You might also like
- Physician Assistant PANCE & PANRE: a QuickStudy Laminated Reference GuideFrom EverandPhysician Assistant PANCE & PANRE: a QuickStudy Laminated Reference GuideNo ratings yet
- Introduction To History Taking Aims:: Summary of Procedure and NotesDocument6 pagesIntroduction To History Taking Aims:: Summary of Procedure and Notesmj.vinoth@gmail.comNo ratings yet
- First Aid ObGynDocument252 pagesFirst Aid ObGynineedsomebooksNo ratings yet
- History Taking NotesDocument7 pagesHistory Taking NotesZWEASNo ratings yet
- History TakingDocument3 pagesHistory TakingwegairnaniNo ratings yet
- How to behave on the wardsDocument252 pagesHow to behave on the wardssilasjubaNo ratings yet
- 3 Medical HistoryDocument101 pages3 Medical HistoryHamsawiNo ratings yet
- First Aid For The Obstetrics & Gynecology ClerkshipDocument253 pagesFirst Aid For The Obstetrics & Gynecology Clerkshipadereje7100% (1)
- Clinical History TakingDocument36 pagesClinical History Takingapi-1964133775% (4)
- NEUROPrelims - History Taking in NeurologyDocument4 pagesNEUROPrelims - History Taking in NeurologyRenatoCosmeGalvanJuniorNo ratings yet
- The Medical History: Herni SupraptiDocument101 pagesThe Medical History: Herni SupraptiPradika Abdi PutraNo ratings yet
- Dzinos MedicineDocument455 pagesDzinos MedicineCollen Lihaka100% (2)
- Robert Waldinger & Alan M. Jacobson: The Initial Psychiatric InterviewDocument4 pagesRobert Waldinger & Alan M. Jacobson: The Initial Psychiatric InterviewMari Forgach100% (1)
- Taking a comprehensive patient historyDocument23 pagesTaking a comprehensive patient historyNikky Rossel FloresNo ratings yet
- History Taking - The Critical First Step in DiagnosisDocument51 pagesHistory Taking - The Critical First Step in DiagnosisJAMES TONNY OKINYINo ratings yet
- History Taking Guide - 70% Diagnosis from Patient HistoryDocument51 pagesHistory Taking Guide - 70% Diagnosis from Patient HistoryJAMES TONNY OKINYINo ratings yet
- History Patient - Co.ukDocument14 pagesHistory Patient - Co.ukiuytrerNo ratings yet
- A Practical Guide to HPIDocument11 pagesA Practical Guide to HPIMichael NyaongoNo ratings yet
- OSCE Revision Guide for Clinical AssessmentsDocument66 pagesOSCE Revision Guide for Clinical AssessmentsApoorva SaxenaNo ratings yet
- PAL Pack 2011 KI UpdateDocument41 pagesPAL Pack 2011 KI UpdateLuveon TangNo ratings yet
- 10 The Rest of The HistoryDocument3 pages10 The Rest of The Historybeba macasinagNo ratings yet
- Foundations of Clinical Medicine-1 Summer 2014 Semester: History TakingDocument63 pagesFoundations of Clinical Medicine-1 Summer 2014 Semester: History Takingparanoea911100% (1)
- 2beginning The History Taking-1Document30 pages2beginning The History Taking-1Wizz Háķìm ĻêşòwNo ratings yet
- Taking The Medical HistoryDocument2 pagesTaking The Medical HistoryPaf VenancioNo ratings yet
- First Aid PsychiatryDocument156 pagesFirst Aid PsychiatryMae Matira AbeladorNo ratings yet
- Guide To History TakingDocument55 pagesGuide To History TakingGabriella Hild100% (1)
- History and Physical Examination: Medical ProfessionalsDocument10 pagesHistory and Physical Examination: Medical ProfessionalsGiorgio CivitareseNo ratings yet
- I. Approach To Clinical Interviewing and DiagnosisDocument6 pagesI. Approach To Clinical Interviewing and DiagnosisRoci ArceNo ratings yet
- The Initial Psychiatric Interview PDFDocument4 pagesThe Initial Psychiatric Interview PDFJoan ChoiNo ratings yet
- Psychiatry: Psychiatric Interview, Diagnosis, and Report OutlineDocument71 pagesPsychiatry: Psychiatric Interview, Diagnosis, and Report OutlineHamidNo ratings yet
- PhiDocument11 pagesPhiGitaq Tri YatmaNo ratings yet
- History of Present IllnessDocument10 pagesHistory of Present Illnesshirsi200518No ratings yet
- Clinical Exam. & History TakingDocument23 pagesClinical Exam. & History TakingManiish Trivedi100% (2)
- The-art-of-history-takingDocument54 pagesThe-art-of-history-takingChowdhury Shaheb MedicalwalaNo ratings yet
- Obtaining an Accurate Patient HistoryDocument5 pagesObtaining an Accurate Patient HistoryKumar KP100% (1)
- The Rubik's Cube Approach To Clinical MedicineDocument2 pagesThe Rubik's Cube Approach To Clinical Medicinehenrygoldstein100% (1)
- Examining a Surgical PatientDocument3 pagesExamining a Surgical Patientakash kumar panwarNo ratings yet
- General Principles of Gastroentorylogy.Document32 pagesGeneral Principles of Gastroentorylogy.hirsi200518No ratings yet
- Compiled Osce - r&c IIDocument73 pagesCompiled Osce - r&c IIFaisal MakkiNo ratings yet
- Comprehensive Respiratory InterviewDocument36 pagesComprehensive Respiratory InterviewDharlyn MungcalNo ratings yet
- Sexual History TakingDocument3 pagesSexual History TakingCheng XinvennNo ratings yet
- First Aid For The Obstetrics & Gynecology ClerkshipDocument253 pagesFirst Aid For The Obstetrics & Gynecology ClerkshipSimona Prodanoiu100% (17)
- Patient History: Objectives Building RapportDocument15 pagesPatient History: Objectives Building RapportAnonymous 23ghm1No ratings yet
- 5-1 HX & Exam Handbook Final PDFDocument23 pages5-1 HX & Exam Handbook Final PDFPépé TechopathamNo ratings yet
- Carte Anamneza Si TestareDocument100 pagesCarte Anamneza Si TestareNarcis PopaNo ratings yet
- Reflection 1Document3 pagesReflection 1api-502171898No ratings yet
- Physician Patient Communication 2018 Handout-1Document35 pagesPhysician Patient Communication 2018 Handout-1Majid KhanNo ratings yet
- Case Presentation CompleteDocument46 pagesCase Presentation CompleteClaireNo ratings yet
- Breaking Bad NewsDocument33 pagesBreaking Bad Newszonia kilashNo ratings yet
- SPIKES ProtocolDocument4 pagesSPIKES ProtocolKassem Gharaibeh100% (1)
- Delivering Bad News Sensitively Using the SPIKES ProtocolDocument4 pagesDelivering Bad News Sensitively Using the SPIKES ProtocolHussam KabakbjiNo ratings yet
- Seminar 3 1Document16 pagesSeminar 3 1Maya BendelianiNo ratings yet
- AnamnesisDocument6 pagesAnamnesisfienny37100% (1)
- MSE and History TakingDocument17 pagesMSE and History TakingGeetika Chutani18No ratings yet
- Medical Investigation 101: A Book to Inspire Your Interest in Medicine and How Doctors ThinkFrom EverandMedical Investigation 101: A Book to Inspire Your Interest in Medicine and How Doctors ThinkNo ratings yet
- CSA Revision Notes for the MRCGP, second editionFrom EverandCSA Revision Notes for the MRCGP, second editionRating: 4.5 out of 5 stars4.5/5 (3)
- Transcript IngleseDocument4 pagesTranscript IngleseGiorgio CivitareseNo ratings yet
- Transcript IngleseDocument4 pagesTranscript IngleseGiorgio CivitareseNo ratings yet
- Records), Patient Identification: Name, Gender, Birth Date and Demographic Data, AsDocument4 pagesRecords), Patient Identification: Name, Gender, Birth Date and Demographic Data, AsGiorgio CivitareseNo ratings yet
- With Your Fellow Students and Then Present Your Work and Conclusions in An English Exam?Document4 pagesWith Your Fellow Students and Then Present Your Work and Conclusions in An English Exam?Giorgio CivitareseNo ratings yet
- 28 1.3. Timelines: A Comparative AnalysisDocument12 pages28 1.3. Timelines: A Comparative AnalysisGiorgio CivitareseNo ratings yet
- Viewership Replaces Readership as Basic Textual ActivityDocument5 pagesViewership Replaces Readership as Basic Textual ActivityGiorgio CivitareseNo ratings yet
- 42 2.1. Medical Records: Social and Textual OrganisationDocument12 pages42 2.1. Medical Records: Social and Textual OrganisationGiorgio CivitareseNo ratings yet
- Language and Publication in Cardiovascular Research ArticlesDocument7 pagesLanguage and Publication in Cardiovascular Research ArticlesGiorgio CivitareseNo ratings yet
- Grafici 4Document9 pagesGrafici 4Giorgio CivitareseNo ratings yet
- Case Report - Articular AspergillosisDocument3 pagesCase Report - Articular AspergillosisGiorgio CivitareseNo ratings yet
- History and Physical Examination: Medical ProfessionalsDocument10 pagesHistory and Physical Examination: Medical ProfessionalsGiorgio CivitareseNo ratings yet
- Resisted ExerciseDocument29 pagesResisted ExerciseVaraNo ratings yet
- General Hospital Philosophy and ObjectivesDocument26 pagesGeneral Hospital Philosophy and ObjectivesTanu GulatiNo ratings yet
- List of Beed Researchers 2 Semester SY 2020-2021 Beed-ADocument5 pagesList of Beed Researchers 2 Semester SY 2020-2021 Beed-AAndamin MalaNo ratings yet
- Awarness About Breast CancerDocument4 pagesAwarness About Breast CancerliaahlanNo ratings yet
- Persuasive Speech TextDocument2 pagesPersuasive Speech TextAnindya Azzahra0% (1)
- Types of Solder FluxDocument6 pagesTypes of Solder Fluxpeter paulNo ratings yet
- A Study On Environmental Impact of Madukkarai Limestone Mine, CoimbatoreDocument11 pagesA Study On Environmental Impact of Madukkarai Limestone Mine, CoimbatoreRamasamyNagarajan100% (1)
- Melidiosis FDocument24 pagesMelidiosis FVyramuthu AtputhanNo ratings yet
- Cea SDocument10 pagesCea Syousra zeidanNo ratings yet
- Petroleum Gases, Liquefied Petroleum Gas: IdentificationDocument4 pagesPetroleum Gases, Liquefied Petroleum Gas: IdentificationdigecaNo ratings yet
- VGEC 2024_Thư mời hội nghịDocument8 pagesVGEC 2024_Thư mời hội nghịkhongquantam101010No ratings yet
- Top 5 Consumer Court CasesDocument7 pagesTop 5 Consumer Court CasesTanishka SoniNo ratings yet
- Leni Robredo CredentialsDocument2 pagesLeni Robredo CredentialsJhelliene Rose V. De CastroNo ratings yet
- Psychopathic Personality: Bridging The Gap Between Scientific Evidence and Public PolicyDocument69 pagesPsychopathic Personality: Bridging The Gap Between Scientific Evidence and Public PolicyGokushimakNo ratings yet
- Nursing and Midwifery Board Candidate Handbook RN OSCE ExaminationDocument25 pagesNursing and Midwifery Board Candidate Handbook RN OSCE ExaminationkemalayazNo ratings yet
- EBM TerbaruDocument5 pagesEBM TerbaruTetty PrasetyaNo ratings yet
- 3075 SWMS RendererDocument13 pages3075 SWMS Renderernik KooNo ratings yet
- Change Your Life in 7 Days With NLP - Paul Mckenna BrochureDocument2 pagesChange Your Life in 7 Days With NLP - Paul Mckenna Brochureapi-385316675% (4)
- TWC Final Settlement DocsDocument374 pagesTWC Final Settlement DocsTHROnlineNo ratings yet
- The Effect of Potassium Permanganate (KMnO4) Concentration and Storage Time on Quality of California Papaya (Carica papaya LDocument8 pagesThe Effect of Potassium Permanganate (KMnO4) Concentration and Storage Time on Quality of California Papaya (Carica papaya LSyifa UlNo ratings yet
- AOTA Statement On Role of OT in NICUDocument9 pagesAOTA Statement On Role of OT in NICUMapi RuizNo ratings yet
- 100 Item Exam On Fundamentals of Nursing - Pulse - Blood Pressure PDFDocument12 pages100 Item Exam On Fundamentals of Nursing - Pulse - Blood Pressure PDFJawad AkbarNo ratings yet
- UKHO Survey Specification Acoustic V3 Jul18Document102 pagesUKHO Survey Specification Acoustic V3 Jul18Iqbal FauzanNo ratings yet
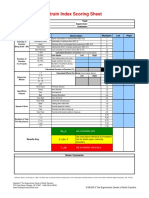
- Strain Index Scoring Sheet: Date: Task: Company: Supervisor: Dept: EvaluatorDocument1 pageStrain Index Scoring Sheet: Date: Task: Company: Supervisor: Dept: EvaluatorUdaydeep SinghNo ratings yet
- Rizzuto God MindDocument22 pagesRizzuto God MindSpats65No ratings yet
- Meat Inspection Certificate For Export of Pork/Pork Products To MalaysiaDocument2 pagesMeat Inspection Certificate For Export of Pork/Pork Products To MalaysiaLingSiewyingNo ratings yet
- Multi-Omic Machine Learning Predictor of Breast Cancer Therapy ResponseDocument28 pagesMulti-Omic Machine Learning Predictor of Breast Cancer Therapy ResponseSobek1789No ratings yet
- Central Pain Syndrome - Pathophysiol., Diag., Mgmt. - S. Canavero, Et. Al., (Cambridge, 2006) WW PDFDocument398 pagesCentral Pain Syndrome - Pathophysiol., Diag., Mgmt. - S. Canavero, Et. Al., (Cambridge, 2006) WW PDFRomeo-Remus RaffaiNo ratings yet
- 2023 AHAR: PIT Estimates of Homelessness in The U.S.Document117 pages2023 AHAR: PIT Estimates of Homelessness in The U.S.Santiago Adolfo OspitalNo ratings yet
- (Bio 024) Lab Activity 12 - BloodDocument9 pages(Bio 024) Lab Activity 12 - Bloodelaq dr100% (1)