You might also like
- Tear Film OrientedDocument13 pagesTear Film OrientedPutri kartiniNo ratings yet
- Limbal Stem Cell Deficiency EtDocument45 pagesLimbal Stem Cell Deficiency EtPutri kartiniNo ratings yet
- Modern Approach To The Treatment of Dry EyeDocument8 pagesModern Approach To The Treatment of Dry EyePutri kartiniNo ratings yet
- Ocular Surface DiseaseDocument450 pagesOcular Surface DiseasePutri kartini100% (1)
- Dry Eye and Ocular Surface DisordersDocument363 pagesDry Eye and Ocular Surface DisordersPutri kartiniNo ratings yet
- Surgery For Glaucoma in Patients With Facial Port Wine MarkDocument6 pagesSurgery For Glaucoma in Patients With Facial Port Wine MarkPutri kartiniNo ratings yet
- Dapus Jurnal 3 INTRAVITREOUS CHEMOTHERAPY FORDocument7 pagesDapus Jurnal 3 INTRAVITREOUS CHEMOTHERAPY FORPutri kartiniNo ratings yet
- Effect of Initial Prednisone Dosing On Ocular.47Document5 pagesEffect of Initial Prednisone Dosing On Ocular.47Putri kartiniNo ratings yet
- Heidary 2020Document5 pagesHeidary 2020Putri kartiniNo ratings yet
- Normal Values For The Pelli-RobsonDocument6 pagesNormal Values For The Pelli-RobsonPutri kartiniNo ratings yet
- Modified Y - Split and Recession ofDocument8 pagesModified Y - Split and Recession ofPutri kartiniNo ratings yet
- Effect of Unilateral VerticalDocument5 pagesEffect of Unilateral VerticalPutri kartiniNo ratings yet
- Soal AAO 2 PD 2022Document3 pagesSoal AAO 2 PD 2022Putri kartiniNo ratings yet
- Orbital Radiation Therapy For Graves OphthalmopatDocument8 pagesOrbital Radiation Therapy For Graves OphthalmopatPutri kartiniNo ratings yet
- Corticosteroids For Periorbital and Orbital Cellulitis (Protocol)Document23 pagesCorticosteroids For Periorbital and Orbital Cellulitis (Protocol)Putri kartiniNo ratings yet
- The Berkeley Rudimentary Vision Test: Original ArticleDocument8 pagesThe Berkeley Rudimentary Vision Test: Original ArticlePutri kartiniNo ratings yet
- Assessing A Modified Fitting Approach For Improved Multifocal Contact LensDocument6 pagesAssessing A Modified Fitting Approach For Improved Multifocal Contact LensPutri kartiniNo ratings yet
- Visual Performance of Daily-Disposable Multifocal Soft ContactDocument9 pagesVisual Performance of Daily-Disposable Multifocal Soft ContactPutri kartiniNo ratings yet
- Comparison of Corneal Biomechanical Properties Among AxialDocument8 pagesComparison of Corneal Biomechanical Properties Among AxialPutri kartiniNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- FACEBOWDocument30 pagesFACEBOWHarini PadmanabhanNo ratings yet
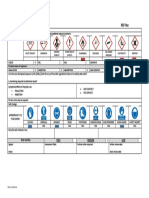
- GP 44.0 Coshh Risk Assessment FormDocument1 pageGP 44.0 Coshh Risk Assessment FormLarbi BelazizNo ratings yet
- TDSB GR 9-12 Student Census, 2022Document31 pagesTDSB GR 9-12 Student Census, 2022True NorthNo ratings yet
- 28,29 Management of Cardiac ArrhythmiasDocument41 pages28,29 Management of Cardiac ArrhythmiasSL Dr ChEMiSNo ratings yet
- Macscore SheetDocument2 pagesMacscore SheetIma HishamNo ratings yet
- Workplan in Project KalingaDocument2 pagesWorkplan in Project KalingaJholeen Mendoza Alegro-Ordoño100% (1)
- Effect of Xylitol With Various Concentration and Duration On The Growth of Candida Albicans (In Vitro Study)Document5 pagesEffect of Xylitol With Various Concentration and Duration On The Growth of Candida Albicans (In Vitro Study)gien fortunasiaNo ratings yet
- MediCover Graduate StandardDocument28 pagesMediCover Graduate StandardNhung LuuNo ratings yet
- Material Safety Data Sheet Lubricating OilDocument2 pagesMaterial Safety Data Sheet Lubricating OilBhavinNo ratings yet
- Poptropica Level1 Student BookDocument4 pagesPoptropica Level1 Student BookAnna Borodina0% (1)
- Chapter 5 - The Research DesignDocument14 pagesChapter 5 - The Research DesignmarlianaNo ratings yet
- Les 3 IELTS WRITING Task 2 - Food WasteDocument4 pagesLes 3 IELTS WRITING Task 2 - Food WasteĐỗ Huy HùngNo ratings yet
- Clinical Neuroscience Psychopathology and The Brain 2Nd Edition Full ChapterDocument41 pagesClinical Neuroscience Psychopathology and The Brain 2Nd Edition Full Chapterwilliam.kellar832100% (20)
- Memorandum: Philippine National Police Training Institute Regional Training Center 8Document2 pagesMemorandum: Philippine National Police Training Institute Regional Training Center 8DUN SAMMUEL LAURENTENo ratings yet
- Axis III GMCDocument4 pagesAxis III GMCFasya GhaffarNo ratings yet
- Faktor-Faktor Yang Berhubungan Dengan Ketajaman Penglihatan Pada Pelajar Sekolah Dasar Negeri 07 Pondok Labu Jakarta SelatanDocument9 pagesFaktor-Faktor Yang Berhubungan Dengan Ketajaman Penglihatan Pada Pelajar Sekolah Dasar Negeri 07 Pondok Labu Jakarta Selatanridhwan khalid06No ratings yet
- Hosp Study MMH2Document26 pagesHosp Study MMH2Bhell MendiolaNo ratings yet
- Entrepreneurial MotivationDocument11 pagesEntrepreneurial Motivationsagar0989% (9)
- Gyne Book 20122Document194 pagesGyne Book 20122თამარ ჩალაურიNo ratings yet
- ATHI InstrumentDocument3 pagesATHI InstrumentmarfloparNo ratings yet
- Thesis StatementDocument15 pagesThesis StatementJos50% (2)
- Rpms Evaluation For School Head (Mov'S / Mfo'S)Document5 pagesRpms Evaluation For School Head (Mov'S / Mfo'S)Laiza Niña Gimenez LariegoNo ratings yet
- Using Secondary Data in Doctoral Research: by Jim Goes and Marilyn SimonDocument3 pagesUsing Secondary Data in Doctoral Research: by Jim Goes and Marilyn SimonSon AdamNo ratings yet
- Zellies CMCSbooklet 2016 SingleDocument16 pagesZellies CMCSbooklet 2016 SinglezauserNo ratings yet
- Post-Test Questions - Act 31 TrainingDocument5 pagesPost-Test Questions - Act 31 TrainingJohn Gavazzi0% (1)
- WNL Junk Food Marketing at The Olympics UppDocument5 pagesWNL Junk Food Marketing at The Olympics UppAndrzejNo ratings yet
- Cramer (1991) - Development of Defense MechanismDocument19 pagesCramer (1991) - Development of Defense MechanismMaesNo ratings yet
- Lesson Title: The Food Pyramid and The Food Plate: ReferencesDocument2 pagesLesson Title: The Food Pyramid and The Food Plate: ReferencesKeanne Dhilan CabansagNo ratings yet
- Rad 97Document188 pagesRad 97Ahmed BadranNo ratings yet
- Acog Committee Opinion No 766 2018 PDFDocument10 pagesAcog Committee Opinion No 766 2018 PDFDaniel AnatoNo ratings yet