You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
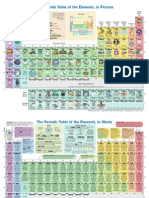
- The Periodic Table of Elements, in PicturesDocument2 pagesThe Periodic Table of Elements, in Picturesrustyy88100% (1)
- Rcads-Child TemplateDocument3 pagesRcads-Child TemplateHome Sweet100% (1)
- ROA Salmonella-Enteritidis-ST11 2022 FinalDocument19 pagesROA Salmonella-Enteritidis-ST11 2022 FinalFrancisca BallesterosNo ratings yet
- 3interim Advice For Public Health Authorities On Summer Events MPXDocument6 pages3interim Advice For Public Health Authorities On Summer Events MPXFrancisca BallesterosNo ratings yet
- Joint ECDC WHO Interim Advice On RCCE For Monkeypox 2 June 2022Document7 pagesJoint ECDC WHO Interim Advice On RCCE For Monkeypox 2 June 2022Francisca BallesterosNo ratings yet
- 5communicable Disease Threats Report 30 Jul 2022 PublicDocument28 pages5communicable Disease Threats Report 30 Jul 2022 PublicFrancisca BallesterosNo ratings yet
- 1considerations For Contact Tracing MPX June 2022Document13 pages1considerations For Contact Tracing MPX June 2022Francisca BallesterosNo ratings yet
- Variable Dictionary VaccineTracker-04!11!2021Document3 pagesVariable Dictionary VaccineTracker-04!11!2021Francisca BallesterosNo ratings yet
- COVID 19 Considerations For Booster Doses in Adolescents Feb 2022Document14 pagesCOVID 19 Considerations For Booster Doses in Adolescents Feb 2022Francisca BallesterosNo ratings yet
- COVID 19 in Children and The Role of School Settings in Transmission Second UpdateDocument37 pagesCOVID 19 in Children and The Role of School Settings in Transmission Second UpdateFrancisca BallesterosNo ratings yet
- 2ECDC WHO Risk Communication Community Engagement Monkeypox Outbreak EuropeDocument11 pages2ECDC WHO Risk Communication Community Engagement Monkeypox Outbreak EuropeFrancisca BallesterosNo ratings yet
- Description and Disclaimer Daily ReportingDocument1 pageDescription and Disclaimer Daily ReportingFrancisca BallesterosNo ratings yet
- Variable Dictionary VaccineTracker-20-08-2021Document3 pagesVariable Dictionary VaccineTracker-20-08-2021Francisca BallesterosNo ratings yet
- Interim Public Health Considerations For COVID 19 Vaccination of AdolescentsDocument19 pagesInterim Public Health Considerations For COVID 19 Vaccination of AdolescentsFrancisca BallesterosNo ratings yet
- Agenda EAAD - European-Level Launch EventDocument1 pageAgenda EAAD - European-Level Launch EventFrancisca BallesterosNo ratings yet
- 2021-01-13 Variable Dictionary and Disclaimer National Weekly DataDocument1 page2021-01-13 Variable Dictionary and Disclaimer National Weekly DataFrancisca BallesterosNo ratings yet
- Communicable Disease Threats Report 16 Jun 2018Document11 pagesCommunicable Disease Threats Report 16 Jun 2018Francisca BallesterosNo ratings yet
- Communicable Disease Threats Report 26 Aug 2017Document9 pagesCommunicable Disease Threats Report 26 Aug 2017Francisca BallesterosNo ratings yet
- ECDC - Systematic Review On Hepatitis B and C Prevalence in The EU-EEADocument1 pageECDC - Systematic Review On Hepatitis B and C Prevalence in The EU-EEAFrancisca BallesterosNo ratings yet
- Hiv and Aids: Surveillance ReportDocument7 pagesHiv and Aids: Surveillance ReportFrancisca BallesterosNo ratings yet
- Ecdc Infographics2015 Measles Is SeriousDocument1 pageEcdc Infographics2015 Measles Is SeriousFrancisca BallesterosNo ratings yet
- Zika Virus Safety of Substances of Human Origin Update 2017 WebDocument35 pagesZika Virus Safety of Substances of Human Origin Update 2017 WebFrancisca BallesterosNo ratings yet
- Antimicrobial Resistance Europe 2015Document120 pagesAntimicrobial Resistance Europe 2015Francisca BallesterosNo ratings yet
- ECDC - Public Consultation - Expert Opinion On Rotavirus Vaccination in InfancyDocument1 pageECDC - Public Consultation - Expert Opinion On Rotavirus Vaccination in InfancyFrancisca BallesterosNo ratings yet
- Communicable Disease Threats Report 29 Jul 2017Document13 pagesCommunicable Disease Threats Report 29 Jul 2017Francisca BallesterosNo ratings yet
- Who Ccsivd Meetingreport SangreDocument31 pagesWho Ccsivd Meetingreport SangreFrancisca BallesterosNo ratings yet
- ECDC Epidemiological SituationDocument1 pageECDC Epidemiological SituationFrancisca BallesterosNo ratings yet
- ECDC - ECDC Policy Briefing - Preparing For Zika in The EUDocument1 pageECDC - ECDC Policy Briefing - Preparing For Zika in The EUFrancisca BallesterosNo ratings yet
- ECDC Policy BriefingsDocument1 pageECDC Policy BriefingsFrancisca BallesterosNo ratings yet
- ECDC - Examples of Interventions To Manage Tuberculosis in Vulnerable GroupsDocument2 pagesECDC - Examples of Interventions To Manage Tuberculosis in Vulnerable GroupsFrancisca BallesterosNo ratings yet
- Analisis Sifat Mirip Obat Prediksi ADMET Dan PenamDocument14 pagesAnalisis Sifat Mirip Obat Prediksi ADMET Dan PenamFrisma DheanovaNo ratings yet
- ER Diagram ExerciseDocument2 pagesER Diagram ExerciseFarhana NaziraNo ratings yet
- Apostila 04Document112 pagesApostila 04fazziobeatrizNo ratings yet
- English 7 Q2 Module 1 1Document15 pagesEnglish 7 Q2 Module 1 1Jojam CarpioNo ratings yet
- NSTP Program GuideDocument19 pagesNSTP Program GuideLester ElipseNo ratings yet
- Safe carriage of dangerous goods by airDocument2 pagesSafe carriage of dangerous goods by airNuran Dursunoğlu100% (1)
- Schemes of Government of Rajasthan in HealthDocument67 pagesSchemes of Government of Rajasthan in HealthKamal ShuklaNo ratings yet
- The Boston Globe - Vol. 304 No. 011 (11 Jul 2023)Document32 pagesThe Boston Globe - Vol. 304 No. 011 (11 Jul 2023)mariuscsmNo ratings yet
- Triethanolamine Safety ReportDocument6 pagesTriethanolamine Safety ReportMaria Inês HarrisNo ratings yet
- Menhaden Fish Oil Typical AnalysisDocument1 pageMenhaden Fish Oil Typical Analysismelimaulani-1No ratings yet
- Alcapa SyndromeDocument38 pagesAlcapa SyndromeZiaNo ratings yet
- General Topics: Anesthesia, Analgesia, and Sedation of Small MammalsDocument23 pagesGeneral Topics: Anesthesia, Analgesia, and Sedation of Small Mammalsdoja catNo ratings yet
- Lauren Makosky ResumeDocument2 pagesLauren Makosky Resumeapi-634419348No ratings yet
- Worksheet For Respiration Low AnswersDocument2 pagesWorksheet For Respiration Low AnswersIcs 2022No ratings yet
- Benefits of Locust PoseDocument2 pagesBenefits of Locust PoseMIBNo ratings yet
- Palm Fatty Acid MSDSDocument2 pagesPalm Fatty Acid MSDSAnggun100% (1)
- Course Guide in Trends and Issues in Social StudiesDocument7 pagesCourse Guide in Trends and Issues in Social StudiesRomar M. DavidNo ratings yet
- Cawood - Howell 1988Document5 pagesCawood - Howell 1988dra.claudiamaria.tiNo ratings yet
- Revised - Ie18 Final UpdatedDocument120 pagesRevised - Ie18 Final UpdatedLUCAS AndrewsNo ratings yet
- Đề 1Document16 pagesĐề 1Tri DangNo ratings yet
- RSPH Level 4 Award in Haccp Management For Food ManufacturingDocument19 pagesRSPH Level 4 Award in Haccp Management For Food ManufacturingHema HemaNo ratings yet
- E.Coli Essay FINAL PDFDocument8 pagesE.Coli Essay FINAL PDFSaraturituriNo ratings yet
- Ashgate - Landscape Professional Practice PDFDocument281 pagesAshgate - Landscape Professional Practice PDFyondaimethunderNo ratings yet
- Intrusion Detection System Method StatementDocument30 pagesIntrusion Detection System Method StatementNideesh RobertNo ratings yet
- Long-Term Mortality After The Blood Pressure and Lipid-Lowering Treatment in Hypertensive Patients: 16-Year Follow-Up of The ASCOT Legacy StudyDocument22 pagesLong-Term Mortality After The Blood Pressure and Lipid-Lowering Treatment in Hypertensive Patients: 16-Year Follow-Up of The ASCOT Legacy StudyFlore HountondjiNo ratings yet
- If Men Could MenstruateDocument3 pagesIf Men Could Menstruatepigixih621No ratings yet
- CLASSIC ARTICLE-Evaluation of The Factors Necessary To Develop Stability in Mandibular Dentures-Corwin R. WrightDocument10 pagesCLASSIC ARTICLE-Evaluation of The Factors Necessary To Develop Stability in Mandibular Dentures-Corwin R. WrightChander UdheyNo ratings yet
- D&D 5E - Homebrew - Class ProfligateDocument7 pagesD&D 5E - Homebrew - Class Profligate19931214No ratings yet
- )Document6 pages)nuraninarunNo ratings yet