You might also like
- (19330693 - Journal of Neurosurgery) Anatomical Considerations of Fascial Release in Ulnar Nerve Transposition - A Concept RevisitedDocument7 pages(19330693 - Journal of Neurosurgery) Anatomical Considerations of Fascial Release in Ulnar Nerve Transposition - A Concept RevisitedDimitris RodriguezNo ratings yet
- Clinical Biomechanics: James Wickham, Tania Pizzari, Simon Balster, Charlotte Ganderton, Lyn WatsonDocument7 pagesClinical Biomechanics: James Wickham, Tania Pizzari, Simon Balster, Charlotte Ganderton, Lyn WatsonErick Andrade IbarraNo ratings yet
- Rectus Femoris in Gait CycleDocument5 pagesRectus Femoris in Gait CycleanjelikaNo ratings yet
- 2016 Sanchez Journal of EMG and KinesiologyDocument6 pages2016 Sanchez Journal of EMG and Kinesiologygembi9No ratings yet
- Antecipatory Postural AdjustmentsDocument9 pagesAntecipatory Postural AdjustmentsPedro FonsecaNo ratings yet
- Yong-Hyun 2011Document7 pagesYong-Hyun 2011GorkaBuesaNo ratings yet
- Stabilizing Function of The Long Head of The Biceps in The Hanging Arm PositionDocument8 pagesStabilizing Function of The Long Head of The Biceps in The Hanging Arm PositionMahatria RajNo ratings yet
- President's Address: Trick MovementsDocument3 pagesPresident's Address: Trick MovementsDr. Rushikesh K. Joshi100% (1)
- Changes in Lumbar Lordosis Modify The RoDocument4 pagesChanges in Lumbar Lordosis Modify The RoanjosNo ratings yet
- Morisaki 2021Document4 pagesMorisaki 2021Deborah SalinasNo ratings yet
- Human Movement Science: Brian C. Nairn, Janessa D.M. DrakeDocument11 pagesHuman Movement Science: Brian C. Nairn, Janessa D.M. DrakeQuiroprácticaParaTodosNo ratings yet
- Lumbar Multifidus Activation During Varied Speed, Incline WalkingDocument25 pagesLumbar Multifidus Activation During Varied Speed, Incline WalkingwalterNo ratings yet
- Sindesmosi Biomechanical Sequelae of Syndesmosis Injury and RepairDocument22 pagesSindesmosi Biomechanical Sequelae of Syndesmosis Injury and RepairTameemNo ratings yet
- 2016 Nerve Compression Syndromes at The ElbowDocument8 pages2016 Nerve Compression Syndromes at The ElbowAbraham Antonio Diaz TorresNo ratings yet
- Activation of The Human Diaphragm During A RepetitiveDocument11 pagesActivation of The Human Diaphragm During A RepetitiveIan ZhangNo ratings yet
- A.D. Pearle - Surgical Technique and Anatomic Study of Latissimus Dorsi and Teres Major Transfers (2006)Document9 pagesA.D. Pearle - Surgical Technique and Anatomic Study of Latissimus Dorsi and Teres Major Transfers (2006)João Pedro ZenattoNo ratings yet
- Experimental Flatfoot Model The Contribution of Dynamic LoadingDocument6 pagesExperimental Flatfoot Model The Contribution of Dynamic LoadingGeorge FernandoNo ratings yet
- Análisis de Elementos Finitos Del Comportamiento Biomecánico de Toda La Columna Toracolumbar Con Efecto Ligamentoso.Document16 pagesAnálisis de Elementos Finitos Del Comportamiento Biomecánico de Toda La Columna Toracolumbar Con Efecto Ligamentoso.Alejandro Marcelo Samalvides PachecoNo ratings yet
- 2009 - ProprioceptionDocument7 pages2009 - ProprioceptionMariana NannettiNo ratings yet
- Spatial Anisotropy Analyses of SubcutaneDocument10 pagesSpatial Anisotropy Analyses of SubcutaneCaerulea Accipiter StriatusNo ratings yet
- Pelvifemoral Rhythm During Unilateral Hip Flexion in StandingDocument5 pagesPelvifemoral Rhythm During Unilateral Hip Flexion in StandingWATEfakNo ratings yet
- Hamstring OM 21Document5 pagesHamstring OM 21Dr Ahmed NabilNo ratings yet
- Frog 2005Document11 pagesFrog 2005Alfi OktafaniNo ratings yet
- Journal of Electromyography and Kinesiology: Lucien Hackett, Darren Reed, Mark Halaki, Karen A. GinnDocument7 pagesJournal of Electromyography and Kinesiology: Lucien Hackett, Darren Reed, Mark Halaki, Karen A. GinnManuel Guillermo Martinez CifuentesNo ratings yet
- Pedro Pérez-Soriano, Salvador Llana Belloch - Biomecanica Basica Aplicada A La Actividad Fisica y El Deporte-Paidotribo (2015)Document7 pagesPedro Pérez-Soriano, Salvador Llana Belloch - Biomecanica Basica Aplicada A La Actividad Fisica y El Deporte-Paidotribo (2015)Osorio Miguel OsorioNo ratings yet
- Joint Position Sense and Vibration Sense: Anatomical Organisation and AssessmentDocument5 pagesJoint Position Sense and Vibration Sense: Anatomical Organisation and AssessmentKaho WongNo ratings yet
- The Myodural Bridge - A Review of The Literature and Clinical Implications 2014Document9 pagesThe Myodural Bridge - A Review of The Literature and Clinical Implications 2014lukeNo ratings yet
- The Examination and Recording of The Occlusion: Why and HowDocument10 pagesThe Examination and Recording of The Occlusion: Why and HowlvisageNo ratings yet
- Feline thyroarytenoid muscle contractile propertiesDocument7 pagesFeline thyroarytenoid muscle contractile propertiesChrisNo ratings yet
- Flexortendonrepair: Healing, Biomechanics, and Suture ConfigurationsDocument8 pagesFlexortendonrepair: Healing, Biomechanics, and Suture ConfigurationsyellowbieNo ratings yet
- Contraccion TrunkDocument5 pagesContraccion TrunkSaira Camila Osso SanchezNo ratings yet
- Biomechanical Factors in Rotator Cuff PathologyDocument5 pagesBiomechanical Factors in Rotator Cuff PathologyYa ChenNo ratings yet
- Tendon Transfer For Radial Nerve Palsy: Michael E. Rettig, MD, and Keith B. Raskin, MDDocument12 pagesTendon Transfer For Radial Nerve Palsy: Michael E. Rettig, MD, and Keith B. Raskin, MDFernando Martín Arce AlvaNo ratings yet
- Superficial Lumbopelvic Muscle OveractivDocument7 pagesSuperficial Lumbopelvic Muscle OveractivHugroNo ratings yet
- Cervical and Lumbar Vertebra RelationshipDocument3 pagesCervical and Lumbar Vertebra RelationshipEdgardo Bivimas100% (1)
- Xxxxissue 06 09 Iliolumbar LigamentsDocument3 pagesXxxxissue 06 09 Iliolumbar Ligamentsrehabimina1No ratings yet
- TVR and Vibration-Induced Timing of Motor Impulses in The Human Jaw Elevator MusclesDocument10 pagesTVR and Vibration-Induced Timing of Motor Impulses in The Human Jaw Elevator MusclesWilliam Alexander Bejarano PinillaNo ratings yet
- Review Literatur Keefektifan Mobilisasi Dini Pada Post Operasi Perbaikan Tendon FleksorDocument7 pagesReview Literatur Keefektifan Mobilisasi Dini Pada Post Operasi Perbaikan Tendon FleksorKrinta AlisaNo ratings yet
- Scapular Dyskinesia RehabDocument6 pagesScapular Dyskinesia RehabQuiroprácticaParaTodosNo ratings yet
- Mandibular Rest Position and ElectricalDocument6 pagesMandibular Rest Position and ElectricalPaula GuerreroNo ratings yet
- Deep_Tendon_Reflexes_The_What_Why_Where_and_How_ofDocument11 pagesDeep_Tendon_Reflexes_The_What_Why_Where_and_How_ofAndrej a TarkoNo ratings yet
- Tendon Transfers For Thumb Opposition: Alexander Y. Shin, MD, and Khiem D. Dao, MDDocument17 pagesTendon Transfers For Thumb Opposition: Alexander Y. Shin, MD, and Khiem D. Dao, MDFernando Martín Arce AlvaNo ratings yet
- Infleunce of Group Function Canine Guidance On Elevator MuscleDocument8 pagesInfleunce of Group Function Canine Guidance On Elevator MuscleHossam BarghashNo ratings yet
- Basic Biomechanics of The HipDocument8 pagesBasic Biomechanics of The HipManuel Azael Rodríguez CigalaNo ratings yet
- Anatomy of The Knee Joint Lateral RetinaculumDocument6 pagesAnatomy of The Knee Joint Lateral RetinaculumHenrique TapumNo ratings yet
- Finkelstein's Test - A Biomechanical AnalysisDocument6 pagesFinkelstein's Test - A Biomechanical AnalysisLUIS SALVADOR FLORESNo ratings yet
- Rehabilitation of Elbow Trauma: Shrikant J. Chinchalkar, Bscot, Otr, CHT, Mike Szekeres, BscotDocument12 pagesRehabilitation of Elbow Trauma: Shrikant J. Chinchalkar, Bscot, Otr, CHT, Mike Szekeres, BscotIoanaCamiiNo ratings yet
- Rotadores de CaderaDocument12 pagesRotadores de CaderaMicaela BenavidesNo ratings yet
- Falla 2004Document7 pagesFalla 2004Martín Seijas GonzálezNo ratings yet
- Infant Oli No 2012Document7 pagesInfant Oli No 2012HeculesNo ratings yet
- Chapter 26: Digital Deformities and SurgeryDocument20 pagesChapter 26: Digital Deformities and SurgerypoddataNo ratings yet
- Posterolateral Corner Injuries of The KneeDocument9 pagesPosterolateral Corner Injuries of The KneeIntanNo ratings yet
- Spinal and Epidural Anesthesia: John H. Turnbull and Pedram AleshiDocument21 pagesSpinal and Epidural Anesthesia: John H. Turnbull and Pedram AleshiAlex Orellana CortezNo ratings yet
- Interphalangeal Joint (Hand Complex)Document6 pagesInterphalangeal Joint (Hand Complex)VIRESH VNo ratings yet
- Spinal and Supraspinal Effects of Activity in Ligament AfferentsDocument10 pagesSpinal and Supraspinal Effects of Activity in Ligament AfferentsItai IzhakNo ratings yet
- General Principles of Tendon TransfersDocument12 pagesGeneral Principles of Tendon TransfersHari PrasadNo ratings yet
- New Insight Into The Iliofemoral Ligament Based On The Anatomical Study of The Hip Joint CapsuleDocument8 pagesNew Insight Into The Iliofemoral Ligament Based On The Anatomical Study of The Hip Joint Capsulexekar59382No ratings yet
- Jurnal 3Document27 pagesJurnal 3Anisa FirdausNo ratings yet
- Mandibular MovementsDocument140 pagesMandibular MovementsVishal Reddy100% (1)
- Neurobiology and BehaviorFrom EverandNeurobiology and BehaviorA. O. Dennis WillowsRating: 5 out of 5 stars5/5 (1)
- Biomechanical Differences Between Left - and Righthanded Baseball PitchersDocument10 pagesBiomechanical Differences Between Left - and Righthanded Baseball PitchersYoh ChenNo ratings yet
- Comparison of Change of Direction SpeedDocument15 pagesComparison of Change of Direction SpeedYoh ChenNo ratings yet
- An Applied Research Model For TheDocument11 pagesAn Applied Research Model For TheYoh ChenNo ratings yet
- Back MusclesDocument10 pagesBack MusclesThe Fitness CoachNo ratings yet
- An Equation To Calculate Individual Muscle ContributionsDocument8 pagesAn Equation To Calculate Individual Muscle ContributionsYoh ChenNo ratings yet
- An MRI Investigation Into The Function of TheDocument4 pagesAn MRI Investigation Into The Function of TheYoh ChenNo ratings yet
- Reliability of Ultrasound Imaging Measures of TransverseDocument8 pagesReliability of Ultrasound Imaging Measures of TransverseYoh ChenNo ratings yet
- Influence of Inward Pressure of TheDocument4 pagesInfluence of Inward Pressure of TheYoh ChenNo ratings yet
- The Relationship Between Trunk Muscle ThicknessDocument7 pagesThe Relationship Between Trunk Muscle ThicknessYoh ChenNo ratings yet
- Injury Trends in Major League BaseballDocument9 pagesInjury Trends in Major League BaseballYoh ChenNo ratings yet
- Taghipour Et Al-2019-Journal of Ultrasound in MedicineDocument13 pagesTaghipour Et Al-2019-Journal of Ultrasound in MedicineYoh ChenNo ratings yet
- Prediction and Validation of Total and Regional SkeletalDocument8 pagesPrediction and Validation of Total and Regional SkeletalYoh ChenNo ratings yet
- Lumbar Spine Buckling Under Compression Studied in CadaversDocument6 pagesLumbar Spine Buckling Under Compression Studied in CadaversYoh ChenNo ratings yet
- Sport-Specific Assessment of TheDocument27 pagesSport-Specific Assessment of TheYoh ChenNo ratings yet
- Interrater and Intrarater ReliabilityDocument10 pagesInterrater and Intrarater ReliabilityYoh ChenNo ratings yet
- Intra - and Inter-Rater Reliabilities For Novel Muscle ThicknessDocument6 pagesIntra - and Inter-Rater Reliabilities For Novel Muscle ThicknessYoh ChenNo ratings yet
- Functional Rehabilitation of Low Back Pain With Core StabilizatioDocument47 pagesFunctional Rehabilitation of Low Back Pain With Core StabilizatioEnyaw DroffatsNo ratings yet
- Critical Review of The Impact of Core Stability On UpperDocument9 pagesCritical Review of The Impact of Core Stability On UpperCambriaChicoNo ratings yet
- Gluteus Medius and Scapula Muscle ActivationsDocument6 pagesGluteus Medius and Scapula Muscle ActivationsYoh ChenNo ratings yet
- Effects of An 8-Week Body-WeightDocument10 pagesEffects of An 8-Week Body-WeightYoh ChenNo ratings yet
- Effects of Stabilization Exercise Using Flexi-Bar OnDocument5 pagesEffects of Stabilization Exercise Using Flexi-Bar OnYoh ChenNo ratings yet
- Dynamic Stretching Has Sustained Effects On Range of Motion and Passive Stiffness of The Hamstring MusclesDocument8 pagesDynamic Stretching Has Sustained Effects On Range of Motion and Passive Stiffness of The Hamstring Musclesjul yanNo ratings yet
- Role of Calcium in Muscle ContractionDocument12 pagesRole of Calcium in Muscle Contractionlisa mornoNo ratings yet
- CFES PTRM SamplePgsDocument70 pagesCFES PTRM SamplePgsIvo LeiteNo ratings yet
- CIE IGCSE Biology Respiration Question Paper 2Document13 pagesCIE IGCSE Biology Respiration Question Paper 2Annmary AbrahamNo ratings yet
- BS Allied Health 1st Sem 27jan22Document43 pagesBS Allied Health 1st Sem 27jan22Gulab khanNo ratings yet
- Competitive Tennis For Young PlayersDocument146 pagesCompetitive Tennis For Young PlayersTuzos100% (1)
- TQ TemplateDocument5 pagesTQ TemplateFerdinand SalardaNo ratings yet
- Green Petal BroucherDocument4 pagesGreen Petal BroucherSunil SagarNo ratings yet
- Muscle MCQs - AnswerDocument41 pagesMuscle MCQs - AnswerMohit Balboa90% (79)
- HOPE NotesDocument6 pagesHOPE Notesayaka kamisatoNo ratings yet
- Anatomi KinesiologiDocument31 pagesAnatomi KinesiologivitriaNo ratings yet
- Brenda R. Bigland-Ritchie - FatigueDocument540 pagesBrenda R. Bigland-Ritchie - FatigueRukaphuongNo ratings yet
- Muscular System - Lesson 19Document17 pagesMuscular System - Lesson 19Gamer0092No ratings yet
- CIT Colleges of Paniqui FoundationDocument3 pagesCIT Colleges of Paniqui FoundationKeseya Castillo TorresNo ratings yet
- Quarter 3 - Week No. 2 Information Sheet: Baybay City Senior High SchoolDocument6 pagesQuarter 3 - Week No. 2 Information Sheet: Baybay City Senior High Schoolangelica palomaNo ratings yet
- Physiology05 Muscle CellDocument37 pagesPhysiology05 Muscle CellsmpoojasubashNo ratings yet
- Literature Review SkeletonDocument7 pagesLiterature Review Skeletonewhknurif100% (1)
- EMG Signal ProcessingDocument38 pagesEMG Signal ProcessingAbdi TeferiNo ratings yet
- Animal Tissues Cell Types and Modifications CompleteDocument60 pagesAnimal Tissues Cell Types and Modifications Completealphabet swswNo ratings yet
- Physiology of Theraupetic Exercise: By: Nini Natalia, DRDocument53 pagesPhysiology of Theraupetic Exercise: By: Nini Natalia, DRSaktriawan ArifNo ratings yet
- Anaphy Muscular SystemDocument54 pagesAnaphy Muscular SystemZosia SageNo ratings yet
- Personal Exercise Plan Gcse CourseworkDocument4 pagesPersonal Exercise Plan Gcse Courseworkafjwrmcuokgtej100% (2)
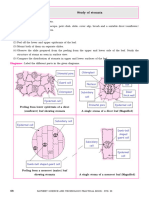
- Experiment 9: Study of StomataDocument10 pagesExperiment 9: Study of StomatajasmitaadodhiaNo ratings yet
- Chap-20 - Locomotion & MovementDocument52 pagesChap-20 - Locomotion & MovementMittal SavaniNo ratings yet
- Guyton and Hall Textbook of Medical PhysDocument13 pagesGuyton and Hall Textbook of Medical PhysPatrick Paul Malano0% (1)
- PE To 16Document193 pagesPE To 16Danielle CunninghamNo ratings yet
- (Lecture 8) Muscles, Bone, and SkinDocument23 pages(Lecture 8) Muscles, Bone, and SkinKasraSrNo ratings yet
- Fitness benefits of daily activitiesDocument10 pagesFitness benefits of daily activitiesAbhijeet ParateNo ratings yet
- The Benefits of PilatesDocument4 pagesThe Benefits of PilatesJen LeeNo ratings yet
- 0413 Physical Education: MARK SCHEME For The October/November 2012 SeriesDocument9 pages0413 Physical Education: MARK SCHEME For The October/November 2012 SeriesRavi BhollahNo ratings yet
- P.E 101 Physical Fitness and HealthDocument55 pagesP.E 101 Physical Fitness and HealthElaiza Mae Andalan100% (1)