratings yet
- Boys Charts Weight For Age 2 To 5 Years (Percentiles)Document1 pageBoys Charts Weight For Age 2 To 5 Years (Percentiles)Mimie CaliNo ratings yet
- SepsisDocument16 pagesSepsisDaniela100% (1)
- Management of Diabetes and Hyperglycemia in The Hospital: A Practical Guide To Subcutaneous Insulin Use in The Non-Critically Ill, Adult PatientDocument12 pagesManagement of Diabetes and Hyperglycemia in The Hospital: A Practical Guide To Subcutaneous Insulin Use in The Non-Critically Ill, Adult PatientRani Dwi NNo ratings yet
- PPT Referat ADHD - Kevin LukitoDocument22 pagesPPT Referat ADHD - Kevin LukitonoviaNo ratings yet
- Sejawat - Idn - Sistem Saraf Dan MuskuloskeletalDocument85 pagesSejawat - Idn - Sistem Saraf Dan MuskuloskeletalAinaya Miftia Asy'aristaNo ratings yet
- KriptorkismusDocument14 pagesKriptorkismusMutiara Prima DianaNo ratings yet
- Ventikular Septal Defect FixDocument18 pagesVentikular Septal Defect FixPutri Sari DewiNo ratings yet
- SINDROM NEFROTIK DR NendenDocument31 pagesSINDROM NEFROTIK DR NendennimuusmNo ratings yet
- Hamed2016Document4 pagesHamed2016Franknanda D'enzieroX-zhirawaxaveriuz PutrascreamoDark-nataseNo ratings yet
- Hannover Polytrauma Score.4Document2 pagesHannover Polytrauma Score.4Helmi IsmunandarNo ratings yet
- PPDS - AR - 22 16 - Agu - P Ilovepdf Compressed Ilovepdf C PDFDocument192 pagesPPDS - AR - 22 16 - Agu - P Ilovepdf Compressed Ilovepdf C PDFlaboratorium rshmdn100% (1)
- Abnormal Chest FindingsDocument5 pagesAbnormal Chest FindingsAbishek Prince100% (1)
- Dyspnea in Children - Wahyuni IndawatiDocument20 pagesDyspnea in Children - Wahyuni IndawatiTarmidi MidziNo ratings yet
- Japanese EncephalitisDocument14 pagesJapanese EncephalitisMuhammad Rafli AkbarNo ratings yet
- NBS Law FinalDocument33 pagesNBS Law Finalkissiah Cajetas100% (1)
- Fluid Managementuntuk Mahasiswa SajaDocument56 pagesFluid Managementuntuk Mahasiswa SajaPratami Rieuwpassa IINo ratings yet
- MCU Analysis Indolakto Purwosari 2017Document102 pagesMCU Analysis Indolakto Purwosari 2017Ririn WidyaNo ratings yet
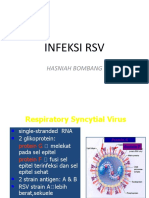
- Infeksi RSV: Hasniah BombangDocument12 pagesInfeksi RSV: Hasniah Bombangmuh hardiansyahNo ratings yet
- Critical Case in Congenital Heart Disease, What's The Sign and Initial Treatment For Them (Prof. Dr. Dr. Mulyadi M.djer, SpA (K) )Document69 pagesCritical Case in Congenital Heart Disease, What's The Sign and Initial Treatment For Them (Prof. Dr. Dr. Mulyadi M.djer, SpA (K) )tyesNo ratings yet
- MiopatiDocument7 pagesMiopatiMarco HutagaolNo ratings yet
- Skdi Full UkmppdDocument8 pagesSkdi Full UkmppdJosa Anggi PratamaNo ratings yet
- KARDIOMYOPATI - Kuliah DR - ErlinaDocument28 pagesKARDIOMYOPATI - Kuliah DR - ErlinaArif Zulfian MubarokNo ratings yet
- Air Leak SyndromesDocument2 pagesAir Leak SyndromesIchalAzNo ratings yet
- Acute Coronary Syndrome 052014Document91 pagesAcute Coronary Syndrome 052014Fatahillah NazarNo ratings yet
- Interna Medicine Case Report Prof. Dr. W. Z. Johannes Hospital AUGUST 2019 Medical Faculty Nusa Cendana UniversityDocument46 pagesInterna Medicine Case Report Prof. Dr. W. Z. Johannes Hospital AUGUST 2019 Medical Faculty Nusa Cendana UniversityErni JawaNo ratings yet
- Diabeticum Ketoacidosis: Ach. Najich RF, DRDocument16 pagesDiabeticum Ketoacidosis: Ach. Najich RF, DRAch Najich RfNo ratings yet
- Kuliah Blok GI Tract-ERCP, Agustus 2010Document15 pagesKuliah Blok GI Tract-ERCP, Agustus 2010HendryNo ratings yet
- Etiologi Dan Patogenesis Ikterus,...Document103 pagesEtiologi Dan Patogenesis Ikterus,...Raditya PrimaNo ratings yet
- Fetal Neural Tube 2021 12 LMBR PDFDocument24 pagesFetal Neural Tube 2021 12 LMBR PDFwayansiagaNo ratings yet
- Fluid Management: Suparto Anesthesia Department Medical Faculty Christian Krida Wacana UniversityDocument61 pagesFluid Management: Suparto Anesthesia Department Medical Faculty Christian Krida Wacana UniversitygozaNo ratings yet
- Laki-Laki, 21 Tahun Dengan Ketoasidosis DiabetikumDocument66 pagesLaki-Laki, 21 Tahun Dengan Ketoasidosis DiabetikumAnonymous gudRSKNo ratings yet
- Children With Henoch Schonlein Purpura 2.0Document13 pagesChildren With Henoch Schonlein Purpura 2.0soniaNo ratings yet
- Ablasio RetinaDocument29 pagesAblasio RetinaTenri AshariNo ratings yet
- Pembahasan UKDI CLINIC 3 Batch Mei 2016Document662 pagesPembahasan UKDI CLINIC 3 Batch Mei 2016widi kusumaNo ratings yet
- Disseminated Intravascular Coagulation in PregnancyDocument8 pagesDisseminated Intravascular Coagulation in Pregnancydr_asaleh100% (1)
- Demam Ruam: Della Rizki Anggilia 18105Document40 pagesDemam Ruam: Della Rizki Anggilia 18105Della Rizki AnggiliaNo ratings yet
- Cataract 20surgery 2029 05 2008 131224024457 Phpapp01Document61 pagesCataract 20surgery 2029 05 2008 131224024457 Phpapp01Bboy ToonNo ratings yet
- Buku Ajar Psikiatri FKUI Ed 3Document638 pagesBuku Ajar Psikiatri FKUI Ed 3karuniasantiNo ratings yet
- Fisiologi BerkemihDocument34 pagesFisiologi BerkemihTunik SugiantoNo ratings yet
- DEMAM Pada Bayi Dan Anak UmyDocument40 pagesDEMAM Pada Bayi Dan Anak UmyFarika NorNo ratings yet
- I1551 6776 12 3 138 PDFDocument9 pagesI1551 6776 12 3 138 PDFIvan VeriswanNo ratings yet
- PIIS2468644118301282Document5 pagesPIIS2468644118301282Lilly PattersonNo ratings yet
- 10.1007@s11060 020 03487 8Document6 pages10.1007@s11060 020 03487 8laurentiaNo ratings yet
- Echocardiographic Evaluation of Patent Ductus Arteriosus Neonatologists Perspective - Dr. Ahmad Kautsar, Sp.ADocument46 pagesEchocardiographic Evaluation of Patent Ductus Arteriosus Neonatologists Perspective - Dr. Ahmad Kautsar, Sp.AlaurentiaNo ratings yet
- Cancer Stem Cell Hypothesis: Implication For Cancer Prevention and TreatmentDocument16 pagesCancer Stem Cell Hypothesis: Implication For Cancer Prevention and TreatmentlaurentiaNo ratings yet
- Accepted Manuscript: Paediatric Respiratory ReviewsDocument32 pagesAccepted Manuscript: Paediatric Respiratory ReviewslaurentiaNo ratings yet
- Effects of Insulin-Like Growth Factor On Nitrogen Balance During Hypoxic ExposureDocument7 pagesEffects of Insulin-Like Growth Factor On Nitrogen Balance During Hypoxic ExposurelaurentiaNo ratings yet
- 10 1016@j Tube 2016 09 001Document7 pages10 1016@j Tube 2016 09 001laurentiaNo ratings yet
- European Journal of Integrative MedicineDocument6 pagesEuropean Journal of Integrative MedicinelaurentiaNo ratings yet
- Role of IGF-binding Proteins in Regulating IGF Responses To Changes in MetabolismDocument31 pagesRole of IGF-binding Proteins in Regulating IGF Responses To Changes in MetabolismlaurentiaNo ratings yet
- 1 s2.0 S147297921730389X MainDocument8 pages1 s2.0 S147297921730389X MainlaurentiaNo ratings yet
- Growth Hormone Replacement Therapy in Adults: 30 Years of Personal Clinical ExperienceDocument10 pagesGrowth Hormone Replacement Therapy in Adults: 30 Years of Personal Clinical ExperiencelaurentiaNo ratings yet
- NCM 118a Lec 10 Hyperosmolar Hyperglycemic SDocument4 pagesNCM 118a Lec 10 Hyperosmolar Hyperglycemic SJan Crizza Dale R. FrancoNo ratings yet
- SNOMEDDocument59 pagesSNOMEDMarcelo BencomoNo ratings yet
- Textbook Braddoms Rehabilitation Care A Clinical Handbook David X Cifu Ebook All Chapter PDFDocument53 pagesTextbook Braddoms Rehabilitation Care A Clinical Handbook David X Cifu Ebook All Chapter PDFpaul.smith924100% (16)
- Coclia EyelidDocument5 pagesCoclia EyelidFaradila HakimNo ratings yet
- Therapeutic Models-2 PDFDocument38 pagesTherapeutic Models-2 PDFDhen MarcNo ratings yet
- Hematocolpos Secondary To Imperforate Hymen: Clinical ImagesDocument2 pagesHematocolpos Secondary To Imperforate Hymen: Clinical ImagesQonny WelendriNo ratings yet
- Left Side Appendix With Appendicitis 333Document3 pagesLeft Side Appendix With Appendicitis 333Medtext PublicationsNo ratings yet
- Mid Term Examination: Physical Activity and The Stages of Behavior Change ModelDocument8 pagesMid Term Examination: Physical Activity and The Stages of Behavior Change Modelapi-457299309No ratings yet
- Chap6-Disease-Mgt-web - VersionDocument25 pagesChap6-Disease-Mgt-web - Versionronalit malintadNo ratings yet
- Integrated Therapeutics IiiDocument15 pagesIntegrated Therapeutics IiiSalahadinNo ratings yet
- Sepsis in Older PatientsDocument8 pagesSepsis in Older PatientsFajar WasilahNo ratings yet
- A Practical Guide To Clinical MedicineDocument6 pagesA Practical Guide To Clinical MedicineHo Lee SheetNo ratings yet
- Term III Practical FileDocument31 pagesTerm III Practical FileShivam kumarNo ratings yet
- Diagnosis and Prevention of Iron Deficiency and Iron-Deficiency Anemia in Infants and Young ChildrenDocument16 pagesDiagnosis and Prevention of Iron Deficiency and Iron-Deficiency Anemia in Infants and Young ChildrenAnwesa Priyadarsini PradhanNo ratings yet
- GAMMA-GT Carboxy GPNA: BiolaboDocument2 pagesGAMMA-GT Carboxy GPNA: BiolaboFariz KasyidiNo ratings yet
- Gyne Long Exam 5 Premalignant and Malignant Lesions Vulva and VaginaDocument3 pagesGyne Long Exam 5 Premalignant and Malignant Lesions Vulva and VaginaRemelou Garchitorena AlfelorNo ratings yet
- 2 - Pressure UlcersDocument64 pages2 - Pressure Ulcerscharity kalinowsky100% (5)
- Airedale N.H.S v. Bland 1993 (Basis of Auna) - DasvDocument29 pagesAiredale N.H.S v. Bland 1993 (Basis of Auna) - DasvNiten ChopraNo ratings yet
- Rev Sistemática - Effectiveness of Medical Nutrition Therapy in Adolescents With TD1Document13 pagesRev Sistemática - Effectiveness of Medical Nutrition Therapy in Adolescents With TD1Nayesca GonzalezNo ratings yet
- Critical Care in Obstetrics Guideline: NHSCT/12/515Document10 pagesCritical Care in Obstetrics Guideline: NHSCT/12/515ana mariaNo ratings yet
- TYPOLOGY OF FAMILY NURSING PROBLEMS HandoutDocument5 pagesTYPOLOGY OF FAMILY NURSING PROBLEMS HandoutMaxime EllaNo ratings yet
- Choice of Drug Therapy in Primary (Essential) Hypertension - UpToDateDocument58 pagesChoice of Drug Therapy in Primary (Essential) Hypertension - UpToDateEver LuizagaNo ratings yet
- Surgery Lecture 1st PatookDocument81 pagesSurgery Lecture 1st PatookPranjali WeladiNo ratings yet
- Microbiology PDFDocument237 pagesMicrobiology PDFchioNo ratings yet
- The Mississippi Small Business and Grocer Investment ActDocument294 pagesThe Mississippi Small Business and Grocer Investment ActJonathan AllenNo ratings yet
- Naja SeabrookDocument2 pagesNaja SeabrookJay KulkarniNo ratings yet
- Labreportnew 6782Document1 pageLabreportnew 6782Shahabuddin AnsariNo ratings yet
- Examen Primer Parcial INGLESDocument5 pagesExamen Primer Parcial INGLESTatiana PerezNo ratings yet
- What Happens To You When You Don't Sleep For Days Days/: (Penyebaran)Document5 pagesWhat Happens To You When You Don't Sleep For Days Days/: (Penyebaran)Nur RafeeahNo ratings yet