You might also like
- QuWave Product PricelistDocument3 pagesQuWave Product PricelistOstromafNo ratings yet
- Inguinal Scrotal SwellingsDocument23 pagesInguinal Scrotal SwellingsAzmyza Azmy100% (1)
- Ust Mock Boards 2017 - Anatomy-1Document10 pagesUst Mock Boards 2017 - Anatomy-1Jason Mirasol100% (1)
- Physics and AnaesthesiaDocument6 pagesPhysics and AnaesthesiaSuresh Kumar100% (1)
- Transcript (Intern) - CharlesDocument3 pagesTranscript (Intern) - CharlesCecille AnnNo ratings yet
- Chemical Pathology Lecture NotesDocument454 pagesChemical Pathology Lecture NotesHigh EducationNo ratings yet
- Low Flow AnesthesiaDocument92 pagesLow Flow Anesthesiaeliezer_89100% (1)
- Pathology For The Health Professions 5th Edition Damjanov Solutions ManualDocument35 pagesPathology For The Health Professions 5th Edition Damjanov Solutions Manualmamalukeadaunt0icji0100% (12)
- Comparison of Three Different Humidification Systems During Prolonged Mechanical VentilationDocument7 pagesComparison of Three Different Humidification Systems During Prolonged Mechanical VentilationAmit KumarNo ratings yet
- Short Term Effect of An Active Heat and Moisture Exchanger During Invasive VentilationDocument7 pagesShort Term Effect of An Active Heat and Moisture Exchanger During Invasive VentilationekaNo ratings yet
- Tre Differenti Sistemi Di Umidificazione A Confronto Durante Ventilazione Meccanica ProlungataDocument7 pagesTre Differenti Sistemi Di Umidificazione A Confronto Durante Ventilazione Meccanica ProlungataMatteo BrambatiNo ratings yet
- HFCN IgdDocument6 pagesHFCN IgdayuniNo ratings yet
- Rbti 29 02 0163Document8 pagesRbti 29 02 0163fgomezvNo ratings yet
- Performance of Different Active Humidification Systems in High-Flow Oxygen TherapyDocument8 pagesPerformance of Different Active Humidification Systems in High-Flow Oxygen TherapyJulieta EvangelistaNo ratings yet
- Automation of Ventilator Control For Hyperbaric Oxygen TherapyDocument2 pagesAutomation of Ventilator Control For Hyperbaric Oxygen Therapyra5tr@No ratings yet
- CrirmiDocument6 pagesCrirmistanleyNo ratings yet
- IcmhumidificacinenvniDocument8 pagesIcmhumidificacinenvniGinaNo ratings yet
- Rebreathing Anesthetic Systems in Small Animal PracticeDocument8 pagesRebreathing Anesthetic Systems in Small Animal PracticeAkın SeverNo ratings yet
- Leung Et Al 2007 AnaesthesiaDocument4 pagesLeung Et Al 2007 AnaesthesiafairuzNo ratings yet
- 046 - SV 2008 3 Suppl 1 S 33 - 36Document4 pages046 - SV 2008 3 Suppl 1 S 33 - 36Lee SakieNo ratings yet
- Online Data Supplement For:: 1. Extended Methods 1.1 Breath CollectionDocument8 pagesOnline Data Supplement For:: 1. Extended Methods 1.1 Breath CollectionSilvermist EiceliNo ratings yet
- 2016-Araos J-Extracorporeal Membrane Oxygenation Improves Survival in A Novel 24-Hour Pig Model of Severe Acute Respiratory Distress SyndromeDocument13 pages2016-Araos J-Extracorporeal Membrane Oxygenation Improves Survival in A Novel 24-Hour Pig Model of Severe Acute Respiratory Distress SyndromePablo Tapia BatallaNo ratings yet
- Anaesthesia - July 1996 - McCormick - Oxygen Saturation of Patients Recovering From Electroconvulsive TherapyDocument3 pagesAnaesthesia - July 1996 - McCormick - Oxygen Saturation of Patients Recovering From Electroconvulsive Therapyakthamsa15No ratings yet
- 231 FullDocument6 pages231 FullSuman DeyNo ratings yet
- Sputum Rheology Changes in Cystic Fibrosis Lung Disease Following Two Different Types of PhysiotherapyDocument7 pagesSputum Rheology Changes in Cystic Fibrosis Lung Disease Following Two Different Types of PhysiotherapyConstanza Martinez ArancibiaNo ratings yet
- Original Article: Doi: 10.1017/S0265021506001888Document7 pagesOriginal Article: Doi: 10.1017/S0265021506001888SherifMohamedNo ratings yet
- Bmri2016 3068467Document5 pagesBmri2016 3068467atika sgrtNo ratings yet
- The Use of Manual Hyperinflation in Airway Clearance: Series "Chest Physiotherapy" Edited by S.L. Hill and B. WebberDocument8 pagesThe Use of Manual Hyperinflation in Airway Clearance: Series "Chest Physiotherapy" Edited by S.L. Hill and B. WebberHello RainbowNo ratings yet
- Low Flow 210x260 WP 9105175 en Us 1801 1 K2Document5 pagesLow Flow 210x260 WP 9105175 en Us 1801 1 K2dmandatari7327No ratings yet
- Effects of High-Flow Nasal Cannula On End-Expiratory Lung Impedance in Semi-Seated Healthy SubjectsDocument8 pagesEffects of High-Flow Nasal Cannula On End-Expiratory Lung Impedance in Semi-Seated Healthy SubjectsJulieta EvangelistaNo ratings yet
- Beaussier1998 Article ComparativeEffectsOfDesfluraneDocument6 pagesBeaussier1998 Article ComparativeEffectsOfDesfluraneMinaz PatelNo ratings yet
- BF01705040Document4 pagesBF01705040fgomezvNo ratings yet
- CO Inhalation at Dose Corresponding To Tobacco Smoke Worsens Cardiac Remodeling After Experimental Myocardial Infarction in RatsDocument7 pagesCO Inhalation at Dose Corresponding To Tobacco Smoke Worsens Cardiac Remodeling After Experimental Myocardial Infarction in RatsGael ROCHEFORTNo ratings yet
- A Clinical Randomized Study On The Effects of Invasive Monitoring On Burn Shock ResuscitationDocument10 pagesA Clinical Randomized Study On The Effects of Invasive Monitoring On Burn Shock ResuscitationHusni maiyantiNo ratings yet
- Case PresentationDocument5 pagesCase PresentationJARIETTA OCHOANo ratings yet
- Oxygen TerapyDocument6 pagesOxygen TerapyCamila AgudeloNo ratings yet
- Original ArticleDocument11 pagesOriginal ArticlePablo Tapia BatallaNo ratings yet
- Review Article: Humidification During Mechanical Ventilation in The Adult PatientDocument13 pagesReview Article: Humidification During Mechanical Ventilation in The Adult Patientdan iacobNo ratings yet
- Effects of Prone Position On Alveolar Dead Space and Gas Exchange During General Anaesthesia in Surgery of Long DurationDocument7 pagesEffects of Prone Position On Alveolar Dead Space and Gas Exchange During General Anaesthesia in Surgery of Long Durationniketut tiniutamiNo ratings yet
- 1063 FullDocument2 pages1063 FullJossue LopezNo ratings yet
- Exposure Assessment To Trichloroethylene and Perchloroethylene For Workers in The Dry Cleaning IndustryDocument5 pagesExposure Assessment To Trichloroethylene and Perchloroethylene For Workers in The Dry Cleaning IndustryLaura Alejandra Beltrán DazaNo ratings yet
- LowflowanesthesiaDocument3 pagesLowflowanesthesiaJossue LopezNo ratings yet
- 7 Parolo & Onesta Tecar in Acute & Chronic Musculo Skeletal Lesions 60 Patient SeriesDocument6 pages7 Parolo & Onesta Tecar in Acute & Chronic Musculo Skeletal Lesions 60 Patient SeriesSilvia PluisNo ratings yet
- Low Flow Anestesi 5 Juli 2022 NewDocument34 pagesLow Flow Anestesi 5 Juli 2022 Newrahmanrais91No ratings yet
- Mechanical Ventilation HumidificationDocument4 pagesMechanical Ventilation HumidificationekaNo ratings yet
- 10.5372 1905-7415.0903.407Document7 pages10.5372 1905-7415.0903.407Kevin FeigeNo ratings yet
- IJPCR, Vol 15, Issue 9, Article 245Document5 pagesIJPCR, Vol 15, Issue 9, Article 245Jaldeep PatelNo ratings yet
- Influence of and Humidity The Obstruction By: Airway Induced Exercise AsthmaDocument8 pagesInfluence of and Humidity The Obstruction By: Airway Induced Exercise AsthmaiulyyNo ratings yet
- H (HBOT) (AD) : Olish Yperbaric EsearchDocument6 pagesH (HBOT) (AD) : Olish Yperbaric EsearchVera MHNo ratings yet
- Use of Early Extra-Corporeal Membrane Oxygenation (ECMO) For Severe Refractory Status AsthmaticusDocument3 pagesUse of Early Extra-Corporeal Membrane Oxygenation (ECMO) For Severe Refractory Status Asthmaticusintanlidyawati26gmaiNo ratings yet
- Eosinophilic Bronchitis Is An Important Cause of Chronic CoughDocument5 pagesEosinophilic Bronchitis Is An Important Cause of Chronic CoughNurfitrianti ArfahNo ratings yet
- Mechanical Ventilation Knowledge-Feedback: Case1 QuestionsDocument19 pagesMechanical Ventilation Knowledge-Feedback: Case1 QuestionsArtem 521No ratings yet
- Park Et Al 2005 Effect of Fresh Gas Flow On Isoflurane Concentrations During Low Flow AnaesthesiaDocument7 pagesPark Et Al 2005 Effect of Fresh Gas Flow On Isoflurane Concentrations During Low Flow AnaesthesiaBaha MirzaeifarNo ratings yet
- Fuzzy Logic Control of Mechanical Ventilation During AnaesthesiaDocument6 pagesFuzzy Logic Control of Mechanical Ventilation During AnaesthesiaTeki ChweNo ratings yet
- 10 11648 J Ajim 20190701 13Document3 pages10 11648 J Ajim 20190701 13Anonymous 8w9QEGNo ratings yet
- Alergia Al LatexDocument4 pagesAlergia Al Latexpaulina7escandarNo ratings yet
- 161111163114Document31 pages161111163114lejizixNo ratings yet
- Inflamt VMDocument6 pagesInflamt VMDiana Reaño RuizNo ratings yet
- 5432 D 9590 CF 225 BDDCC 85 B 42Document6 pages5432 D 9590 CF 225 BDDCC 85 B 42Jossue LopezNo ratings yet
- 1951 - Herxheimer - Induced Asthma in ManDocument5 pages1951 - Herxheimer - Induced Asthma in Manpond_1993No ratings yet
- Do Commonly Used Ventilator SettingsDocument6 pagesDo Commonly Used Ventilator Settingsnatalia muñozNo ratings yet
- Dreyfuss 1985 VentilatorDocument5 pagesDreyfuss 1985 Ventilatorgyroscope channelNo ratings yet
- HOUGH 2014 - Lung Recruitment and Endotracheal Suction in Ventilated Preterm Infants Measured With Electrical Impedance TomographyDocument7 pagesHOUGH 2014 - Lung Recruitment and Endotracheal Suction in Ventilated Preterm Infants Measured With Electrical Impedance TomographyRafael JustinoNo ratings yet
- Use Less: Model MS The Part, Be Our 3 Schedule. We Parts Will BeDocument2 pagesUse Less: Model MS The Part, Be Our 3 Schedule. We Parts Will BeAmalina Izati Nur IbrahimNo ratings yet
- 1 s2.0 S0104001421002037 MainDocument7 pages1 s2.0 S0104001421002037 MainFarhana MardilaNo ratings yet
- The Michigan Appropriateness Guide For Intravenous Catheters (MAGIC) : Results From A Multispecialty Panel Using The RAND/UCLA Appropriateness MethodDocument48 pagesThe Michigan Appropriateness Guide For Intravenous Catheters (MAGIC) : Results From A Multispecialty Panel Using The RAND/UCLA Appropriateness Methodnanang criztaNo ratings yet
- 2008 Evolution of Mechanical Ventilation in Response ToDocument8 pages2008 Evolution of Mechanical Ventilation in Response Tonanang criztaNo ratings yet
- 2 6 8 Offer Letter - WrestiDocument1 page2 6 8 Offer Letter - Wrestinanang criztaNo ratings yet
- Laryngoscopes e RevFDocument16 pagesLaryngoscopes e RevFnanang criztaNo ratings yet
- Lowongan Kerja MarketingDocument2 pagesLowongan Kerja Marketingnanang criztaNo ratings yet
- Rancangan Program Refresh Training Kariadi-RevisiDocument2 pagesRancangan Program Refresh Training Kariadi-Revisinanang criztaNo ratings yet
- 43 Adaptive Support Ventilation As VDocument5 pages43 Adaptive Support Ventilation As Vnanang criztaNo ratings yet
- The Cell As The Basic Unit of LifeDocument8 pagesThe Cell As The Basic Unit of LifeCarlo Joseph MoskitoNo ratings yet
- Endocrine Emergencies: Glucose Metabolism DisordersDocument23 pagesEndocrine Emergencies: Glucose Metabolism DisordersJoaquim RodriguezNo ratings yet
- Logbook Biochemistry Intake Sept 2015 EditedDocument40 pagesLogbook Biochemistry Intake Sept 2015 EditedRamesh Babu Manivannan100% (1)
- Chapter 4 B Inhibition of Enzyme Activity 3rd Year Chemistry Dep'tDocument21 pagesChapter 4 B Inhibition of Enzyme Activity 3rd Year Chemistry Dep'telsaNo ratings yet
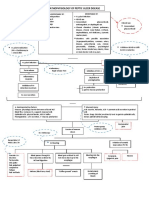
- POMR HydrocephalusDocument22 pagesPOMR HydrocephalusPutri YektiNo ratings yet
- 1.cardiac CycleDocument43 pages1.cardiac CycleNatasha Grace NtembwaNo ratings yet
- Class 10 Cbse Science Sample Paper Term 1 Model 2Document11 pagesClass 10 Cbse Science Sample Paper Term 1 Model 2Sunaina RawatNo ratings yet
- Clinical Teaching Birth InjuriesDocument15 pagesClinical Teaching Birth InjuriesAjit M Prasad PrasadNo ratings yet
- Judde and Rickard 2010 The Effect of Post-Learning Presentation of Music On Long-Term Word-List RetentionDocument8 pagesJudde and Rickard 2010 The Effect of Post-Learning Presentation of Music On Long-Term Word-List RetentionCande CastroNo ratings yet
- Clavicle FracturesDocument14 pagesClavicle FracturesKevin KusumanNo ratings yet
- Neurological Assessment ChartDocument5 pagesNeurological Assessment ChartshodhgangaNo ratings yet
- Principles of Biology 4Th Edition Robert J Brooker 2 All ChapterDocument67 pagesPrinciples of Biology 4Th Edition Robert J Brooker 2 All Chapterjoel.maccarone300100% (2)
- Peptic Ulcer Disease Pathogenesis Risk FactorsDocument1 pagePeptic Ulcer Disease Pathogenesis Risk FactorsKEn PilapilNo ratings yet
- A1C InfographicDocument1 pageA1C Infographiclewisch81No ratings yet
- 3 Skeletal SystemDocument58 pages3 Skeletal SystemFareez HamidNo ratings yet
- (Healthy Ageing and Longevity, 18) Anita Jagota - Sleep and Clocks in Aging and Longevity-Springer (2023)Document552 pages(Healthy Ageing and Longevity, 18) Anita Jagota - Sleep and Clocks in Aging and Longevity-Springer (2023)amrjano.ajNo ratings yet
- Jurnal FunggalDocument11 pagesJurnal FunggalAnastasio HarimbaNo ratings yet
- Gram Staining Protocol or ProcedureDocument4 pagesGram Staining Protocol or Procedurearavindbt2523No ratings yet
- Chapter 4 Basic Principles of Animal Form and FunctionDocument44 pagesChapter 4 Basic Principles of Animal Form and FunctionPrince VillacrusisNo ratings yet
- Endocrine GlandsDocument19 pagesEndocrine Glandscale suarezNo ratings yet
- Dermatological Science, 57, 162-169.: Anne Bernadette So KawDocument6 pagesDermatological Science, 57, 162-169.: Anne Bernadette So KawAnne KawNo ratings yet
- Kuliah LeukimiaDocument31 pagesKuliah LeukimiaMohammad SutamiNo ratings yet
- Labyrinth: BolanoDocument13 pagesLabyrinth: BolanojgswanNo ratings yet
- Special Senses NotesDocument17 pagesSpecial Senses NotesataraxialliNo ratings yet