You might also like
- Master File 2003 - Body As A WholeDocument32 pagesMaster File 2003 - Body As A Wholeobinna12No ratings yet
- MNI SAH ProtocolDocument10 pagesMNI SAH ProtocolAbo ZakariaNo ratings yet
- Vascular Emergencies: Susan L. Drinkwater, Vikas A. Pandey, and Alun H. DaviesDocument17 pagesVascular Emergencies: Susan L. Drinkwater, Vikas A. Pandey, and Alun H. DaviesHarshpreet KaurNo ratings yet
- Anaesthesia For TURPDocument6 pagesAnaesthesia For TURPMutia FarinaNo ratings yet
- Caring For A Patient After Coronary Artery Bypass.6Document6 pagesCaring For A Patient After Coronary Artery Bypass.6Nadia BeadleNo ratings yet
- Post Op CardiacDocument7 pagesPost Op CardiacsimplyputmonicNo ratings yet
- Coronary Artery Bypass Graft SurgeryDocument8 pagesCoronary Artery Bypass Graft SurgeryJatin SinghNo ratings yet
- Cardiac AnesthesiologyDocument48 pagesCardiac AnesthesiologyNiaNo ratings yet
- Cabg NursingDocument7 pagesCabg NursingDennis Cobb100% (1)
- TIVA in CKDDocument7 pagesTIVA in CKDfixheartNo ratings yet
- Anestesi Abdominal ApproachDocument14 pagesAnestesi Abdominal ApproachabdulkadirmunsyNo ratings yet
- Simon Bricker Short Answer QuestionsDocument280 pagesSimon Bricker Short Answer Questionskaran270100% (4)
- PE HeartofenglandDocument9 pagesPE HeartofenglandavfNo ratings yet
- Cardiology: 27 Maret 2021Document52 pagesCardiology: 27 Maret 2021Dian ParamitaNo ratings yet
- 296 Neck of Femur Fracture Peri-Operative ManagementDocument8 pages296 Neck of Femur Fracture Peri-Operative ManagementNilam dwinilamsariNo ratings yet
- The Preoperative EvaluationDocument25 pagesThe Preoperative Evaluationnormie littlemonsterNo ratings yet
- Saq 1Document68 pagesSaq 1joe kayongoNo ratings yet
- Perioperative Management of Pulmonary Hypertensive Crisis: AsktheexpertDocument2 pagesPerioperative Management of Pulmonary Hypertensive Crisis: AsktheexpertGede AdiNo ratings yet
- Trauma Tumpul AbdomenDocument30 pagesTrauma Tumpul AbdomendewiswahyuNo ratings yet
- Cardiac Surgery Basic KnowledgeDocument28 pagesCardiac Surgery Basic KnowledgeGinwong100% (1)
- Cardiac Anesthesia Made Ridiculously SimpleDocument17 pagesCardiac Anesthesia Made Ridiculously SimplecoolzygoteNo ratings yet
- Aneurysm Abdominal AortaDocument8 pagesAneurysm Abdominal AortaMochammad Halim NNo ratings yet
- 1 s2.0 S0870255121005096 MainDocument3 pages1 s2.0 S0870255121005096 MainangelemanuelarmasNo ratings yet
- 2018 Article 1648Document5 pages2018 Article 1648Dewi NurfadilahNo ratings yet
- RANASINGHE Cardiac Function & Disease & AnesthesiaDocument51 pagesRANASINGHE Cardiac Function & Disease & AnesthesiaDagimNo ratings yet
- Cardiac Coarctation of The Aorta CoA Management Following Surgical RepairDocument6 pagesCardiac Coarctation of The Aorta CoA Management Following Surgical RepairMohammed IbrahimNo ratings yet
- Cardiac CatheterizationDocument9 pagesCardiac CatheterizationAnurag Gupta100% (1)
- Care of The Unconscious, Multi-Trauma PatientDocument37 pagesCare of The Unconscious, Multi-Trauma PatientRomaine BarrettNo ratings yet
- AF KardiomiopatiDocument5 pagesAF KardiomiopatiannisNo ratings yet
- Perioperative Nursing Med-SurgDocument3 pagesPerioperative Nursing Med-SurgKarla Fralala100% (1)
- CC-Concept Map 2Document5 pagesCC-Concept Map 2MDCITY50% (2)
- Case StudyDocument6 pagesCase StudyHelsa Eldatarina JNo ratings yet
- ESC GUIDELINES SUMMARY on heart failure, atrial fibrillation, dyslipidaemia and cardiovascular preventionDocument11 pagesESC GUIDELINES SUMMARY on heart failure, atrial fibrillation, dyslipidaemia and cardiovascular preventionNick StamatiadisNo ratings yet
- Anaesthesia Guidelines for Patients with Marfan SyndromeDocument21 pagesAnaesthesia Guidelines for Patients with Marfan SyndromeZoelNo ratings yet
- Perioperative Care For CABG PatientsDocument32 pagesPerioperative Care For CABG PatientsAya EyadNo ratings yet
- Presentation By: DR Prabhakar Moderator: DR DeepakDocument44 pagesPresentation By: DR Prabhakar Moderator: DR DeepakPrabhakar KumarNo ratings yet
- Marfan ENDocument8 pagesMarfan ENDewinsNo ratings yet
- Medical Emergency Oral Q.docx26.docx8Document44 pagesMedical Emergency Oral Q.docx26.docx8Simina ÎntunericNo ratings yet
- Anaesthesia for Tetralogy of FallotDocument11 pagesAnaesthesia for Tetralogy of FallotIma SoniaNo ratings yet
- Treatment, Prognosis, and Follow-Up of Acute Pulmonary Embolism in Adults - UpToDateDocument49 pagesTreatment, Prognosis, and Follow-Up of Acute Pulmonary Embolism in Adults - UpToDateJulio Orallo MartínezNo ratings yet
- "Pulmonary Hypertension": Jimmy Ford, MD Pulmonary and Critical CareDocument51 pages"Pulmonary Hypertension": Jimmy Ford, MD Pulmonary and Critical CareSohil ElfarNo ratings yet
- Strategies For Improving Visualization During Endoscopic Skull Base SurgeryDocument10 pagesStrategies For Improving Visualization During Endoscopic Skull Base SurgeryTi FaNo ratings yet
- Poster Presentation CCRA Malang 2014Document3 pagesPoster Presentation CCRA Malang 2014alfarobi yogiNo ratings yet
- Eisenmenger SyndromeDocument10 pagesEisenmenger SyndromeprastiaNo ratings yet
- Review Article Ref: Anesthesiology Clinics September 2015 Dr. Anuradha T Jubilee Mission Medical College & Research Institute, Thrissur, Kerala, IndiaDocument40 pagesReview Article Ref: Anesthesiology Clinics September 2015 Dr. Anuradha T Jubilee Mission Medical College & Research Institute, Thrissur, Kerala, IndiaRun HajNo ratings yet
- Pulmonary EmbolismDocument46 pagesPulmonary EmbolismAnusha VergheseNo ratings yet
- Abdominal Aortic Aneurysms-EditDocument32 pagesAbdominal Aortic Aneurysms-EditrandikaNo ratings yet
- Acute Lung Edema Management PracticeDocument5 pagesAcute Lung Edema Management PracticeYunia DuanaNo ratings yet
- Politrauma - Rolul AtiDocument18 pagesPolitrauma - Rolul AtiChirita ElenaNo ratings yet
- Improving outcomes for high-risk patients with optimised anaesthesiaDocument46 pagesImproving outcomes for high-risk patients with optimised anaesthesiakevandmwnNo ratings yet
- Summary 2013 Esc GuidelinesDocument8 pagesSummary 2013 Esc GuidelinesNick StamatiadisNo ratings yet
- Aas - Hasta IqDocument8 pagesAas - Hasta IqFrancisco A. Perez JimenezNo ratings yet
- Open Heart 1Document18 pagesOpen Heart 1mohamedNo ratings yet
- HarrisDocument25 pagesHarrisHafiz AlfarizieNo ratings yet
- Preoperative Patient Assessment and Management: Roxanne Jeen L. FornollesDocument61 pagesPreoperative Patient Assessment and Management: Roxanne Jeen L. FornollesRyan FornollesNo ratings yet
- Preoperative Assessment and Premedication - PACUDocument60 pagesPreoperative Assessment and Premedication - PACUTraceNo ratings yet
- December 2012 Final Frca Soe Questions: Long CasesDocument23 pagesDecember 2012 Final Frca Soe Questions: Long Caseskaran270100% (1)
- PGSUP - 9198 - D.M. CARDIAC ANAESTHESIA - CANTP3 ( JULY-2018 )_JULY-2018 (OCT-18)Document1 pagePGSUP - 9198 - D.M. CARDIAC ANAESTHESIA - CANTP3 ( JULY-2018 )_JULY-2018 (OCT-18)prem kotiNo ratings yet
- Pgsup - 9199 - d.m. Cardiac Anaesthesia - Cantp4 ( July-2018 )_july-2018 (Oct-18)Document1 pagePgsup - 9199 - d.m. Cardiac Anaesthesia - Cantp4 ( July-2018 )_july-2018 (Oct-18)prem kotiNo ratings yet
- Pgsup - 9199 - d.m. Cardiac Anaesthesia - Cantp4 ( July-2018 )_july-2018 (Oct-18)Document1 pagePgsup - 9199 - d.m. Cardiac Anaesthesia - Cantp4 ( July-2018 )_july-2018 (Oct-18)prem kotiNo ratings yet
- Stenotic Lesions AaDocument7 pagesStenotic Lesions Aaprem kotiNo ratings yet
- Pro-Forma For Display of Information On The College WebsiteDocument16 pagesPro-Forma For Display of Information On The College Websiteprem kotiNo ratings yet
- PHARMACOLOGYDocument2 pagesPHARMACOLOGYprem kotiNo ratings yet
- Postoperative Nausea and VomitingDocument45 pagesPostoperative Nausea and Vomitingprem kotiNo ratings yet
- Anemia in PregnancyDocument9 pagesAnemia in Pregnancyprem kotiNo ratings yet
- Microbiology Final Exam MaterialDocument37 pagesMicrobiology Final Exam MaterialEdgar Mandeng100% (1)
- Second Periodical Test in ScienceDocument2 pagesSecond Periodical Test in ScienceLorraine lee100% (1)
- Drug StudyDocument1 pageDrug StudyKRISTIL MARIE CHAVEZNo ratings yet
- Bone Structure and DiseasesDocument191 pagesBone Structure and DiseasesDrRobin SabharwalNo ratings yet
- Consensus Based Guidelines For The Recognition,.15Document13 pagesConsensus Based Guidelines For The Recognition,.15ms98alissaNo ratings yet
- GMMMG Dental Prescribing Guidelines February 2020 v1 0Document4 pagesGMMMG Dental Prescribing Guidelines February 2020 v1 0Erick GuanoluisaNo ratings yet
- BGS ISBT Antigens Antibodies and Associated DiseasesDocument1 pageBGS ISBT Antigens Antibodies and Associated DiseasesIya BangalanNo ratings yet
- A Successful Case Study On Ayurvedic Management of HypothyroidismDocument6 pagesA Successful Case Study On Ayurvedic Management of HypothyroidismIJRASETPublicationsNo ratings yet
- DR Vibhor PardasaniDocument19 pagesDR Vibhor PardasaniPushpanjali Crosslay HospitalNo ratings yet
- COVID-19 in PH: WHO supports DOH responseDocument2 pagesCOVID-19 in PH: WHO supports DOH responseLegal Affairs OfficeNo ratings yet
- Legg Calvé Perthes DiseaseDocument19 pagesLegg Calvé Perthes DiseaseFranklin Pito JellaNo ratings yet
- Lesson Plan in English Transcode Linear To Non Linear and Vice VersaDocument5 pagesLesson Plan in English Transcode Linear To Non Linear and Vice VersaRoneca BatucanNo ratings yet
- Catch-Up Friday Teaching Guide - LamanilaoDocument3 pagesCatch-Up Friday Teaching Guide - LamanilaoLamanilao Calubag Eludo JoiceanneNo ratings yet
- Schizophrenia Clinical Case StudyDocument13 pagesSchizophrenia Clinical Case Studyapi-497473260100% (1)
- الميكروبيولوجى والتحكم فى العدوىDocument115 pagesالميكروبيولوجى والتحكم فى العدوىmahmoud salahNo ratings yet
- Chapter 05 - Food Safety and SanitationDocument15 pagesChapter 05 - Food Safety and SanitationĐặng ĐạtNo ratings yet
- Human Disorder & Gene TherapyDocument14 pagesHuman Disorder & Gene Therapyulfh08152No ratings yet
- Final Exams - NUTRI EXAM FINALSDocument27 pagesFinal Exams - NUTRI EXAM FINALSJana Patricia JalovaNo ratings yet
- Final Assessment TaskDocument1 pageFinal Assessment TaskHERLIN HOBAYANNo ratings yet
- SEO-Optimized Title for Febrile Seizures and Ear Infection DocumentDocument6 pagesSEO-Optimized Title for Febrile Seizures and Ear Infection DocumentKirstin del CarmenNo ratings yet
- Headache Oet ReadingDocument22 pagesHeadache Oet ReadinglianausinNo ratings yet
- Medical Certificate for Cough, Sore Throat, HeadacheDocument1 pageMedical Certificate for Cough, Sore Throat, HeadacheJareena SamsonNo ratings yet
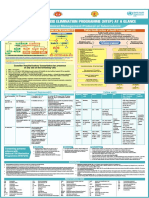
- NTEP at A Glance - Comprehensive Clinical Management Protocol For TBDocument1 pageNTEP at A Glance - Comprehensive Clinical Management Protocol For TBNael NajeebNo ratings yet
- Hemorhhoids CssDocument31 pagesHemorhhoids CssNaren RenNo ratings yet
- SEO Roundworms GuideDocument26 pagesSEO Roundworms GuideCzerinne Angela Justinne AlarillaNo ratings yet
- Sensory GanglionopathyDocument6 pagesSensory GanglionopathyEdwin MedinaNo ratings yet
- Askep Bahasa Inggris SaneDocument12 pagesAskep Bahasa Inggris SaneRio FernandoNo ratings yet
- PROTOCOL of Management of Critical CasesDocument131 pagesPROTOCOL of Management of Critical Casesaziz.shokry.mosaNo ratings yet
- Fill in The Blanks Using "Should" or Shouldn't and A Suitable Verb From The List ProvidedDocument1 pageFill in The Blanks Using "Should" or Shouldn't and A Suitable Verb From The List ProvidedDragana ZafirovskaNo ratings yet
- 1700 Updated Sept 2016 DR KhalidDocument607 pages1700 Updated Sept 2016 DR KhalidTaliya CherianNo ratings yet