You might also like
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5813)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (844)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Weightlifting 101 - OP3 (January 2020)Document140 pagesWeightlifting 101 - OP3 (January 2020)Yusuf DuranNo ratings yet
- Converge&Diverge Lab ReportDocument28 pagesConverge&Diverge Lab ReportIrfan Syafiq40% (5)
- Soil-Structure Interaction Analysis For Bridge Caisson FoundationDocument10 pagesSoil-Structure Interaction Analysis For Bridge Caisson FoundationarslanpasaNo ratings yet
- SecantPile Method StatementDocument34 pagesSecantPile Method Statementsantanu mukherjeeNo ratings yet
- Method Statement For Production and Laying of Cement Concrete Kerb and Kerb With ChannelDocument5 pagesMethod Statement For Production and Laying of Cement Concrete Kerb and Kerb With ChannelKeerti Bongu100% (1)
- Intech Open COVID-19Document20 pagesIntech Open COVID-19СергейNo ratings yet
- Primary and Secondary Negative Symptoms in SchizopDocument12 pagesPrimary and Secondary Negative Symptoms in SchizopСергейNo ratings yet
- Medicina: Electroconvulsive Therapy (ECT) in Bipolar Disorder Patients With Ultra-Rapid Cycling and Unstable Mixed StatesDocument17 pagesMedicina: Electroconvulsive Therapy (ECT) in Bipolar Disorder Patients With Ultra-Rapid Cycling and Unstable Mixed StatesСергейNo ratings yet
- Stress and Anxiety Among Healthcare Workers Associated With Covid-19 Pandemic in RussiaDocument8 pagesStress and Anxiety Among Healthcare Workers Associated With Covid-19 Pandemic in RussiaСергейNo ratings yet
- R. R. Gupta - Topics in Heterocyclic Chemistry: Microwave-Assisted Synthesis of HeterocyclesDocument14 pagesR. R. Gupta - Topics in Heterocyclic Chemistry: Microwave-Assisted Synthesis of HeterocyclesNstm30% (1)
- FAO: Classification and Illustrated Definition of Fishing GearsDocument110 pagesFAO: Classification and Illustrated Definition of Fishing GearsSapriyun SNo ratings yet
- CaveDocument6 pagesCaveKatrina MangaringNo ratings yet
- TOEFL Vocabulary 400 WordsDocument3 pagesTOEFL Vocabulary 400 WordsANGLISHT0% (1)
- Sew AbilityDocument1 pageSew AbilityAnonymous zd5HPB5No ratings yet
- Proceedings TIL2014Document204 pagesProceedings TIL2014GogyNo ratings yet
- Chapter 5 Perception Ans SensationDocument4 pagesChapter 5 Perception Ans SensationPing Ping TanNo ratings yet
- Literature Review Food SafetyDocument8 pagesLiterature Review Food Safetygw10ka6s100% (1)
- Case 11F Einschmecker SauceDocument2 pagesCase 11F Einschmecker SauceDexter LiboonNo ratings yet
- Product Life Cycle of Tata SaltDocument14 pagesProduct Life Cycle of Tata SaltHARIPRANESH KNo ratings yet
- Alg 2 t4 4Document13 pagesAlg 2 t4 4api-261379705No ratings yet
- I Am Proud To Be A FilipinoDocument1 pageI Am Proud To Be A Filipinojaner48No ratings yet
- Unit 11 Boyle Charles GayLussac and Combined Gas Law Worksheet Gas WS 1 2010Document2 pagesUnit 11 Boyle Charles GayLussac and Combined Gas Law Worksheet Gas WS 1 2010Pablo AlconzNo ratings yet
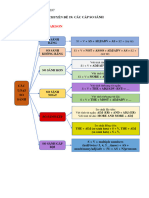
- CHUYÊN ĐỀ 19 - CÁC CẤP SO SÁNH - GRade B1,b2Document10 pagesCHUYÊN ĐỀ 19 - CÁC CẤP SO SÁNH - GRade B1,b2Thành Nam NguyễnNo ratings yet
- Dus 20 PlusDocument23 pagesDus 20 PlusMarly SalasNo ratings yet
- SSRN Id4542751Document28 pagesSSRN Id4542751Akbarjie_87No ratings yet
- Golden Gate Colleges P. Prieto ST., Batangas City: College of NursingDocument7 pagesGolden Gate Colleges P. Prieto ST., Batangas City: College of NursingR Hornilla ArcegaNo ratings yet
- Ate QuizDocument1 pageAte QuizRicardo VelozNo ratings yet
- 137Document1 page137IT jasmerNo ratings yet
- Vibhor Bishwas 27Document44 pagesVibhor Bishwas 27vibhors751No ratings yet
- Koso Xr-Sa Installation ManualDocument3 pagesKoso Xr-Sa Installation ManualPanagiotis Stam100% (2)
- UBoat Leader 2 Help SheetDocument2 pagesUBoat Leader 2 Help SheetChris van MelsNo ratings yet
- Investigatory ProjectsDocument1 pageInvestigatory ProjectsOwner PcNo ratings yet
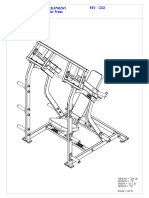
- HAMMER STRENGTH EQUIPMENT ILSP Iso Lateral Shoulder ...Document8 pagesHAMMER STRENGTH EQUIPMENT ILSP Iso Lateral Shoulder ...Rida DahmounNo ratings yet
- Psychophysiological Methods: Paul Sowden and Paul BarrettDocument42 pagesPsychophysiological Methods: Paul Sowden and Paul BarrettsudhaduraiasshNo ratings yet