Professional Documents
Culture Documents
Outcome of Polyhydroamnios
Outcome of Polyhydroamnios
Uploaded by
MuhammadAzharZaeniCopyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
Outcome of Polyhydroamnios
Outcome of Polyhydroamnios
Uploaded by
MuhammadAzharZaeniCopyright:
Available Formats
Outcomes From Polyhydramnios
With Normal Ultrasound
Enav Yefet, MD, PhDa Etty Daniel-Spiegel, MDa,b
OBJECTIVE: To investigate the short- and long-term outcomes of children from pregnancies abstract
complicated with polyhydramnios, defined as amniotic fluid index (AFI) >24 cm, and with a
normal detailed ultrasound examination.
METHODS: This retrospective cohort study examined 134 children aged 4 to 9 years with
polyhydramnios and normal detailed ultrasound examination during pregnancy compared
with 268 controls with normal AFI and normal detailed ultrasound examination matched
for maternal age, year of delivery, gestational week at delivery, and presence or absence
of diabetes. The primary outcome was the rate of malformations diagnosed postnatally.
Additional outcomes were obstetrics outcomes, genetic syndromes, and neurodevelopment.
RESULTS: Polyhydramnios was associated with increased risk for cesarean delivery (CD)
and birth weight >90th percentile. This elevation in CD was attributed to increased rate of
elective CD due to suspected macrosomia. Polyhydramnios was associated with increased
risk for congenital malformations (n = 25 [19%] compared with 27 [10%], respectively;
P = .016) without a statistically significant increase in the rate of major malformations (11
[8%] vs. 10 [4%]; P = .057). Genetic syndromes were more prevalent in the polyhydramnios
group (5 [3.7%] vs. 2 [0.75%]; P = .043), as were neurologic disorders and developmental
delay (9.7% vs. 3%; P = .004).
CONCLUSIONS: Despite a normal detailed ultrasound examination, polyhydramnios is
associated with increased rate of fetal malformations, genetic syndromes, neurologic
disorders, and developmental delay, which may be diagnosed only after birth.
aDepartment of Obstetrics and Gynecology, Emek Medical Center, Afula, Israel; and bUltrasound Unit, WHAT’S KNOWN ON THIS SUBJECT: The outcome
Department of Obstetrics and Gynecology, Emek Medical Center, Afula, Israel
of children with polyhydramnios depends on the
Dr Yefet drafted the initial manuscript; Dr Daniel-Spiegel designed the data collection instruments primary etiology (eg, maternal diabetes, fetal
and reviewed and revised the manuscript; and both authors conceptualized and designed the malformations). However, the short- and long-term
study and approved the final manuscript as submitted. outcome of polyhydramnios without a prenatal
DOI: 10.1542/peds.2015-1948 known etiology with normal detailed ultrasound
examination is not clear.
Accepted for publication Nov 17, 2015
Address correspondence to Enav Yefet, Department of Obstetrics & Gynecology, Emek Medical WHAT THIS STUDY ADDS: This study demonstrates
Center, Afula, Israel. Fax: 972-4-649-5483; e-mail: enavy1@gmail.com that despite a prenatal normal detailed ultrasound
examination, polyhydramnios is associated
PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online, 1098-4275).
with increased risk for fetal malformations,
Copyright © 2016 by the American Academy of Pediatrics genetic syndromes, neurologic disorders, and
FINANCIAL DISCLOSURE: The authors have indicated they have no financial relationships relevant developmental delay that might be diagnosed only
to this article to disclose. after birth.
FUNDING: No external funding.
POTENTIAL CONFLICT OF INTEREST: The authors have indicated they have no potential conflicts of
interest to disclose.
To cite: Yefet E and Daniel-Spiegel E. Outcomes From
Polyhydramnios With Normal Ultrasound. Pediatrics.
2016;137(2):e20151948
Downloaded from www.aappublications.org/news by guest on December 9, 2018
PEDIATRICS Volume 137, number 2, February 2016:e20151948 ARTICLE
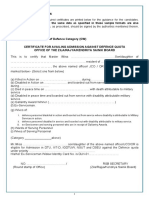
FIGURE 1
Patient flow chart.
Polyhydramnios complicates 0.5% associated with preterm delivery, much of the data is based on studies
to 2% of all pregnancies. It may unstable lie, malpresentation,4 cord from 20 years ago, when sonographic
be defined as either the sum of 4 prolapse, and placental abruption.8 assessment and fetal and neonatal
quadrant measurements (amniotic management were less developed.
In 50% to 60% of cases, the
fluid index [AFI]) >24 cm or a single Second, other factors for unfavorable
etiology remains elusive during
pocket of amniotic fluid >8 cm.1,2 outcomes such as prematurity, which
pregnancy. Polyhydramnios by itself
Known maternal etiologies for is more common in polyhydramnios,
has a prognostic implication, as
polyhydramnios include diabetes were not sufficiently controlled for.
pregnancies with polyhydramnios
mellitus, placental tumors, and In addition, to date, the information
without fetal malformations are
fetal pathologies such as fetal regarding long-term outcomes of
associated with increased risk for
malformations, chromosomal children after pregnancies with
aberrations, and neuromuscular preterm labor, large for gestational
polyhydramnios is still scarce. One
abnormalities.3 age (LGA) and small for gestational
study that examined the effect
age fetuses, low Apgar scores, fetal
Different subdivisions of of idiopathic polyhydramnios
distress during labor, and increased
polyhydramnios have been found abnormalities in 28.4% of
rate of cesarean delivery (CD).
associated with different perinatal cases during the first year of life;2
Perinatal mortality was 2 to 5 times
outcomes. Increasing severity however, the study had no control
higher for neonates after pregnancies
correlates with increased group, and some of the abnormalities
complicated with idiopathic
perinatal mortality and congenital were related to prematurity and
polyhydramnios compared with the
abnormalities.4 Early diagnosis not polyhydramnios per se. Studies
general population.3,9–11
before 30 gestational weeks has been of older children are not available.
associated with worse prognosis Nevertheless, data regarding the Finally, 20% of polyhydramnios cases
because of more central nervous long- and short-term outcomes of are related to diabetes.3,12 Because
system abnormalities.5,6 Persistent children from pregnancies with polyhydramnios in such pregnancies
polyhydramnios has been associated polyhydramnios and normal detailed is not considered idiopathic, those
with fetal aneuploidy,7 and ultrasound examination is limited pregnancies were excluded from other
polyhydramnios at birth has been due to several considerations. First, studies and their outcome is not clear.
Downloaded from www.aappublications.org/news by guest on December 9, 2018
2 YEFET and DANIEL-SPIEGEL
In the current study, we aimed to TABLE 1 Patient Characteristics
investigate the short- and long- Characteristic Polyhydramnios Control P
term outcomes of children aged 4 n 134 268
to 9 years from pregnancies with Maternal age, y 31 ± 5.7 (31) 31 ± 5.5 (31) .8
polyhydramnios and a normal Maternal BMI, kg/m2 24.4 ± 5.2 (23.4) 24.4 ± 4.8 (23.2) .9
detailed ultrasound examination. Gestational age at birth, wks 38.4 ± 2 (39) 38.7 ± 1.7 (39) .1
Number of birtha 3 ± 1.3 (3) 3 ± 1.5 (2) .5
We controlled for possible
Diabetes mellitus
confounders by using a control Gestational diabetes 21(16) 42 (16) 1.0
group matched for maternal age, Pregestational diabetes (P-GDM) 7 (5) 14 (5)
year of delivery, gestational week Type 1 (% of P-GDM) 1 (14) 2 (14) 1.0
at delivery, and presence or absence Type 2 (% of P-GDM) 6 (86) 12 (86)
Glycemic control
of diabetes.
Good 17 (60) 41 (73)
Poor 10 (34) 15 (27) .3
METHODS Not reported 1 (4) 0
Performed amniocentesis 35 (26) 21 (8) 0.0001
Study Population Need for amnioreduction 4 (3) — —
Gestational age at polyhydramnios diagnosis, 28.2 ± 5.6 (28) — —
This retrospective cohort study wks
was carried out in the obstetric Early: 20–29 wks 6 d 76 (57)
department of a university teaching Medium: 30–34 wks 6 d 36 (27)
Late: ≥35 wks 22 (16)
hospital in Afula, Israel, and
Severity of polyhydramniosb — —
included patients delivered in the Mild (AFI ≤30 cm) 93 (69)
hospital from 2005 to 2010. All Severe (AFI >30 cm) 31 (23)
the patients underwent a detailed Not reported 10 (8)
ultrasound examination to evaluate Persistent polyhydramnios 97 (72) — —
Polyhydramnios at birthc — —
fetal measurements, AFI, detailed Yes 42 (31)
anatomic scan, and screening for No 70 (52)
diabetes. Anatomic scans were Not known 22 (17)
performed as part of routine Values are expressed as mean ± SD (median) or n (%).
a Indicates number of births the woman had including the present one.
pregnancy surveillance at 19 to
b In 10 cases (8%), polyhydramnios was reported according to AFI but the value was missing.
25 gestational weeks according c In 22 cases (17%) known to have polyhydramnios, patients were diagnosed with rupture of membranes before labor
to the guidelines of the Israel when admitted to the delivery unit; therefore AFI status was not known during delivery.
Society of Ultrasound in Obstetrics
and Gynecology, based on the Polyhydramnios Definitions diabetes; 19 of 21 patients (90%)
recommendations of the American had the examination. All the available
Institute of Ultrasound in Medicine.13 Polyhydramnios was determined
fetal echocardiograms in this
They were performed by a senior by using the AFI measurement
study were normal. The rest of the
physician who is an obstetrics and technique.1 Color Doppler was used
obstetric follow-up was the same as
gynecology specialist and who in cases of uncertainty regarding
with normal AFI. Polyhydramnios
underwent additional training in the presence of an umbilical cord
without diabetes is not considered an
ultrasound and was authorized to within the measured pocket.
indication for labor induction in our
perform anatomic scans. Polyhydramnios was defined as AFI
institution.
>24 cm. Repeated ultrasound for AFI
Children born during this period evaluation was done every 4 to 6 Within the polyhydramnios group,
were 4 to 9 years old during data weeks and before delivery. Additional the patients were subdivided into
collection for this study. AFI measurements were done at the following groups: (1) time
emergency department visits and of diagnosis: early (20 to 29.6
Exclusion Criteria
hospitalizations. Genetic counseling gestational weeks), medium (30
Pregnancies without anatomic followed by amniocentesis, 100-g to 34.6 weeks), and late (≥35
scans; with multiple gestation, oral glucose tolerance test, and fetal weeks); (2) severity: mild (AFI ≤30
fetal malformations, or genetic echocardiogram are recommended cm) and severe (AFI >30 cm); (3)
abnormalities diagnosed in these cases. Fetal echocardiogram persistent polyhydramnios (defined
antenatally; with antenatal death was done in 34 patients (25% of as ≥2 sonographic examinations
or oligohydramnios; or in which the polyhydramnios group). Fetal with polyhydramnios on different
diabetes was not evaluated were echocardiogram is also indicated days) versus not persistent; and (4)
excluded from this study. in patients with pregestational polyhydramnios present at birth
Downloaded from www.aappublications.org/news by guest on December 9, 2018
PEDIATRICS Volume 137, number 2, February 2016 3
TABLE 2 Obstetric and Short-term Outcomes was defined as any neurologic
Factor Polyhydramnios Control P impairment affecting motor function,
n 134 268
emotion, learning ability, self-control,
Vacuum extraction 6 (5) 6 (2.5) .2 and memory that was documented
CD 42 (31) 57 (21) .02 in the pediatric medical record or
Labor dystocia 3 (2) 5 (2) .8 the records of the specialized child
Nonreassuring fetal monitoring 3 (2.2) 10 (3.7) .5
development clinics. According to the
Electivea 36 (27) 42 (16) .008
Indications for elective CD recommendations of the Ministry of
Previous CD 17 (13) 25 (9) .3 Health in Israel, all children undergo
Previous single CD and suspected 4 (3) 1 (0.4) .04 regular neurologic assessment by
macrosomia a pediatrician at the ages of 2 to 3
Suspected macrosomia 7 (5) 2 (0.7) .007
months, 9 months, 1.5 to 2 years,
Patient request 2 (1) 4 (1.5) 1
Placenta previa/tumor previa 2 (1) 1 (0.4) .3 and 5.5 years. Additional evaluations
Malpresentation 4 (3) 9 (3) 1 are performed upon parent or
Birth weight >90th percentile 27 (21) 26 (10) .003 educational staff request. Because
Birth weight <10th percentile 7 (5) 7 (2.5) .3 all Israeli citizens are entitled to
Macrosomia 15 (11) 13 (5) .02
the same health insurance, the
Male newborn 70 (52) 145 (54) .7
Nonvertex presentationb 4 (3) 13 (5) .4 public health system contains all the
Meconium 13 (10) 23 (9) .7 medical data.
Perineal tear grade 3 0 0
Apgar score <7 at 1 min 1 (0.75) 4 (1.5) .7
If the child had fetal malformations,
Apgar score <7 at 5 min 0 1 1 metabolic abnormalities, or seizures
Values are expressed as n (%).
as part of a genetic disease, he or she
a Each indication for elective surgery was compared with the complete group, either polyhydramnios or control. was included in the genetic diseases
b Values are different from those of the malpresentation row because the main indication was previously >1 CD in some
group and not the others.
of the cases.
Data Collection
versus not (in this specific analysis, Study Outcomes
cases with rupture of membranes at Demographic and obstetric
The primary outcome of this characteristics and sonographic
admission were excluded). We also
study was the rate of overall evaluation were extracted from the
collected data regarding the value of
fetal malformations diagnosed electronic medical records of the
the maximal vertical pocket (MVP).
postnatally in the polyhydramnios ultrasound unit of the Department
In all the polyhydramnios cases
group compared with the control of Obstetrics and Gynecology at
according to the AFI in which the MVP
group. The secondary outcomes Emek Medical Center, Maternal-
measurement was available (n = 6), it
were the rates of major and minor Fetal Medicine Unit, and Labor
was >8 cm, and there were no cases
malformations. Major malformations and Delivery Unit. Birth weight
with MVP >8 cm in the control group.
were considered those that generally percentiles were calculated according
Control Group cause functional impairment or to Dollberg growth curves, adjusted
require surgical correction.14 for the Israeli population.15 LGA
For each pregnancy with
Additional secondary outcomes were neonates were defined as birth
polyhydramnios, 2 pregnancies with
genetic and chromosomal alterations weight >90th percentile, and
normal AFI (in all the available scans)
diagnosed postnatally, obstetric macrosomia was defined as birth
were matched according to maternal
outcomes such as mode of delivery, weight >4000 g. Data regarding the
age, year of delivery, gestational
indications for CD, birth weight, neonates were extracted from the
week at delivery, and diabetes.
gender, malpresentations, meconium, electronic medical records of the
Maternal age was matched using the
Apgar scores <7 after 1 and 5 neonatology department and the
following age groups: <20, 20 to 30,
minutes, admission to the NICU, NICU. Data regarding long-term
30 to 35, 35 to 40, and >40 years.
and trauma at birth. Data regarding outcomes were collected from the
Gestational week at delivery was
postnatal oxygen support, perinatal children’s medical records in the
matched using the following ranges:
metabolic abnormalities, jaundice, community and from specialized
≤31 weeks (6 days) of gestation,
need for phototherapy, and seizures child development clinics.
32 to 36 (6), 37 to 40 (6), and ≥41
were also collected.
(6). After defining the selection Statistical Analysis
parameters, the group was chosen Finally, data regarding
randomly using the random option in neurodevelopment were collected. Because the overall malformation
Excel software. Neurodevelopment impairment rate in the general population is
Downloaded from www.aappublications.org/news by guest on December 9, 2018
4 YEFET and DANIEL-SPIEGEL
which 153 cases (60%) were normal
and 134 (90%) were available for
analysis.
The control group was chosen using
information from the Ultrasound
Unit, Maternal and Fetal Medicine
Unit, and delivery unit records.
The groups’ characteristics are
presented in Table 1. Because in
our center polyhydramnios is an
indication for genetic assessment,
the polyhydramnios group had more
patients with amniocentesis than the
control group. No cases of perinatal
mortality or death later in life were
reported.
Obstetric Outcomes
Table 2 summarizes the obstetric
characteristics of the polyhydramnios
and control groups. The risk for CD
was increased in the polyhydramnios
group. This was attributed to an
increased rate of elective surgeries
because of suspected macrosomia.
Occurrence of LGA neonate and
FIGURE 2 macrosomia were also significantly
Age distribution of the children in this study from pregnancies complicated with polyhydramnios.
increased in the polyhydramnios
Note that the age distribution of the children from the control group is the same.
group. The increased rates of CD,
LGA, and macrosomia were also
reported to be ∼5%,16 the sample between polyhydramnios and statistically significant after adjusting
size required to detect a 10% diabetes and to adjust for diabetes. for diabetes (CD adjusted odds ratios
difference is 333 pregnancies in a Statistical analyses were carried out [aOR] 1.745, 95% confidence interval
ratio of 1:2 (111 pregnancies with with SAS version 9.2 (SAS Institute, [CI] 1.1–2.8; LGA aOR 2.5, 95% CI
polyhydramnios and 222 in the Cary, NC). Significance was set at a P 1.4–4.5; macrosomia aOR 2.5, 95% CI
control group; 80% power, 2-sided value <.05. 1.2–5.5).
α = 0.05). Because 134 pregnancies
matched the inclusion criteria with The study was approved by the local The obstetric outcomes described
268 cases in the control group, the institutional review board. in Table 2 were also compared
power to detect the study hypothesis according to the polyhydramnios
was 88%. characteristics described in Patients
RESULTS and Methods and Table 1. Severe
Categorical variables are presented polyhydramnios was associated with
Patient Characteristics
as frequencies and percentages. LGA (n = 11 [35%] cases in severe vs
Continuous variables are presented Figure 1 shows the patient flow chart. 14 [15%] in mild polyhydramnios;
as average, SD, and median. The During the study period, 14 131 P = .01) and malpresentations (3
associations between categorical women underwent an ultrasound [10%] in severe vs 1 [1%] in mild
variables were analyzed by using examination in the Obstetrics and polyhydramnios; P = .047). LGA
χ2 test or Fisher exact test. For Gynecology Unit at Emek Medical was also more common when
continuous data, differences were Center. A total of 312 (2.2%) women polyhydramnios was persistent
assessed with the t test or Mann– had polyhydramnios during the compared with nonpersistent cases
Whitney U test. Simple and multiple second or third trimester. Of those, (25 [26%] vs 2 [6%]; P = .01). All the
stepwise logistic regressions were 275 women had available detailed other comparisons were statistically
carried out to assess interactions ultrasound examination results, of insignificant (data not shown).
Downloaded from www.aappublications.org/news by guest on December 9, 2018
PEDIATRICS Volume 137, number 2, February 2016 5
TABLE 3 Neonatal and Long-term Outcomes TABLE 4 Diagnosed Malformations and
Factor Polyhydramnios Control P Prevalence
n 134 268 Malformation n
Jaundice 53 (40) 94 (35) .4 Umbilical hernia 6
Phototherapy 33 (25) 47 (18) .1 Ventricular septal defect 5
Genetic disordera 5 (3.7) 2 (0.75) .04 Ventricular septal defect with other 5
Metabolic disorder 8 (6) 11 (4) .4 cardiac malformation
Congenital malformation Valvular stenosis or insufficiency 3
Overall 25 (19) 27 (10) .02 Congenital hearing loss 3
Majorb 11 (8) 10 (4) .06 External hydrocephalus 2
Minorb 18 (13) 23 (9) .1 Congenital hip dysplasia and torticolis 2
Postnatal oxygen support 2 (1.5) 5 (2) 1 Varicocelle and hydrocele of spermatic 2
Trauma at birth 1 (0.75) 4 (1.5) .7 cord
Intraventricular hemorrhage 1 (0.75) 1 (0.37) 1 Hydronephrosis 2
Convulsions/epilepsy 0 (0) 5 (2) .2 Hypospadias 2
Neural disorders and developmental delay 13 (9.7) 8 (3) .004 Vesicoureteral reflux 2
Admission to the NICUc 16 (12) 13 (5) .01 Metatarsus varus 1
Prematurity and related conditions 2 (1.5) 2 (0.7) .6 Atrial septal defect 1
Anemia and related conditions 3 (2.2) 2 (0.7) .3 Atrial septal defect and pulmonary valve 1
Respiratory problems and apnea 2 (1.5) 6 (2.2) .7 stenosis
Complications related to maternal diabetes 3 (2.2) 2 (0.7) .3 Branchial cleft cyst 1
Infections 1 (0.7) 0 (0) .3 Congenital anal fissure 1
Congenital malformations and genetic 5 (3.7) 1 (0.4) .02 Congenital dislocation of hip 1
disorders Congenital hypothyroidism 1
Values are expressed as n (%). Congenital talipes valgus 1
a Genetic abnormalities in the polyhydramnios group were 3 children with Bartter syndrome, 1 KCNK9 mutation, and Hypertrophic cardiomyopathy 1
1 familial Mediterranean fever (FMF). In the control group, genetic abnormalities included 1 case of primary ciliary Congenital laryngomalacia 1
dyskinesia and 1 FMF. Micropenis 1
b Children with simultaneous major and minor malformations are listed in both rows.
Congenital deformity of hip joint 1
c Primary indication for NICU admission. Genetic disorders refer to abnormalities that were later diagnosed as part of a
Brown syndrome (congenital) 1
genetic syndrome.
Patent ductus arteriosus 1
Patent foramen ovale and patent ductus 1
Neonatal Outcomes twice that of the control group. No arteriosus
specific system was found to be more Patent foramen ovale and peripheral 1
Figure 2 describes the age pulmonic stenosis
affected than others (Table 5). The
distribution of the children in this Pharyngeal anomaly 1
risk was also statistically significant Polydactyly 1
study. The children’s outcomes in the
after adjusting for diabetes (aOR 2.1, Pyloric stenosis 1
polyhydramnios group compared
95% CI 1.2–3.8). Characteristics of Rectal prolapse 1
with the control group are presented Ankyloglossia 1
polyhydramnios severity, time of
in Table 3. All the children were Congenital torticolis 1
diagnosis, and persistence did not
included in the analysis.
modify the risk (data not shown).
Fifty-six malformations were found (Table 3), also after adjusting for
The risk for genetic diseases was
in this study (Table 4). The most diabetes (aOR 2.7, 95% CI 1.3–6).
increased in the polyhydramnios
common were ventricular septal This difference was attributed to
group compared with the control
defects, isolated or with other genetic problems and congenital
group. The risk for genetic malformations (Table 3).
cardiac anomalies (10 [18%] cases).
Sonographic prenatal diagnosis was abnormalities was more pronounced
possible in only 35 (63%) of the in the severe polyhydramnios group Long-Term Neurodevelopment
cases. Findings that are not routinely than in the mild cases (3 [9.7%] vs
diagnosed in anatomic scans are 2 [2.15%], respectively; P = .008). The polyhydramnios group
The risk for genetic malformations demonstrated an increased rate
anatomic defects visible only after birth
in the mild polyhydramnios cases of neurodevelopment problems
(eg, patent ductus arteriosus), soft
was not statistically different compared with the control
anatomic changes (eg, ankyloglossia),
from that of the control group (2 group (Table 3). The types of
and defects that are predominantly
[2.15%] vs 2 [0.75%]; P = .2). Other neurodevelopment disorders are
functional in nature. The average
polyhydramnios characteristics did listed in Table 6. The increased rate
time for postnatal malformation
was still statistically significant
diagnosis was 7.4 ± 15.6 months. not modify the risk (data not shown).
after controlling for diabetes (aOR
The overall malformation rate in the More children were admitted to the 3.5, 95% CI 1.4–8.7). No association
polyhydramnios group was almost NICU in the polyhydramnios group was demonstrated between
Downloaded from www.aappublications.org/news by guest on December 9, 2018
6 YEFET and DANIEL-SPIEGEL
TABLE 5 Overall Congenital Malformations by Organ Systema group, the overall rate of
System Polyhydramnios Control P malformations diagnosed postnatally
n 134 268 was higher than that of the general
Cardiovascular 10 (7.5) 9 (3.4) .07 population. The risk for congenital
Genitourinary 5 (3.7) 4 (2.2) .2 malformations varies between
Skeletal 5 (3.7) 6 (2.2) .5 studies, ranging from 2% to 6%,
Abdominal wall defect 3 (2.2) 3 (1.1) .4
Congenital hypothyroidism 0 (0) 1 (0.37) 1 and depends on the population
Gastrointestinal 1 (0.75) 3 (1.1) 1 investigated and the definition
Respiratory 2 (1.5) 0 (0) .1 used.14 In this study, the incidence
Central nervous system 1 (0.75) 3 (1.1) 1 of fetal malformations in the control
Values are expressed as n (%). group was 10%, which is higher than
a Children who had malformations in >1 system are listed in all the relevant rows.
previously reported.16,26,27 The risk
for major anomaly in the presence
TABLE 6 Types of Neurodevelopmental Disorders of polyhydramnios and normal
Type of Disorder Polyhydramnios Control P detailed sonographic examination
n 134 268 was also higher than previously
Motoric difficulties and general slow 8 (6) 3 (1.1) .008 reported by Dashe et al.28 A possible
development
explanation is that studies of
Speech disturbance 3 (3.7) 1 (0.37) .1
Attention and learning disorders 5 (3.7) 2 (0.75) .04 congenital malformations are based
Pervasive developmental disorder 0 (0) 2 (0.75) .5 on records from the perinatal and
neonatal periods, whereas we also
considered malformations diagnosed
neurodevelopment impairment of children after pregnancies with years after birth. The most common
and fetal malformations (OR 1.6, polyhydramnios. Approximately 2% malformations in our study were of
95% CI 0.5–5.1). Polyhydramnios of the pregnancies were diagnosed the cardiovascular system. This is
characteristics did not modify the with polyhydramnios, and 60% of consistent with the results of Dashe
risk (data not shown). those were considered idiopathic. et al.28 In their cohort, the antenatal
These results are consistent with detection rate of cardiac anomalies
Diabetes Subanalysis previous studies.3 was the lowest and reached only
40%.28
We performed a separate analysis of The results demonstrated that
the short- and long-term outcomes polyhydramnios increased the Polyhydramnios also increased
of diabetic patients with and without risk for CD, LGA, and macrosomia. the risk for genetic disorders,
polyhydramnios (Table 7). When This information was reported especially in the severe cases. It
polyhydramnios was present, the risk previously.4,17–21 This study is should be noted that during the
for CD was elevated, particularly in innovative in demonstrating that the study period, genetic assessment
cases of previous CD with suspected rate of CD was increased mainly due included only fetal karyotype.
macrosomia. There were also more to elective surgeries for suspected Now that comparative genomic
cases of NICU admissions and macrosomia and not emergent hybridization has been introduced,
congenital malformations (Table CD during labor. Macrosomia has the association of idiopathic
7). When we used multiple logistic previously been shown to be a risk polyhydramnios with genetic
regression to examine whether factor for CD.22,23 Thus, one might abnormalities should be reassessed
diabetes modified the effect of suggest that those cases would be in future studies.
polyhydramnios on short- and long- operated on anyway if allowed to
In this study, there were 3 cases of
term outcomes, the interaction terms undergo a trial of labor. However,
Bartter syndrome. This syndrome
were statistically insignificant (P > this is not necessarily the case, as
is caused by mutations of genes
.05), suggesting that diabetes did not suspected macrosomia before labor
encoding proteins of the ion
modify the effect of polyhydramnios (either true or false) increased the
channels in the thick ascending
on the study outcomes. risk for CD.24,25
limb of the nephron.29 Severe
In the current study, it was shown polyhydramnios is caused by
DISCUSSION that although all the children excessive fetal urination. In our area,
underwent documented normal there are several families known to
In the current study, we investigated sonographic anatomic scan during carry Bartter syndrome mutations.
the long- and short-term outcomes pregnancy, in the polyhydramnios Similarly, the risk for genetic
Downloaded from www.aappublications.org/news by guest on December 9, 2018
PEDIATRICS Volume 137, number 2, February 2016 7
TABLE 7 Subanalysis of Study Outcomes in Pregnancies With Diabetes, With and Without were not statistically significant
Polyhydramnios between the groups; however,
Factor Polyhydramnios Control P this might be attributed to the
n 28 56 small sample size of pregnancies
Vacuum extraction 1 (3.6) 0 (0) .3 with diabetes. Interestingly, the
CD 15 (54) 17 (30) .04 risk for unfavorable outcomes in
Labor dystocia 0 (0) 2 (3.6) .6 polyhydramnios was not modified by
Nonreassuring fetal monitoring 3 (11) 2 (3.6) .3
the presence of diabetes.
Electivea 12 (43) 13 (23) .06
Previous CD 5 (18) 6 (11) .5
Previous single CD and suspected 3 (11) 0 (0) .03 The strengths of this study are the
macrosomia use of single-hospital information
Suspected macrosomia 3 (11) 2 (3.6) .3 and electronic documentations
Patient request 1 (3.6) 3 (5.4) 1
that were made in real time. The
Placenta previa/tumor previa 0 (0) 0 (0) 1
Malpresentation 0 (0) 2 (3.6) 1 control group was chosen randomly
Birth weight >90th percentile 8 (28) 8 (14) .1 by computer from all births in the
Birth weight <10th percentile 2 (7.2) 2 (3.6) .6 appropriate years, thus minimizing
Macrosomia 5 (18) 4 (7.1) .2 selection bias. Using a control group
Male newborn 16 (57) 29 (52) .6
matched for possible confounders
Nonvertex presentation 0 (0) 2 (3.6) .6
Meconium 0 (0) 5 (9) .2 for unfavorable outcomes such as
Perineal tear grade 3 0 (0) 0 (0) 1 maternal age and gestational week
Apgar score <7 at 1 min 0 (0) 1 (1.8) 1 enables isolation of the net effect
Apgar score <7 at 5 min 0 (0) 0 (0) 1 of polyhydramnios on the study
Admission to the NICU 5 (18) 2 (3.6) .04
outcomes.
Jaundice 15 (54) 20 (36) .1
Phototherapy 10 (36) 11 (20) .1
Genetic disorder 1 (3.6) 0 (0) .3 The limitations of this study
Metabolic disorder 6 (21) 5 (9) .2 are those inherent to the use of
Congenital malformations (overall) 10 (35) 6 (11) .006
retrospective databases. However,
Postnatal oxygen support 1 (3.6) 0 (0) .3
Trauma at birth 0 (0) 0 (0) 1 inaccuracies were minimized by
Intraventricular hemorrhage 0 (0) 0 (0) 1 the use of multiple sources such
Convulsions/epilepsy 0 (0) 2 (3.6) .6 as hospitalization records and
Neural disorders and developmental delay 3 (11) 2 (3.6) .3 documents from the ultrasound unit,
Values are expressed as n (%). pediatrics department, pediatricians,
a Each indication for elective surgery was compared with the whole group, either polyhydramnios or control.
and child development clinics.
Another limitation is the fact that
mutations probably depends on further, including in larger long-term diagnosis might be
the prevalence of genetic diseases prospective studies. influenced by the parents’ awareness
associated with polyhydramnios in In this study, we included and compliance with medical
specific populations. pregnancies with diabetes. We surveillance. Because the maternal
This study found an increased chose to do so because although this characteristics were similar in the
risk for neurodevelopmental group makes up 20% of the cases polyhydramnios and control groups,
delay and learning problems. of polyhydramnios, the information and because according to the law
To our knowledge, this is the in the literature regarding such in Israel all citizens are entitled
first study to report on this pregnancies with a normal anatomic to the same health insurance, the
outcome and in school-aged scan is scarce. Moreover, because difference in medical availability
children. The association polyhydramnios is a marker for and accessibility should not be
between polyhydramnios and uncontrolled diabetes, the patients substantially different between
neurodevelopmental delay is not with diabetes in the polyhydramnios the groups. A regular screening
clear. A possible hypothesis is and control groups might act program for neurodevelopment
that the swallowing mechanism, differently because of the nature of in schools and kindergartens
which is representative of normal glycemic control and not because of also helps to minimize possible
neurologic function in utero, is less polyhydramnios per se. We showed differences. It is acknowledged that
developed in those fetuses, resulting that the risks for CD, admission to the subgroup analyses in this study are
in the formation of polyhydramnios. NICU, and congenital malformations underpowered, and therefore their
However, this result as well as the were elevated in the presence of results should be interpreted with
hypothesis should be investigated polyhydramnios. Other outcomes caution.
Downloaded from www.aappublications.org/news by guest on December 9, 2018
8 YEFET and DANIEL-SPIEGEL
CONCLUSIONS 4. Sandlin AT, Chauhan SP, Magann EF. reproductive technology and birth
Clinical relevance of sonographically defects: a systematic review and
In summary, this study demonstrates
estimated amniotic fluid volume: meta-analysis. Hum Reprod Update.
that even after controlling for polyhydramnios. J Ultrasound Med. 2013;19(4):330–353
possible confounders including 2013;32(5):851–863
diabetes, pregnancies complicated 15. Dollberg S, Haklai Z, Mimouni
with polyhydramnios after normal 5. Barkin SZ, Pretorius DH, Beckett MK, FB, Gorfein I, Gordon ES. Birth
detailed ultrasound examination Manchester DK, Nelson TR, Manco- weight standards in the live-born
are at increased risk for CD, fetal Johnson ML. Severe polyhydramnios: population in Israel. Isr Med Assoc J.
incidence of anomalies. AJR Am J 2005;7(5):311–314
macrosomia, congenital malformation,
Roentgenol. 1987;148(1):155–159
and genetic abnormalities, as well 16. Davies MJ, Moore VM, Willson KJ, et
as neurodevelopment abnormalities 6. Pauer HU, Viereck V, Krauss V, al. Reproductive technologies and the
and delay. This information should Osmers R, Krauss T. Incidence of risk of birth defects. N Engl J Med.
be discussed with the patient, and fetal malformations in pregnancies 2012;366(19):1803–1813
children should be closely overseen by complicated by oligo- and
polyhydramnios. Arch Gynecol Obstet. 17. Harlev A, Sheiner E, Friger M,
pediatricians and child development
2003;268(1):52–56 Hershkovitz R. Polyhydramnios and
clinics. Finally, this important topic adverse perinatal outcome: what is the
should be investigated further, 7. Glantz JC, Abramowicz JS, Sherer DM. actual cutoff? J Matern Fetal Neonatal
particularly in prospective studies Significance of idiopathic midtrimester Med. 2014;27(12):1199–1203
designed to overcome the limitations polyhydramnios. Am J Perinatol.
of the current study. 1994;11(4):305–308 18. Biggio JR Jr, Wenstrom KD, Dubard
MB, Cliver SP. Hydramnios prediction
8. Moise KJ Jr. Polyhydramnios. Clin of adverse perinatal outcome.
ACKNOWLEDGMENTS Obstet Gynecol. 1997;40(2):266–279 Obstet Gynecol. 1999;94(5 pt 1):
773–777
We thank Naama Schwartz, PhD for 9. Taskin S, Pabuccu EG, Kanmaz
her kind assistance in the statistical AG, Kahraman K, Kurtay G. 19. Magann EF, Doherty DA, Lutgendorf
analysis. We also thank Mrs Snait Perinatal outcomes of idiopathic MA, Magann MI, Chauhan SP, Morrison
Ayalon for her assistance in data polyhydramnios. Interv Med Appl Sci. JC. Peripartum outcomes of high-risk
mining. 2013;5(1):21–25 pregnancies complicated by oligo-
and polyhydramnios: a prospective
10. Panting-Kemp A, Nguyen T, Chang longitudinal study. J Obstet Gynaecol
ABBREVIATIONS E, Quillen E, Castro L. Idiopathic Res. 2010;36(2):268–277
polyhydramnios and perinatal
AFI: amniotic fluid index 20. Golan A, Wolman I, Sagi J, Yovel I, David
outcome. Am J Obstet Gynecol.
aOR: adjusted odds ratio 1999;181(5 pt 1):1079–1082 MP. Persistence of polyhydramnios
CD: cesarean delivery during pregnancy: its significance and
CI: confidence interval 11. Chen KC, Liou JD, Hung TH, et al. correlation with maternal and fetal
LGA: large for gestational age Perinatal outcomes of polyhydramnios complications. Gynecol Obstet Invest.
MVP: maximal vertical pocket without associated congenital fetal 1994;37(1):18–20
anomalies after the gestational age
of 20 weeks. Chang Gung Med J. 21. Chauhan SP, Martin RW, Morrison
REFERENCES 2005;28(4):222–228 JC. Intrapartum hydramnios at term
and perinatal outcome. J Perinatol.
1. Moore TR, Cayle JE. The amniotic 12. Thompson O, Brown R, Gunnarson 1993;13(3):186–189
fluid index in normal human G, Harrington K. Prevalence of
pregnancy. Am J Obstet Gynecol. polyhydramnios in the third 22. Mazouni C, Rouzier R, Collette E, et
1990;162(5):1168–1173 trimester in a population screened al. Development and validation of
by first and second trimester a nomogram to predict the risk of
2. Dorleijn DM, Cohen-Overbeek
ultrasonography. J Perinat Med. cesarean delivery in macrosomia.
TE, Groenendaal F, Bruinse
1998;26(5):371–377 Acta Obstet Gynecol Scand.
HW, Stoutenbeek P. Idiopathic
2008;87(5):518–523
polyhydramnios and postnatal 13. American Institute of Ultrasound
findings. J Matern Fetal Neonatal Med. in Medicine. AIUM practice 23. Stotland NE, Hopkins LM, Caughey AB.
2009;22(4):315–320 guideline for the performance Gestational weight gain, macrosomia,
of obstetric ultrasound and risk of cesarean birth in
3. Magann EF, Chauhan SP, Doherty DA,
examinations. J Ultrasound Med. nondiabetic nulliparas. Obstet Gynecol.
Lutgendorf MA, Magann MI, Morrison
2013;32(6):1083–1101 2004;104(4):671–677
JC. A review of idiopathic hydramnios
and pregnancy outcomes. Obstet 14. Hansen M, Kurinczuk JJ, Milne 24. Peleg D, Warsof S, Wolf MF, Perlitz
Gynecol Surv. 2007;62(12):795–802 E, de Klerk N, Bower C. Assisted Y, Shachar IB. Counseling for fetal
Downloaded from www.aappublications.org/news by guest on December 9, 2018
PEDIATRICS Volume 137, number 2, February 2016 9
macrosomia: an estimated fetal 26. Anthony S, Buitendijk SE, Dorrepaal 28. Dashe JS, McIntire DD, Ramus
weight of 4,000 g is excessively low. CA, Lindner K, Braat DD, den Ouden RM, Santos-Ramos R, Twickler DM.
Am J Perinatol. 2014;32(1): AL. Congenital malformations in 4224 Hydramnios: anomaly prevalence and
71–74 children conceived after IVF. Hum sonographic detection. Obstet Gynecol.
25. Parry S, Severs CP, Sehdev HM, Reprod. 2002;17(8):2089–2095 2002;100(1):134–139
Macones GA, White LM, Morgan 27. Fujii M, Matsuoka R, Bergel E, van
MA. Ultrasonographic prediction of der Poel S, Okai T. Perinatal risk 29. Rodríguez-Soriano J. Bartter and
fetal macrosomia. Association with in singleton pregnancies after related syndromes: the puzzle is
cesarean delivery. J Reprod Med. in vitro fertilization. Fertil Steril. almost solved. Pediatr Nephrol.
2000;45(1):17–22 2010;94(6):2113–2117 1998;12(4):315–327
Downloaded from www.aappublications.org/news by guest on December 9, 2018
10 YEFET and DANIEL-SPIEGEL
Outcomes From Polyhydramnios With Normal Ultrasound
Enav Yefet and Etty Daniel-Spiegel
Pediatrics 2016;137;
DOI: 10.1542/peds.2015-1948 originally published online January 11, 2016;
Updated Information & including high resolution figures, can be found at:
Services http://pediatrics.aappublications.org/content/137/2/e20151948
References This article cites 29 articles, 2 of which you can access for free at:
http://pediatrics.aappublications.org/content/137/2/e20151948#BIBL
Subspecialty Collections This article, along with others on similar topics, appears in the
following collection(s):
Fetus/Newborn Infant
http://www.aappublications.org/cgi/collection/fetus:newborn_infant_
sub
Birth Defects
http://www.aappublications.org/cgi/collection/birth_defects_sub
Permissions & Licensing Information about reproducing this article in parts (figures, tables) or
in its entirety can be found online at:
http://www.aappublications.org/site/misc/Permissions.xhtml
Reprints Information about ordering reprints can be found online:
http://www.aappublications.org/site/misc/reprints.xhtml
Downloaded from www.aappublications.org/news by guest on December 9, 2018
Outcomes From Polyhydramnios With Normal Ultrasound
Enav Yefet and Etty Daniel-Spiegel
Pediatrics 2016;137;
DOI: 10.1542/peds.2015-1948 originally published online January 11, 2016;
The online version of this article, along with updated information and services, is
located on the World Wide Web at:
http://pediatrics.aappublications.org/content/137/2/e20151948
Pediatrics is the official journal of the American Academy of Pediatrics. A monthly publication, it
has been published continuously since 1948. Pediatrics is owned, published, and trademarked by
the American Academy of Pediatrics, 141 Northwest Point Boulevard, Elk Grove Village, Illinois,
60007. Copyright © 2016 by the American Academy of Pediatrics. All rights reserved. Print ISSN:
1073-0397.
Downloaded from www.aappublications.org/news by guest on December 9, 2018
You might also like
- An-Evaluation-Of-Risk-Factors-In-Cases-Of-Perinatal-Asphyxia-9563 2021Document4 pagesAn-Evaluation-Of-Risk-Factors-In-Cases-Of-Perinatal-Asphyxia-9563 2021Chiki CacaNo ratings yet
- HHS Public Access: Non-Immune Hydrops FetailsDocument12 pagesHHS Public Access: Non-Immune Hydrops FetailsYosita AuroraNo ratings yet
- Poster Session I: Results: Study DesignDocument2 pagesPoster Session I: Results: Study DesignFatih AkbarNo ratings yet
- Fetomaternal Outcome in Twin Pregnancies - A Retrospective Analysis From A Tertiary Care CentreDocument5 pagesFetomaternal Outcome in Twin Pregnancies - A Retrospective Analysis From A Tertiary Care CentreLouis HadiyantoNo ratings yet
- Non-Immune Hydrops Fetalis: Murat YurdakökDocument12 pagesNon-Immune Hydrops Fetalis: Murat YurdakökagitaNo ratings yet
- Bjo12636 PDFDocument9 pagesBjo12636 PDFLuphly TaluvtaNo ratings yet
- Alexander 1999Document5 pagesAlexander 1999Hòa HồNo ratings yet
- 1fg BasgDocument5 pages1fg BasgPrasetio Kristianto BudionoNo ratings yet
- Sifilis Congénita - Seminars Perinatology 2018Document9 pagesSifilis Congénita - Seminars Perinatology 2018AlejandraMayaNo ratings yet
- Acute Respiratory Distress Syndrome Among Premature Neonates: Prevalence, Mortality Rate and Risk Factors of MortalityDocument5 pagesAcute Respiratory Distress Syndrome Among Premature Neonates: Prevalence, Mortality Rate and Risk Factors of MortalityInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Less Is More Modern NeonatologyDocument11 pagesLess Is More Modern NeonatologyEN BUNo ratings yet
- 61 Goepfert2004Document7 pages61 Goepfert2004angela_karenina_1No ratings yet
- OligohidramnionDocument9 pagesOligohidramnionRizki R. WahidahNo ratings yet
- Hyperemesis Gravidarum and Risks of Placental Dysfunction Disorders: A Population-Based Cohort StudyDocument15 pagesHyperemesis Gravidarum and Risks of Placental Dysfunction Disorders: A Population-Based Cohort StudybellamonicaNo ratings yet
- Parto Prematuro y EPDocument7 pagesParto Prematuro y EPFrancisco Bustamante VelásquezNo ratings yet
- Risk Factor Assessment For Pre-Eclampsia: A Case Control StudyDocument6 pagesRisk Factor Assessment For Pre-Eclampsia: A Case Control StudyPutra SeptiansyahNo ratings yet
- Antecedents of CPDocument8 pagesAntecedents of CPЯковлев АлександрNo ratings yet
- Case Report: A Delayed Diagnosis of Congenital Syphilis-Too Many Missed OpportunitiesDocument4 pagesCase Report: A Delayed Diagnosis of Congenital Syphilis-Too Many Missed OpportunitiesFerdi KapisaNo ratings yet
- 140 140 1 PBDocument4 pages140 140 1 PBMina LelymanNo ratings yet
- A Clinical Study of Maternal and Perinatal Outcome in OligohydramniosDocument5 pagesA Clinical Study of Maternal and Perinatal Outcome in OligohydramniosNIKHILESH BADUGULANo ratings yet
- ObgynnnDocument5 pagesObgynnnGiga Hasabi AlkaraniNo ratings yet
- Tseng Et Al 2022 Severe Maternal Morbidity in Pregnancies Complicated by Fetal Congenital Heart DiseaseDocument10 pagesTseng Et Al 2022 Severe Maternal Morbidity in Pregnancies Complicated by Fetal Congenital Heart DiseaseUMAE GINENo ratings yet
- 538-Article Text-2068-1-10-20191125Document6 pages538-Article Text-2068-1-10-20191125Tifanny TantosoNo ratings yet
- 37004-Article Text-130842-2-10-20180629Document5 pages37004-Article Text-130842-2-10-20180629nishita biswasNo ratings yet
- Hypospadias and Early Gestation Growth Restriction in InfantsDocument8 pagesHypospadias and Early Gestation Growth Restriction in InfantsNaveed HussainNo ratings yet
- Good Outcome of Teenage Pregnancies in High-Quality Maternity CareDocument5 pagesGood Outcome of Teenage Pregnancies in High-Quality Maternity CareNabila MomorNo ratings yet
- European Journal of Obstetrics & Gynecology and Reproductive BiologyDocument7 pagesEuropean Journal of Obstetrics & Gynecology and Reproductive BiologySuis MionooNo ratings yet
- Late Intra-Uterine Fetal Demise With Fetal Hydrops: Challenges of Management Planning in IndonesiaDocument13 pagesLate Intra-Uterine Fetal Demise With Fetal Hydrops: Challenges of Management Planning in IndonesiaGeztaNasafirHermawanNo ratings yet
- Jurnal NewDocument6 pagesJurnal NewTatik HandayaniNo ratings yet
- Guía Preeclampsia IJGO 2019Document33 pagesGuía Preeclampsia IJGO 2019teresita vargasNo ratings yet
- NCM 109 Care of Mother and Child at RiskDocument10 pagesNCM 109 Care of Mother and Child at RiskMia Fe Cuaya Lorenzo100% (1)
- NCM 109 Care of Mother and Child at RiskDocument10 pagesNCM 109 Care of Mother and Child at RiskMia Fe Cuaya Lorenzo100% (1)
- Clinical Risk Factor For Preeclamsia in Twin PregnanciesDocument8 pagesClinical Risk Factor For Preeclamsia in Twin PregnanciesLouis HadiyantoNo ratings yet
- Blom Et Al-2010-BJOG - An International Journal of Obstetrics & GynaecologyDocument9 pagesBlom Et Al-2010-BJOG - An International Journal of Obstetrics & GynaecologyNeni RochmayatiNo ratings yet
- RM 12021Document4 pagesRM 12021liana devi oktaviaNo ratings yet
- Aynalem 2020@journal - Pone.0235544Document14 pagesAynalem 2020@journal - Pone.0235544Huệ MinhNo ratings yet
- Research: Anaemia in Pregnant Adolescent Girls With Malaria and Practicing PicaDocument13 pagesResearch: Anaemia in Pregnant Adolescent Girls With Malaria and Practicing PicaJaniezt Linggi AlloNo ratings yet
- 1 s2.0 S000293781502579XDocument6 pages1 s2.0 S000293781502579XsaryindrianyNo ratings yet
- Acute Pyelonephritis in Pregnancy: An 18-Year Retrospective AnalysisDocument6 pagesAcute Pyelonephritis in Pregnancy: An 18-Year Retrospective AnalysisIntan Wahyu CahyaniNo ratings yet
- Mor 2016Document9 pagesMor 2016Farin MauliaNo ratings yet
- Severity of Anemia During Pregnancy and Adverse Maternal and Fetal OutcomesDocument13 pagesSeverity of Anemia During Pregnancy and Adverse Maternal and Fetal OutcomesIlda IldaNo ratings yet
- Polyhydramnios and Oligohydramnios - Background, Pathophysiology, EtiologyDocument4 pagesPolyhydramnios and Oligohydramnios - Background, Pathophysiology, EtiologyAhmad FahroziNo ratings yet
- Deense Studie PDFDocument12 pagesDeense Studie PDFBas HermansNo ratings yet
- Intra Uterine Growth RetardationDocument46 pagesIntra Uterine Growth RetardationIba Ghannam100% (1)
- 298 FullDocument7 pages298 Fullmadimadi11No ratings yet
- Study On Outcomes of PROMDocument5 pagesStudy On Outcomes of PROMRohit MaliNo ratings yet
- Cerebral Palsy Among Children Born After in Vitro Fertilization: The Role of Preterm Delivery-A Population-Based, Cohort StudyDocument10 pagesCerebral Palsy Among Children Born After in Vitro Fertilization: The Role of Preterm Delivery-A Population-Based, Cohort StudyandriNo ratings yet
- Laas 2012 (Inglês)Document11 pagesLaas 2012 (Inglês)André Toga Machado CoelhoNo ratings yet
- Epidemiology and Initial Management of Ambiguous Genitalia at Birth in GermanyDocument9 pagesEpidemiology and Initial Management of Ambiguous Genitalia at Birth in GermanyFikri Abd AzisNo ratings yet
- IjgoDocument33 pagesIjgoInggrid OlyviaNo ratings yet
- AAP. Management of Neonates Born at Less 34 6 Weeks' Gestation With Suspected or Proven Early-Onset Bacterial Sepsis. Pediatrics.Document12 pagesAAP. Management of Neonates Born at Less 34 6 Weeks' Gestation With Suspected or Proven Early-Onset Bacterial Sepsis. Pediatrics.PEDRO MUNYOZ ALVAREZNo ratings yet
- Jsafog 13 137Document5 pagesJsafog 13 137Elizabeth Duprat GaxiolaNo ratings yet
- Gestational Diabetes Mellitus Is Associated With Adverse Outcomes in Twin PregnanciesDocument8 pagesGestational Diabetes Mellitus Is Associated With Adverse Outcomes in Twin PregnanciesDwi OktaviliaNo ratings yet
- The Origins of Cerebral Palsy: John M. Keogh and Nadia BadawiDocument6 pagesThe Origins of Cerebral Palsy: John M. Keogh and Nadia BadawiC_DanteNo ratings yet
- 3cleveland Clinic Journal of Medicine-2004-Meador-S38Document4 pages3cleveland Clinic Journal of Medicine-2004-Meador-S38Elok ZakiyyaNo ratings yet
- Knowledge On PIHDocument6 pagesKnowledge On PIHMadhusmita NayakNo ratings yet
- 04 Shehla20Noor 20PREVALANCE20OF20PRROM20AND20ITS20OUTCOMEDocument5 pages04 Shehla20Noor 20PREVALANCE20OF20PRROM20AND20ITS20OUTCOMEMirachel AugustNo ratings yet
- Old and New Anti-Epileptic Drugs in Pregnancy: Review ArticlesDocument6 pagesOld and New Anti-Epileptic Drugs in Pregnancy: Review ArticleskoesantoNo ratings yet
- Epidemiology and Causes of Preterm BirthDocument10 pagesEpidemiology and Causes of Preterm BirthCarlos Rojas CuevaNo ratings yet
- Food Protein Induced Enterocolitis (FPIES): Diagnosis and ManagementFrom EverandFood Protein Induced Enterocolitis (FPIES): Diagnosis and ManagementTerri Faye Brown-WhitehornNo ratings yet
- Ade Egie Prayogi - Perbaikan InggrisDocument6 pagesAde Egie Prayogi - Perbaikan InggrisAde Egie PrayogiNo ratings yet
- Veterinary Focus 2010 1enDocument49 pagesVeterinary Focus 2010 1enPetrisor GheorghiuNo ratings yet
- Natural ScienceDocument6 pagesNatural ScienceJandro KareemNo ratings yet
- International Ayurvedic Medical Journal: Review Article ISSN: 2320 5091 Impact Factor: 4.018Document4 pagesInternational Ayurvedic Medical Journal: Review Article ISSN: 2320 5091 Impact Factor: 4.018bandgar123No ratings yet
- Foodborne Botulism, A Case ReportDocument4 pagesFoodborne Botulism, A Case ReportAri SiswadiNo ratings yet
- Hand SanitizerDocument21 pagesHand SanitizerVitalis MbuyaNo ratings yet
- Antepartum HaemorrhageDocument13 pagesAntepartum HaemorrhagedanielNo ratings yet
- A Clinal Primer On Intellectual DisabilityDocument13 pagesA Clinal Primer On Intellectual DisabilityAra AzzahraNo ratings yet
- Sexually Transmitted Infections - Lecture NotesDocument10 pagesSexually Transmitted Infections - Lecture NotesMa. Loucel RodriguezNo ratings yet
- Iron Metabolism: DR Mukhtiar BaigDocument58 pagesIron Metabolism: DR Mukhtiar BaigdrmukhtiarbaigNo ratings yet
- PATH505PDocument11 pagesPATH505PMohsin SialNo ratings yet
- AntibioticDocument4 pagesAntibioticYadile D BenoitNo ratings yet
- C. Difficile-7Document7 pagesC. Difficile-7Suprakkash DasNo ratings yet
- ATELECTASISDocument4 pagesATELECTASISAshley Jane MacapayadNo ratings yet
- Certificates and FormatsDocument12 pagesCertificates and FormatsAnimesh PriyadarshiNo ratings yet
- Clinical Pharmacology Book 2018 1Document304 pagesClinical Pharmacology Book 2018 1Salman khanNo ratings yet
- AB ? Pre-Board Exam-1Document20 pagesAB ? Pre-Board Exam-1sdfghNo ratings yet
- Review Article: Conceptual Review On Vijaya (Cannabis Sativa Linn.) : A Forgotten AmbrosiaDocument10 pagesReview Article: Conceptual Review On Vijaya (Cannabis Sativa Linn.) : A Forgotten Ambrosiasiva RamNo ratings yet
- Understanding KwashiorkorDocument7 pagesUnderstanding KwashiorkorpraneethNo ratings yet
- Astrocytoma: Zagada, Timothy MDocument12 pagesAstrocytoma: Zagada, Timothy MleartaNo ratings yet
- Culture Throat SwabsDocument5 pagesCulture Throat SwabsDryn TorresNo ratings yet
- Drug Study (Vancomycin)Document4 pagesDrug Study (Vancomycin)Jared Niles SantosNo ratings yet
- Dressler's Syndrome Case ReportDocument3 pagesDressler's Syndrome Case ReportResearch ParkNo ratings yet
- BillaDocument5 pagesBillaZeeshan AfzalNo ratings yet
- Ciliate and FlagellatesDocument95 pagesCiliate and FlagellatesJohn AdvinculaNo ratings yet
- A 50-Year-Old Female With Quadriparesis Secondary To Viral Myositis: Unusual Presentation and Diagnostic ApproachDocument4 pagesA 50-Year-Old Female With Quadriparesis Secondary To Viral Myositis: Unusual Presentation and Diagnostic ApproachInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- 7.14 Fungi and Fungal DiseaseDocument25 pages7.14 Fungi and Fungal DiseaseFN FajrinNo ratings yet
- Surgery Rotation NotesDocument18 pagesSurgery Rotation NotesNadiim Rajabalee100% (2)
- Causes of Low Grade Fever in ChildrenDocument2 pagesCauses of Low Grade Fever in Childrenkarthivisu2009No ratings yet
- Perio - Classification of Periodontal DiseasesDocument7 pagesPerio - Classification of Periodontal DiseasesGlyndale CatalunaNo ratings yet