You might also like
- Cupping Benefits With Respect To AgeDocument12 pagesCupping Benefits With Respect To AgeAnonymous CYdagINo ratings yet
- Feldenkrais Method Empowers Adults With Chronic.4Document13 pagesFeldenkrais Method Empowers Adults With Chronic.4Yvette M Reyes100% (1)
- Mike ReinoldDocument20 pagesMike ReinoldVikas Kashnia0% (1)
- Chiropractic ICD-10 Code ListDocument5 pagesChiropractic ICD-10 Code ListDale100% (1)
- A Prospective Study in Analgesic Effect of Distal Sodium Channel Blockers (DSCB) in Patients With SciaticaDocument5 pagesA Prospective Study in Analgesic Effect of Distal Sodium Channel Blockers (DSCB) in Patients With SciaticaInternational Journal of Innovative Science and Research Technology100% (1)
- Jurnal Mengurangi Nyeri Meningkatkan Kualitas DepresiDocument6 pagesJurnal Mengurangi Nyeri Meningkatkan Kualitas DepresiPerdanaNo ratings yet
- Musculoskeletal Science and PracticeDocument7 pagesMusculoskeletal Science and PracticeDavid SoaresNo ratings yet
- Family Medicine & Medical Science ResearchDocument9 pagesFamily Medicine & Medical Science ResearchAndhika DNo ratings yet
- 1 s2.0 S1836955319300578 MainDocument12 pages1 s2.0 S1836955319300578 MainSairam PhysioNo ratings yet
- Malone Final SignedDocument29 pagesMalone Final Signedapi-622666324No ratings yet
- Low Back Pain Prognosis Structured Review of The LiteratureDocument6 pagesLow Back Pain Prognosis Structured Review of The Literaturec5rga5h2No ratings yet
- Positive Lifestyle Behaviours and Emotional Health Factors Are Associated With Low Back Pain ResilienceDocument11 pagesPositive Lifestyle Behaviours and Emotional Health Factors Are Associated With Low Back Pain ResilienceJacks CanalsNo ratings yet
- Kaptein-Common-Sense Model-OsteoarthritisDocument9 pagesKaptein-Common-Sense Model-OsteoarthritisZyania MelchyNo ratings yet
- The Effectiveness of Non-Pharmaceutical Interventions Upon Pregnancy-Related Low Back Pain: A Systematic Review and Meta-AnalysisDocument11 pagesThe Effectiveness of Non-Pharmaceutical Interventions Upon Pregnancy-Related Low Back Pain: A Systematic Review and Meta-AnalysisYenie YenNo ratings yet
- Jurnal Pendukung 1 - A Systematic Review and Meta-Analysis of Exercise Interventions in Schizophrenia PatientsDocument19 pagesJurnal Pendukung 1 - A Systematic Review and Meta-Analysis of Exercise Interventions in Schizophrenia PatientsM SNo ratings yet
- Patients' Experience of Health Three Years After Structured Physiotherapy or Surgery For Lumbar Disc HerniationDocument8 pagesPatients' Experience of Health Three Years After Structured Physiotherapy or Surgery For Lumbar Disc HerniationsamNo ratings yet
- Physiotherapy: JournalofDocument7 pagesPhysiotherapy: JournalofMaulida HalimahNo ratings yet
- Lower Back PainDocument18 pagesLower Back PainmeganNo ratings yet
- Jurnal LBPDocument10 pagesJurnal LBPeka mei dianitaNo ratings yet
- Spinal Manipulation and Exercise For Low Back Pain in Adolescents: Study Protocol For A Randomized Controlled TrialDocument9 pagesSpinal Manipulation and Exercise For Low Back Pain in Adolescents: Study Protocol For A Randomized Controlled TrialMizan PaishalNo ratings yet
- Jurnal 2Document18 pagesJurnal 2Yusuf WildanNo ratings yet
- Fragilidad Dolor y EjercicioDocument7 pagesFragilidad Dolor y EjercicioCecilia Suarez HerreraNo ratings yet
- 1941Document7 pages1941Zia CobosNo ratings yet
- The Effectiveness of Complementary ManualDocument10 pagesThe Effectiveness of Complementary ManualAli DptNo ratings yet
- Risk Factors Forchronic Low Back Pain 2161 0711.1000271Document4 pagesRisk Factors Forchronic Low Back Pain 2161 0711.100027155664411No ratings yet
- The Effectiveness of A Group Based Otago Exercise Program On Phy - 2023 - Geriat PDFDocument14 pagesThe Effectiveness of A Group Based Otago Exercise Program On Phy - 2023 - Geriat PDFJefrioSuyantoNo ratings yet
- Ho 2013Document6 pagesHo 2013Vera El Sammah SiagianNo ratings yet
- 2019 Article 5476Document10 pages2019 Article 5476Gaspar ContrerasNo ratings yet
- Low Back Pain 2018Document18 pagesLow Back Pain 2018Salazar Ángel100% (1)
- Cairns 2006Document12 pagesCairns 2006David LorencNo ratings yet
- 5 Spinal Mobilization Vs Conventional PhysiotherapyDocument11 pages5 Spinal Mobilization Vs Conventional PhysiotherapyEstrella SegniniNo ratings yet
- Relationship of Chronic LBP (Low Back Pain) With Hamstring Tightness in ProfessionalsDocument5 pagesRelationship of Chronic LBP (Low Back Pain) With Hamstring Tightness in ProfessionalsRizwan khanNo ratings yet
- Effectiveness of A Low Back Pain ClassificationDocument11 pagesEffectiveness of A Low Back Pain ClassificationLuis cabezas mirandaNo ratings yet
- Stimsonm Researchcritiquen531Document11 pagesStimsonm Researchcritiquen531api-270067627No ratings yet
- Literacy-Adapted Cognitive Behavioral Therapy Versus Education For Chronic Pain at Low-Income ClinicsDocument15 pagesLiteracy-Adapted Cognitive Behavioral Therapy Versus Education For Chronic Pain at Low-Income ClinicsJay JalaliNo ratings yet
- Pain Kronis Di Kota Denpasar Dan Kabupaten Badung: Studi Tentang Rekomendasi Fisioterapis Pada Pasien Low BackDocument10 pagesPain Kronis Di Kota Denpasar Dan Kabupaten Badung: Studi Tentang Rekomendasi Fisioterapis Pada Pasien Low Backgamma kurnia mahananiNo ratings yet
- Relationship of Chronic LBP (Low Back Pain) With Hamstring Tightness in ProfessionalsDocument6 pagesRelationship of Chronic LBP (Low Back Pain) With Hamstring Tightness in ProfessionalsRizwan khanNo ratings yet
- The Ef Cacy of Systematic Active Conservative Treatment For Patients With Severe SciaticaDocument12 pagesThe Ef Cacy of Systematic Active Conservative Treatment For Patients With Severe SciaticaTomáš KrajíčekNo ratings yet
- Pone 0203029jsjsjDocument20 pagesPone 0203029jsjsjElizabethBarriaNo ratings yet
- The Treatment of Acute Low Back Pain - Bed Rest, Exercises, or Ordinary Activity?Document5 pagesThe Treatment of Acute Low Back Pain - Bed Rest, Exercises, or Ordinary Activity?Arya Maulana NugrohoNo ratings yet
- Dor Lombar Crônica em IdososDocument6 pagesDor Lombar Crônica em IdososYara Borini RossiNo ratings yet
- Cognitive Functional Therapy in Patients With Non Specific Chronic Low Back Pain-A Randomized Controlled Trial 3 Year Follow UpDocument9 pagesCognitive Functional Therapy in Patients With Non Specific Chronic Low Back Pain-A Randomized Controlled Trial 3 Year Follow UpRachel PutriNo ratings yet
- Physiotherapy As An Initial Treatment Option For Femoroacetabular ImpingementDocument9 pagesPhysiotherapy As An Initial Treatment Option For Femoroacetabular ImpingementNicolas ParejaNo ratings yet
- ContentServer AspDocument8 pagesContentServer AspClauNo ratings yet
- Chan, Clara (2017)Document8 pagesChan, Clara (2017)Rafael FontesNo ratings yet
- Case Report 2 FinalDocument50 pagesCase Report 2 Finalapi-680119126No ratings yet
- Factors Associated With Quality of Life in Patients With Depression: A Nationwide Population-Based StudyDocument12 pagesFactors Associated With Quality of Life in Patients With Depression: A Nationwide Population-Based StudyMinodora MilenaNo ratings yet
- Pta 2750 Term Research ProjectDocument11 pagesPta 2750 Term Research Projectapi-240265376No ratings yet
- Manipulação e Mobilização para o Tratamento Da Dor Crônica Inespecífica Do Pescoço Uma Revisão Sistemática e Meta-Análise para Um Painel de AdequaçãoDocument24 pagesManipulação e Mobilização para o Tratamento Da Dor Crônica Inespecífica Do Pescoço Uma Revisão Sistemática e Meta-Análise para Um Painel de AdequaçãoCelso SouzaNo ratings yet
- Artículo 3 - Manipulacion and Movilzacion para Dolor Lumbar CrónicoDocument25 pagesArtículo 3 - Manipulacion and Movilzacion para Dolor Lumbar CrónicoNicolás Espinoza ConstanzoNo ratings yet
- Faktor ResikoDocument7 pagesFaktor ResikoAnonymous hF9HwHVuqNo ratings yet
- Jamaneurology Van Dillen 2020 Oi 200094 1617209065.06484Document11 pagesJamaneurology Van Dillen 2020 Oi 200094 1617209065.06484Meme BuletNo ratings yet
- Federici 2007Document10 pagesFederici 2007Tomáš MartínekNo ratings yet
- Effect of Intensive Patient Education Vs Placebo Patient Education On Outcomes in Patients With Acute Low Back Pain A Randomized Clinical TrialDocument9 pagesEffect of Intensive Patient Education Vs Placebo Patient Education On Outcomes in Patients With Acute Low Back Pain A Randomized Clinical TrialsoylahijadeunvampiroNo ratings yet
- Chiropractic Care For Adults With Pregnancy Related Low Back, Pelvic Gridle Pain or Combinated Pais A Sistematic ReviewDocument18 pagesChiropractic Care For Adults With Pregnancy Related Low Back, Pelvic Gridle Pain or Combinated Pais A Sistematic ReviewQuiropraxia ChapecóNo ratings yet
- Effectiveness of An Extension-OrientedDocument11 pagesEffectiveness of An Extension-OrientedAna Carolina SouzaNo ratings yet
- (Journal of Neurosurgery - Spine) Patient Misconceptions Concerning Lumbar Spondylosis Diagnosis and TreatmentDocument7 pages(Journal of Neurosurgery - Spine) Patient Misconceptions Concerning Lumbar Spondylosis Diagnosis and Treatmentefancoolhand09No ratings yet
- Guided Imagery Relaxation Therapy in Malaysian Patients With Knee Osteoarthritis: A Randomized Controlled TrialDocument12 pagesGuided Imagery Relaxation Therapy in Malaysian Patients With Knee Osteoarthritis: A Randomized Controlled TrialLili YaacobNo ratings yet
- Brennan Et Al Spine 2006 RCT LBPDocument9 pagesBrennan Et Al Spine 2006 RCT LBPEric ZhangNo ratings yet
- Chronic Pain DissertationDocument7 pagesChronic Pain DissertationColumbia100% (1)
- Case ReportDocument9 pagesCase ReportStephany Granados GonzalezNo ratings yet
- Synthesis Paper Final DraftDocument24 pagesSynthesis Paper Final Draftapi-669373317No ratings yet
- Clinical GuidelinesDocument34 pagesClinical GuidelinesAlberto PachecoNo ratings yet
- Evaluation of The Lumbar Multifidus in Rowers During Espinal Estabilizacion ExercisesDocument7 pagesEvaluation of The Lumbar Multifidus in Rowers During Espinal Estabilizacion ExercisesAline KreiNo ratings yet
- SpineDocument7 pagesSpineayyappakrishnadasNo ratings yet
- Williams Exercises Vs Mckenzie ExercisesDocument3 pagesWilliams Exercises Vs Mckenzie ExercisesMasi KhanNo ratings yet
- Journal of Bodywork & Movement Therapies: Md. Nasir Ali, Kritika Sethi, Majumi M. NoohuDocument6 pagesJournal of Bodywork & Movement Therapies: Md. Nasir Ali, Kritika Sethi, Majumi M. NoohuNurul Annisa KamalNo ratings yet
- Diploma in AcccupressureDocument7 pagesDiploma in AcccupressureKishore TadinadaNo ratings yet
- Benhur Shipping Corporation Vs RiegoDocument17 pagesBenhur Shipping Corporation Vs RiegoDon FreecssNo ratings yet
- Johnson OE (2012) - Therapeutic Exercises in The Management of Non-Specific Low Back PainDocument23 pagesJohnson OE (2012) - Therapeutic Exercises in The Management of Non-Specific Low Back PainApollwn100% (1)
- Strength Versus Stability - Part 1 Concept and Terms PDFDocument11 pagesStrength Versus Stability - Part 1 Concept and Terms PDFDiego Cruces OrdoñezNo ratings yet
- Centennial Transmarine Inc., Eduardo R. Jabla, Centennial Maritime Services & M/T ACUSHNET, Petitioners EMERITO E. SALES, RespondentDocument26 pagesCentennial Transmarine Inc., Eduardo R. Jabla, Centennial Maritime Services & M/T ACUSHNET, Petitioners EMERITO E. SALES, RespondentSamantha AdduruNo ratings yet
- Bru Magne 2004Document4 pagesBru Magne 2004Juan PalomoNo ratings yet
- 9789513944360Document146 pages9789513944360Roar SyltebøNo ratings yet
- Research Article: Prevalence of Low Back Pain Among Undergraduate Physiotherapy Students in NigeriaDocument5 pagesResearch Article: Prevalence of Low Back Pain Among Undergraduate Physiotherapy Students in NigeriaMirza Kurnia AngelitaNo ratings yet
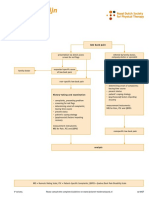
- Dutch LBP Physiotherapy FlowchartDocument2 pagesDutch LBP Physiotherapy FlowchartyohanNo ratings yet
- Exercises" - : "Mckenzie'S A ReviewDocument1 pageExercises" - : "Mckenzie'S A ReviewSuhaila NajibNo ratings yet
- Suitability V3 - 56 ItemDocument41 pagesSuitability V3 - 56 ItemMary Divine Grace BalagtasNo ratings yet
- Low Back Pain + Spinal StenosisDocument67 pagesLow Back Pain + Spinal StenosiswildanmalikNo ratings yet
- Benzakour-Benzakour2019 Article DiscHerniationAndDiscDiseaseTh PDFDocument6 pagesBenzakour-Benzakour2019 Article DiscHerniationAndDiscDiseaseTh PDFLee제노No ratings yet
- Paramedical Dissertations 2018, 2019 BatchDocument69 pagesParamedical Dissertations 2018, 2019 Batchsana naazNo ratings yet
- Lower Back PainDocument9 pagesLower Back PainAishath Samha HussainNo ratings yet
- Pseudoscience in The Use of ManipulationDocument6 pagesPseudoscience in The Use of Manipulationlpcmg1No ratings yet
- Combinepdf 3Document95 pagesCombinepdf 3paruNo ratings yet
- Diagnosis and Treatment of Low Back Pain: A Clinical Practice Guideline From Korean Association of Pain MedicineDocument37 pagesDiagnosis and Treatment of Low Back Pain: A Clinical Practice Guideline From Korean Association of Pain Medicinekang soon cheolNo ratings yet
- Clinical StudyDocument9 pagesClinical StudyJavierAntonioMéndezNo ratings yet
- Doctor and Patient Mini CEX - Teaching Points CompilationDocument74 pagesDoctor and Patient Mini CEX - Teaching Points CompilationCalder JohnsonNo ratings yet
- TecarDocument9 pagesTecarMarco PastoreNo ratings yet
- Efficacy of Mckenzie Approach Combined With Sustained Traction in Improving The Quality of Life Following Low Back Ache - A Case ReportDocument6 pagesEfficacy of Mckenzie Approach Combined With Sustained Traction in Improving The Quality of Life Following Low Back Ache - A Case ReportDr. Krishna N. SharmaNo ratings yet