You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5796)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Comparison of Total Body Irradiation Versus Non-Total Body Irradiation Containing Regimens For de Novo Acute Myeloid Leukemia in ChildrenDocument7 pagesComparison of Total Body Irradiation Versus Non-Total Body Irradiation Containing Regimens For de Novo Acute Myeloid Leukemia in ChildrenAbdurrahman HasanuddinNo ratings yet
- Magnetic Resonance Imaging Versus Serum Iron Status As Diagnostic Tools For Pituitary Iron Overload in Children With Beta ThalassemiaDocument13 pagesMagnetic Resonance Imaging Versus Serum Iron Status As Diagnostic Tools For Pituitary Iron Overload in Children With Beta ThalassemiaAbdurrahman HasanuddinNo ratings yet
- Mina Jahangiri, Fakher Rahim & Amal Saki Malehi: Scientific ReportsDocument13 pagesMina Jahangiri, Fakher Rahim & Amal Saki Malehi: Scientific ReportsAbdurrahman HasanuddinNo ratings yet
- Sponsored Supplement Publication ManuscriptDocument14 pagesSponsored Supplement Publication ManuscriptAbdurrahman HasanuddinNo ratings yet
- Childhood Iron Deficiency Anemia Leads To Recurrent Respiratory Tract Infections and GastroenteritisDocument8 pagesChildhood Iron Deficiency Anemia Leads To Recurrent Respiratory Tract Infections and GastroenteritisAbdurrahman HasanuddinNo ratings yet
- Therapy For Children and Adults With Mixed Phenotype Acute Leukemia: A Systematic Review and Meta-AnalysisDocument23 pagesTherapy For Children and Adults With Mixed Phenotype Acute Leukemia: A Systematic Review and Meta-AnalysisAbdurrahman HasanuddinNo ratings yet
- Gain of Chromosome 21 in Hematological Malignancies: Lessons From Studying Leukemia in Children With Down SyndromeDocument16 pagesGain of Chromosome 21 in Hematological Malignancies: Lessons From Studying Leukemia in Children With Down SyndromeAbdurrahman HasanuddinNo ratings yet
- Pregnancy and Child Health Outcomes in Pediatric and Young Adult Leukemia and Lymphoma Survivors: A Systematic ReviewDocument25 pagesPregnancy and Child Health Outcomes in Pediatric and Young Adult Leukemia and Lymphoma Survivors: A Systematic ReviewAbdurrahman HasanuddinNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Payaman KamiDocument35 pagesPayaman Kamifaye tamayoNo ratings yet
- Opposite Integers1Document2 pagesOpposite Integers1Hapsari C. Hanandya NannaNo ratings yet
- Department of Human Services: Course Information Course DescriptionDocument9 pagesDepartment of Human Services: Course Information Course DescriptionS ElburnNo ratings yet
- 71 SubmissionDocument4 pages71 Submissionmohamed aliNo ratings yet
- Activity 4.analytic RubricDocument2 pagesActivity 4.analytic RubricAbby PolvorizaNo ratings yet
- Implementation LabDocument7 pagesImplementation LabDavid BenjamingNo ratings yet
- Workshop Practical Attendance SheetDocument2 pagesWorkshop Practical Attendance SheetSachidhanandam MNo ratings yet
- Diode Equivalent ModelsDocument9 pagesDiode Equivalent ModelsJay Ey0% (1)
- MIT15 093J F09 Rec04Document4 pagesMIT15 093J F09 Rec04santiago gonzalezNo ratings yet
- Courses Offered in Spring 2015Document3 pagesCourses Offered in Spring 2015Mohammed Afzal AsifNo ratings yet
- Experiment 3: Illumination Design of Dental Clinic: B. Lighting StandardDocument16 pagesExperiment 3: Illumination Design of Dental Clinic: B. Lighting StandarderizaNo ratings yet
- Weekly Progress Report PDFDocument7 pagesWeekly Progress Report PDFHeak Hor50% (2)
- Chart-5050 by Songram BMA 54thDocument4 pagesChart-5050 by Songram BMA 54thMd. Noor HasanNo ratings yet
- CAE Listening Practice Test 13 Printable - EngExam - InfoDocument2 pagesCAE Listening Practice Test 13 Printable - EngExam - InfoCarolina MartinezNo ratings yet
- Watson SPEECH TO TEXT Code Snippet.rDocument2 pagesWatson SPEECH TO TEXT Code Snippet.rLucia Carlina Puzzar QuinteroNo ratings yet
- 32 KV High Voltage Power Transmission Line and Stress On Brassica JunceaDocument4 pages32 KV High Voltage Power Transmission Line and Stress On Brassica Junceamuhammad mushofahNo ratings yet
- Summary Buku Introduction To Management - John SchermerhornDocument5 pagesSummary Buku Introduction To Management - John SchermerhornElyana BiringNo ratings yet
- Asphaltene Eng2020Document4 pagesAsphaltene Eng2020Elprince MidoNo ratings yet
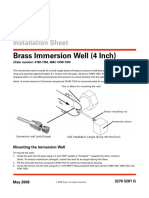
- Brass Immersion Well (4 Inch) : Installation SheetDocument2 pagesBrass Immersion Well (4 Inch) : Installation SheetKim Nicolas SaikiNo ratings yet
- Bahasa Inggris Teknik Individual Assignment 3Document5 pagesBahasa Inggris Teknik Individual Assignment 3Khaiza SyNo ratings yet
- Les Lac Inset Monitoring FormDocument57 pagesLes Lac Inset Monitoring FormKim Sang AhNo ratings yet
- Engineering Council of South Africa: Training and Mentoring Guide For Professional CategoriesDocument26 pagesEngineering Council of South Africa: Training and Mentoring Guide For Professional CategoriesMECHANICAL ENGINEERINGNo ratings yet
- Name: Maturan, Renz Myko B. Date: November 28, 2022 Subject & Section: EE 330 AC/DC Machineries - CDocument7 pagesName: Maturan, Renz Myko B. Date: November 28, 2022 Subject & Section: EE 330 AC/DC Machineries - CRenz MykoNo ratings yet
- Hot-Rolled Steel Beam Calculation To AISC 360-16Document2 pagesHot-Rolled Steel Beam Calculation To AISC 360-16vanda_686788867No ratings yet
- Automobile Engineering NotesDocument120 pagesAutomobile Engineering Notesakshay2992No ratings yet
- Fatigue BasicsDocument30 pagesFatigue BasicsABY.SAAJEDI879No ratings yet
- Final Examination SEMESTER 1, SESSION 2014/2015: SKAA 2722 1Document10 pagesFinal Examination SEMESTER 1, SESSION 2014/2015: SKAA 2722 1Hanis SyafiqNo ratings yet
- Ductile-Iron Pressure Pipe: Standard Index of Specifications ForDocument2 pagesDuctile-Iron Pressure Pipe: Standard Index of Specifications ForTamil funNo ratings yet
- History of Sport PsychologyDocument13 pagesHistory of Sport PsychologyObii DenisNo ratings yet
- Transportation Research Part C: Xiaojie Luan, Francesco Corman, Lingyun MengDocument27 pagesTransportation Research Part C: Xiaojie Luan, Francesco Corman, Lingyun MengImags GamiNo ratings yet