You might also like
- Apple Inc PresentationDocument17 pagesApple Inc PresentationurougeNo ratings yet
- Acls Study Guide 2016Document2 pagesAcls Study Guide 2016nova939100% (2)
- 5.ALS Algorithms TachycardiaDocument1 page5.ALS Algorithms TachycardiaMassimo Di BenedettoNo ratings yet
- Tachycardia AlgorythmDocument1 pageTachycardia AlgorythmUZNAPMNo ratings yet
- Tachycardia Algorithm 2021Document1 pageTachycardia Algorithm 2021Ravin DebieNo ratings yet
- Adult Tachycardia (With Pulse) AlgorithmDocument1 pageAdult Tachycardia (With Pulse) AlgorithmJames ChoiNo ratings yet
- G2015 Adult Tachycardia PDFDocument1 pageG2015 Adult Tachycardia PDFPlabber JuneNo ratings yet
- G2015 Adult Tachycardia PDFDocument1 pageG2015 Adult Tachycardia PDFibbs91No ratings yet
- Ecgs and Acute Cardiac Events: Yuniardi Alriyanto, MD Doris Sylvanus Hospital PalangkarayaDocument47 pagesEcgs and Acute Cardiac Events: Yuniardi Alriyanto, MD Doris Sylvanus Hospital PalangkarayaAuliaRusdiAllmuttaqienNo ratings yet
- 2010 Integrated Updated Circulation ACLS Tachycardia AlgorithmDocument1 page2010 Integrated Updated Circulation ACLS Tachycardia AlgorithmRyggie ComelonNo ratings yet
- Peri-Arrest ArrythmiaDocument14 pagesPeri-Arrest Arrythmiamohamed mowafeyNo ratings yet
- AlgorithmACLStachycardiawithapulse PDFDocument1 pageAlgorithmACLStachycardiawithapulse PDFDendy Frannuzul RamadhanNo ratings yet
- Tachycardia AlgorithmDocument1 pageTachycardia AlgorithmGideon BahuleNo ratings yet
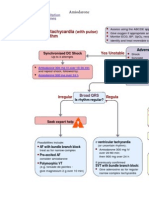
- Tachycardia With A Pulse Algorithm: Assess Appropriateness For Clinical ConditionDocument1 pageTachycardia With A Pulse Algorithm: Assess Appropriateness For Clinical ConditionDendy Frannuzul RamadhanNo ratings yet
- Assess Appropriateness For Clinical Condition. Heart Rate Typically 150/min If TachyarrhythmiaDocument1 pageAssess Appropriateness For Clinical Condition. Heart Rate Typically 150/min If TachyarrhythmiaSiti Nur R Firda FauziyahNo ratings yet
- Bra Dal GoDocument1 pageBra Dal Gozacklim_2000No ratings yet
- Adult Tachycardia Algorithm: (With Pulse)Document1 pageAdult Tachycardia Algorithm: (With Pulse)ITSimplyNo ratings yet
- Algo Tachycardia PDFDocument1 pageAlgo Tachycardia PDFYudhistira AdiNo ratings yet
- Managemen Disritmia: Dr. Rofika Hanifa, SPPDDocument20 pagesManagemen Disritmia: Dr. Rofika Hanifa, SPPDavivlabirdNo ratings yet
- Pediatric Tachycardia With A Pulse Algorithm: Yes NoDocument1 pagePediatric Tachycardia With A Pulse Algorithm: Yes NoRatna TambaNo ratings yet
- TachycardiaDocument7 pagesTachycardiaArvind SahniNo ratings yet
- Advanced Cardiac Life SupportDocument37 pagesAdvanced Cardiac Life SupportRoy Acosta GumbanNo ratings yet
- Obat-Obatan Dalam Bantuan Hidup LanjutDocument16 pagesObat-Obatan Dalam Bantuan Hidup LanjutTheresia SihotangNo ratings yet
- AdultTachycardiaWithPulse AlgorithmDocument1 pageAdultTachycardiaWithPulse AlgorithmIsmail SlimNo ratings yet
- ACLS Tachycardia Algorithm For Managing Stable TachycardiaDocument4 pagesACLS Tachycardia Algorithm For Managing Stable TachycardiaLady MuffinsNo ratings yet
- Adult Tachycardia With A Pulse Algorithm: Doses/DetailsDocument1 pageAdult Tachycardia With A Pulse Algorithm: Doses/DetailsAlexis HospitalNo ratings yet
- Adult Tachycardia With A Pulse Algorithm: Doses/DetailsDocument1 pageAdult Tachycardia With A Pulse Algorithm: Doses/DetailsZakiyahulfahdwNo ratings yet
- Tatalaksana ArrthytmiaDocument55 pagesTatalaksana ArrthytmiaJanstine FirstiandyNo ratings yet
- Acute Coronary SyndromeDocument7 pagesAcute Coronary SyndromePuskesmas Pinang JayaNo ratings yet
- AlgorithmACLS Tachycardia 200612Document1 pageAlgorithmACLS Tachycardia 200612must dietNo ratings yet
- Hippo EM Board Review - Bradycardia - A Simplified Approach Written Summary 2Document10 pagesHippo EM Board Review - Bradycardia - A Simplified Approach Written Summary 2alexandertorresreyNo ratings yet
- 26) Approach To Pediatric ArrhythmiasDocument44 pages26) Approach To Pediatric ArrhythmiasJude AlyousefNo ratings yet
- Pals TachycardiaDocument1 pagePals TachycardiadarlingcarvajalduqueNo ratings yet
- AlgorithmACLS Tachycardia 200612Document1 pageAlgorithmACLS Tachycardia 200612YassarNo ratings yet
- Nursing CS Treatment-Of-Atrial-Dysrhythmias 02Document1 pageNursing CS Treatment-Of-Atrial-Dysrhythmias 02frankshro156No ratings yet
- Arrhythmias: - Finot D., MD, MSC, Emergency Physician, CC FellowDocument43 pagesArrhythmias: - Finot D., MD, MSC, Emergency Physician, CC FellowKaleb DemisseNo ratings yet
- .JPG 958×1,280 PixelsDocument1 page.JPG 958×1,280 Pixelsyordanos getachewNo ratings yet
- Algoritmos AHA ACLS AdultoDocument4 pagesAlgoritmos AHA ACLS AdultoChristianFelipePorrasCastroNo ratings yet
- Periarestne AritmijeDocument10 pagesPeriarestne AritmijeMustafa ŠabićNo ratings yet
- Pharmacological Tools: Doses, Routes, and Uses of Common DrugDocument1 pagePharmacological Tools: Doses, Routes, and Uses of Common DrugApuntesdemedicinaa blogNo ratings yet
- Algo Pals TachycardiaDocument1 pageAlgo Pals TachycardiaArdie FratamaNo ratings yet
- Algorithm 1: Initial Evaluation and Management: Symptoms of Possible ACSDocument6 pagesAlgorithm 1: Initial Evaluation and Management: Symptoms of Possible ACSNenyNo ratings yet
- Arrhythmias: Clinical DiagnosisDocument4 pagesArrhythmias: Clinical DiagnosispaveethrahNo ratings yet
- ACLS Algorithm Pulse No Yes: Stable Patient Unstable Patient Stable PatientDocument1 pageACLS Algorithm Pulse No Yes: Stable Patient Unstable Patient Stable PatientAhmed AlkhaqaniNo ratings yet
- TachycardiaDocument12 pagesTachycardiaPuskesmas Pinang JayaNo ratings yet
- K31a - Electrophysiology and Cardiac Arrhytmia EmergencyDocument46 pagesK31a - Electrophysiology and Cardiac Arrhytmia EmergencyXeniel AlastairNo ratings yet
- Adult Tachycardia Algorithm: (With Pulse)Document1 pageAdult Tachycardia Algorithm: (With Pulse)ITSimplyNo ratings yet
- Website Tachycardia Algorithm DiagramDocument1 pageWebsite Tachycardia Algorithm Diagramcolette zgheibNo ratings yet
- Med II-LE1-1.03 Arrhythmia NotesDocument14 pagesMed II-LE1-1.03 Arrhythmia NotesAbigael SantosNo ratings yet
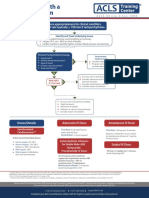
- Syndromes Suggestive of Ischemia or Infarction: EMS Assessment and Care and Hospital PreparationDocument1 pageSyndromes Suggestive of Ischemia or Infarction: EMS Assessment and Care and Hospital PreparationIGOR SHEYNINNo ratings yet
- Onlinemeded Notes CardioDocument1 pageOnlinemeded Notes CardioCourtney HolbrookNo ratings yet
- ACLS AritmiaDocument18 pagesACLS AritmiaZega AgustianNo ratings yet
- With A Pulse and Poor Perfusion: Pediatric TachycardiaDocument1 pageWith A Pulse and Poor Perfusion: Pediatric TachycardiaIin-Ignasia Diahayujulindah Mujiman0% (1)
- ACLS Algorithms Adult 2010Document12 pagesACLS Algorithms Adult 2010anon_336736395No ratings yet
- ACLS Simplify AlgorithmDocument6 pagesACLS Simplify AlgorithmKristine Monforte Coma UritaNo ratings yet
- EKG Quick and Dirty - GD v3.0Document2 pagesEKG Quick and Dirty - GD v3.0Sheema Sh100% (1)
- Wiggins Ijaied 2016Document24 pagesWiggins Ijaied 2016niwayannovita7564No ratings yet
- Fascination Roman PDFDocument2 pagesFascination Roman PDFKristelNo ratings yet
- 1.3 Formulae, Equations and Amounts of Substance: Relative Mass Relative ChargeDocument19 pages1.3 Formulae, Equations and Amounts of Substance: Relative Mass Relative ChargeRaiyan RahmanNo ratings yet
- Islcollective Worksheets Elementary A1 Preintermediate A2 Adult Elementary School High School Reading Speaking Writing M 46694f6b0efec48285 61900856Document3 pagesIslcollective Worksheets Elementary A1 Preintermediate A2 Adult Elementary School High School Reading Speaking Writing M 46694f6b0efec48285 61900856DaVinci PortoNo ratings yet
- ĐỀ THI THỬ SỐ 10- DÀNH CHO 2K5 6 7-BIÊN SOẠN CÔ PHẠM LIỄU NGÀY 23042023Document5 pagesĐỀ THI THỬ SỐ 10- DÀNH CHO 2K5 6 7-BIÊN SOẠN CÔ PHẠM LIỄU NGÀY 2304202336Hoàng Phạm Tiến Thành10A03No ratings yet
- STD 10th Iqb English Kumarbharati English Medium MH BoardDocument18 pagesSTD 10th Iqb English Kumarbharati English Medium MH BoardHarsh KumarNo ratings yet
- Adriana Espinosa - Avid 10 My Api GoalsDocument3 pagesAdriana Espinosa - Avid 10 My Api Goalsapi-460281338No ratings yet
- Bibliografía Central - Control AversivoDocument7 pagesBibliografía Central - Control Aversivojuan diegoNo ratings yet
- Belief in The Hereafter Sheikh Munawar Haque PDFDocument5 pagesBelief in The Hereafter Sheikh Munawar Haque PDFCahaya IslamiahNo ratings yet
- 200 Most Wanted Political Science MCQs (One Liner)Document9 pages200 Most Wanted Political Science MCQs (One Liner)SohailNo ratings yet
- Ma CF Naspe Standards-5Document9 pagesMa CF Naspe Standards-5api-249855828No ratings yet
- I Tonya Reflection Reaction PaperDocument2 pagesI Tonya Reflection Reaction PaperAlgen UbasaNo ratings yet
- 106-Wells Fargo Bank and Union vs. Collector 70 Phil 325Document4 pages106-Wells Fargo Bank and Union vs. Collector 70 Phil 325wewNo ratings yet
- Off-Centre Anchoring of AZ Sheet Pile WallsDocument18 pagesOff-Centre Anchoring of AZ Sheet Pile WallsjmmNo ratings yet
- What Do You Hear The Effect of Stadium Noise On Football Players Passing PerformancesDocument27 pagesWhat Do You Hear The Effect of Stadium Noise On Football Players Passing PerformancesJorge Rubio LópezNo ratings yet
- Should We Legalize Euthanasia?: Presenters: - Sarah Bamba Professor: DR G Eorges Gnakpa - Ingrid KragbeDocument11 pagesShould We Legalize Euthanasia?: Presenters: - Sarah Bamba Professor: DR G Eorges Gnakpa - Ingrid KragbeIngrid KragbeNo ratings yet
- What Are The Different Types of Solitaire?: Solitaire Spider Solitaire Solitaire OnlineDocument20 pagesWhat Are The Different Types of Solitaire?: Solitaire Spider Solitaire Solitaire OnlineSrijeetRoutrayNo ratings yet
- Bruce Lee - BiographyDocument7 pagesBruce Lee - BiographyLaishram PilotNo ratings yet
- Kamo How To Doodle Year Round Cute Super Easy Drawings For Holidays Celebrations and Special Events With Over 1000 Drawings Tuttle Publishing 2020Document132 pagesKamo How To Doodle Year Round Cute Super Easy Drawings For Holidays Celebrations and Special Events With Over 1000 Drawings Tuttle Publishing 2020Thao La ThuNo ratings yet
- Grammar Exercises: Active & Passive SentencesDocument3 pagesGrammar Exercises: Active & Passive SentencespuanroshNo ratings yet
- Phrasebank: A University-Wide Online Writing Resource: BackgroundDocument6 pagesPhrasebank: A University-Wide Online Writing Resource: BackgroundOlga SelkinaNo ratings yet
- CancerDocument81 pagesCancerCodered Review100% (1)
- East Asian MusicDocument32 pagesEast Asian MusicXyrone SolimanNo ratings yet
- Mistakes", Pays USD 12.9 Billion in "Settlement" For Money Laundering, Nobody Held Accountable..Document4 pagesMistakes", Pays USD 12.9 Billion in "Settlement" For Money Laundering, Nobody Held Accountable..Human Rights Alert - NGO (RA)No ratings yet
- Geri A AaaaaaaaaaaaDocument24 pagesGeri A AaaaaaaaaaaaCarl John Manalo100% (2)
- Prospectus BEd 2016 PunjabDocument51 pagesProspectus BEd 2016 PunjabDipanjanNo ratings yet
- Resume PDFDocument15 pagesResume PDFFida HussainNo ratings yet
- Chico Sees A GhostDocument7 pagesChico Sees A GhostSamantha HarrellNo ratings yet
- SQL NotesDocument40 pagesSQL NotesMounikaNo ratings yet