You might also like
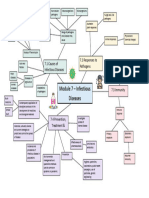
- Module 7 Mind Map BiologyDocument1 pageModule 7 Mind Map BiologyAltSpace TimeNo ratings yet
- PRTG Report 400 - Summary Report For All Sensors - Created 2023-09-01 23-05-02 (2023-08-25 00-00 - 2023-09-01 00-00) UTCDocument9 pagesPRTG Report 400 - Summary Report For All Sensors - Created 2023-09-01 23-05-02 (2023-08-25 00-00 - 2023-09-01 00-00) UTCMuhammed KunnappillyNo ratings yet
- xxx-ILC 4.2-024 Poster-Shahed Hossain Bangladesh-2 PDFDocument22 pagesxxx-ILC 4.2-024 Poster-Shahed Hossain Bangladesh-2 PDFRahen Rangan100% (1)
- MY Abstract MO 2Document1 pageMY Abstract MO 2Mohammad Ullah NasriNo ratings yet
- USDA Center For Veterinary Biologics Statistics Section: Work InstructionsDocument9 pagesUSDA Center For Veterinary Biologics Statistics Section: Work InstructionsTakeshi MochizukiNo ratings yet
- Spss CokenDocument5 pagesSpss CokenEten MaitaleNo ratings yet
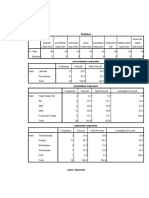
- Frequencies Frequency Table: Jenis KelaminDocument4 pagesFrequencies Frequency Table: Jenis Kelaminちかお 千春No ratings yet
- IdentitasDocument5 pagesIdentitasNadia NingsihNo ratings yet
- Particle Size Analysis: - Chapter 3Document50 pagesParticle Size Analysis: - Chapter 3Aleena SiddiquiNo ratings yet
- Empagliflozin and Linagliptin 2020 Sept FinalDocument65 pagesEmpagliflozin and Linagliptin 2020 Sept FinalJenny Calapati TorrijosNo ratings yet
- FrekuensiDocument3 pagesFrekuensiAhmad BukhariNo ratings yet
- Long Term Mental Health and Social Support in Victims of Disaster Comparison With A General Population Sample ErratumDocument2 pagesLong Term Mental Health and Social Support in Victims of Disaster Comparison With A General Population Sample ErratumNur PurwatiNo ratings yet
- Univariat EcakDocument9 pagesUnivariat EcakTheresa EditNo ratings yet
- Book 2Document2 pagesBook 2Chase MenardyNo ratings yet
- Ritonavir 5Document2 pagesRitonavir 5tengku zadeqNo ratings yet
- Analisis Univariat Dan BivariatDocument10 pagesAnalisis Univariat Dan BivariatAyangNo ratings yet
- Statistics: (Dataset1)Document16 pagesStatistics: (Dataset1)KURNIANo ratings yet
- Test Document 4Document25 pagesTest Document 4Ufuk YazganNo ratings yet
- Hazard CharacterizationDocument17 pagesHazard CharacterizationAnthony OkpeNo ratings yet
- Cote Divoire - Africa - RE - SPDocument4 pagesCote Divoire - Africa - RE - SPowusuansahphilip17No ratings yet
- Frequencies: FREQUENCIES VARIABLES Service Capital Form /statistics Mean /piechart Percent /order AnalysisDocument19 pagesFrequencies: FREQUENCIES VARIABLES Service Capital Form /statistics Mean /piechart Percent /order AnalysisAysNo ratings yet
- HCD 3,5/50-II: General Lens DataDocument2 pagesHCD 3,5/50-II: General Lens DataZbigniew LipinskiNo ratings yet
- FMD Research PakistanDocument5 pagesFMD Research PakistanQuratulainNo ratings yet
- Lesson 2: Summarizing DataDocument53 pagesLesson 2: Summarizing DataminhchauNo ratings yet
- Analisis BerlianaDocument8 pagesAnalisis BerlianaBerliana PangestuNo ratings yet
- DISTRIBUSIDocument3 pagesDISTRIBUSIanthoNo ratings yet
- IcceDocument13 pagesIcceAhmad NersNo ratings yet
- Fokkens EPOS 2020 Chronic Rhinosinusitis How To Implement Current and New Treatment OptionsDocument22 pagesFokkens EPOS 2020 Chronic Rhinosinusitis How To Implement Current and New Treatment OptionsGiuseppe MeccarielloNo ratings yet
- DatttDocument10 pagesDatttRachmat Wihandana AgasiNo ratings yet
- Far FRR EERDocument8 pagesFar FRR EERelf100% (1)
- Frequency 1Document3 pagesFrequency 1Nika Mei Hendra NingrumNo ratings yet
- Dis Frek 1Document4 pagesDis Frek 1sudartoNo ratings yet
- Full Download Business Statistics in Practice 7th Edition Bowerman Solutions ManualDocument35 pagesFull Download Business Statistics in Practice 7th Edition Bowerman Solutions Manualcomnickshay100% (26)
- Output Kak LinaDocument7 pagesOutput Kak Linakelompoksatu cpnsNo ratings yet
- France Europe RE SPDocument4 pagesFrance Europe RE SPCarmen CastroNo ratings yet
- Uji LengkapDocument4 pagesUji LengkapAlans FabrezinNo ratings yet
- EstadisticaDocument2 pagesEstadisticaAntonio Jesus Jaen LopezNo ratings yet
- Tabla de AconDocument2 pagesTabla de AconAntonio Jesus Jaen LopezNo ratings yet
- OutputDocument4 pagesOutputNUR SYAKIRAH BINTI ABD SAMAD MoeNo ratings yet
- OutputDocument4 pagesOutputNUR SYAKIRAH BINTI ABD SAMAD MoeNo ratings yet
- Frequency Table: Lampiran VDocument7 pagesFrequency Table: Lampiran VJhenk Lidya Dhydi KorosiNo ratings yet
- Bern Klein Bulk Sorting Abstract2Document3 pagesBern Klein Bulk Sorting Abstract2Luis Katsumoto Huere AnayaNo ratings yet
- Nama: Fitriyani Kelas: Profesi Ners Tingkat III NIM: P37320218014Document3 pagesNama: Fitriyani Kelas: Profesi Ners Tingkat III NIM: P37320218014fitriyani israNo ratings yet
- Nilai UTSDocument10 pagesNilai UTSparida tuahenaNo ratings yet
- Lampiran 5-8Document6 pagesLampiran 5-8Fajri WengkengNo ratings yet
- Hasil Output SPSS1Document3 pagesHasil Output SPSS1ちかお 千春No ratings yet
- Fox 7th ISM ch07-13Document1 pageFox 7th ISM ch07-13Ramón RamalhoNo ratings yet
- Survey ResearchDocument7 pagesSurvey Researchnithin talluriNo ratings yet
- Hasil SPSSDocument8 pagesHasil SPSStatapsrbNo ratings yet
- Representation of The Market Mechanism of Income Distribution Using Lorenz Curve. Gini Coefficient.Document8 pagesRepresentation of The Market Mechanism of Income Distribution Using Lorenz Curve. Gini Coefficient.Мария МариничNo ratings yet
- Pareto Chart Weekly DataDocument3 pagesPareto Chart Weekly DataIl Meravigliosõ AmirNo ratings yet
- MATH 1280-Unit 1 Learning JournalDocument1 pageMATH 1280-Unit 1 Learning JournalRegNo ratings yet
- OutputDocument7 pagesOutputica maresaNo ratings yet
- Activity 10 Data Presentation Part IIDocument7 pagesActivity 10 Data Presentation Part IIZYRAH LUKE E. VILBARNo ratings yet
- Student Evals s22Document8 pagesStudent Evals s22api-652606702No ratings yet
- Hasil Spss NewDocument13 pagesHasil Spss NewrusliNo ratings yet
- Spss Mas UmarDocument14 pagesSpss Mas UmarAnis yuliantiNo ratings yet
- Frequencies: StatisticsDocument9 pagesFrequencies: StatisticsPutu ErikawatiNo ratings yet
- Medicolegal Issues With Substance AbusersDocument23 pagesMedicolegal Issues With Substance AbusersHazdalila Yais RazaliNo ratings yet
- HASILDocument44 pagesHASILbintanglestariNo ratings yet
- Applied Time Series Econometrics: A Practical Guide for Macroeconomic Researchers with a Focus on AfricaFrom EverandApplied Time Series Econometrics: A Practical Guide for Macroeconomic Researchers with a Focus on AfricaRating: 3 out of 5 stars3/5 (1)
- Optimizacija Doze U Razvoju LekaDocument301 pagesOptimizacija Doze U Razvoju LekaLancre witchNo ratings yet
- End of Life Costs of Medical Care For Advanced Stage Cancer Patients VSP 2015Document8 pagesEnd of Life Costs of Medical Care For Advanced Stage Cancer Patients VSP 2015Lancre witchNo ratings yet
- Asthma Medication Use and Air Pollution in California A Cross-Sectional AnalysisDocument37 pagesAsthma Medication Use and Air Pollution in California A Cross-Sectional AnalysisLancre witchNo ratings yet
- Studies of Sunscreens: Percutaneous Absorption of Benzophenone-3 and PhotostabilityDocument55 pagesStudies of Sunscreens: Percutaneous Absorption of Benzophenone-3 and PhotostabilityLancre witchNo ratings yet
- Medical Abbreviations Pharmacotherapy Case PDFDocument15 pagesMedical Abbreviations Pharmacotherapy Case PDFLancre witchNo ratings yet
- Conversion Factors and Anthropometrics : Appendix ADocument4 pagesConversion Factors and Anthropometrics : Appendix ALancre witchNo ratings yet
- EMA Guidelines Modified Release 2013 DraftDocument38 pagesEMA Guidelines Modified Release 2013 DraftLancre witchNo ratings yet
- June 2017: The Value of Innovation in Decision MakingDocument2 pagesJune 2017: The Value of Innovation in Decision MakingLancre witchNo ratings yet
- BMJ Costing in Economic EvaluationDocument1 pageBMJ Costing in Economic EvaluationLancre witchNo ratings yet
- Opportunistic Infections: Dr. Baldev S. PrajapatiDocument69 pagesOpportunistic Infections: Dr. Baldev S. PrajapatiZazzZaffaNo ratings yet
- Molecular Biology: ICMR Registration No: RPPLPMPDocument2 pagesMolecular Biology: ICMR Registration No: RPPLPMPMaths Tricks solution Mr. G CNo ratings yet
- Southampton Grading SystemDocument5 pagesSouthampton Grading SystemswestyNo ratings yet
- Dysfunctional Labor As One of The Intrapartal ComplicationsDocument23 pagesDysfunctional Labor As One of The Intrapartal ComplicationsKenje Kate AgripoNo ratings yet
- Dok 21Document2 pagesDok 21dr. Noni PrisciliaNo ratings yet
- EKG Self Study GuideDocument40 pagesEKG Self Study GuideArgee AlonsabeNo ratings yet
- Chapter 15 Introduction To The Immune Response and InflammationDocument4 pagesChapter 15 Introduction To The Immune Response and InflammationTan AdonnisNo ratings yet
- Atreyi Chakraborty, Et AlDocument9 pagesAtreyi Chakraborty, Et Alkavya bharadhwajNo ratings yet
- Bi-Level Pressure Ventilation Assistive Device For Pulmonary Ailments and Overlap SyndromesDocument4 pagesBi-Level Pressure Ventilation Assistive Device For Pulmonary Ailments and Overlap SyndromesMuhammad Bin AjmalNo ratings yet
- M-1 MCQDocument88 pagesM-1 MCQFrt TrfNo ratings yet
- NCP FormatDocument2 pagesNCP FormatLorie Yvonne Quibin AgullanaNo ratings yet
- Croup - Clinical Features, Evaluation, and Diagnosis - UpToDateDocument43 pagesCroup - Clinical Features, Evaluation, and Diagnosis - UpToDateRafaela BassettiNo ratings yet
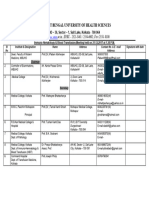
- Danh Mục Sách Điện Tử: Trường Đại Học Y DượC Huế T.T Thông Tin Thư ViệnDocument8 pagesDanh Mục Sách Điện Tử: Trường Đại Học Y DượC Huế T.T Thông Tin Thư ViệnLinh TinhNo ratings yet
- Cardio SNAP-BNP NT-proBNP IdexxDocument4 pagesCardio SNAP-BNP NT-proBNP IdexxXenia FernandezNo ratings yet
- Quality Control in HistopathologyDocument30 pagesQuality Control in HistopathologyMuhammad Jamiu Bello78% (9)
- Terapi Farmakologi Pada GeriatriDocument41 pagesTerapi Farmakologi Pada GeriatriFauzi SatriaNo ratings yet
- Management Emesis GravidarumDocument8 pagesManagement Emesis GravidarumDewi KurniasariNo ratings yet
- Research ArticleDocument8 pagesResearch ArticleHappy Martha NababanNo ratings yet
- Valori Contract An. 2023 - Paraclinic - 20.09.2023Document21 pagesValori Contract An. 2023 - Paraclinic - 20.09.2023Matteo si Sofia vlog'sNo ratings yet
- Dates Lab Clin Clin Tasks Attempted 1 2 3 4 5 6 7: UWISON Revised 2014-2015,2018 IM MedicationDocument4 pagesDates Lab Clin Clin Tasks Attempted 1 2 3 4 5 6 7: UWISON Revised 2014-2015,2018 IM MedicationRasheda PickettNo ratings yet
- Prelim Activity 1 - Health TeachingsDocument2 pagesPrelim Activity 1 - Health TeachingsNICOLE MAGLAQUINo ratings yet
- Macrolides and LincosamidesDocument22 pagesMacrolides and LincosamidesSunilNo ratings yet
- Anal FissureDocument3 pagesAnal FissureBhaveen ShethNo ratings yet
- Hemoperitoneum From Corpus Luteum Cyst Rupture in Pregnancy of Unknown LocationDocument4 pagesHemoperitoneum From Corpus Luteum Cyst Rupture in Pregnancy of Unknown Locationlina ukagoNo ratings yet
- Acute Otitis Media Children and AdolescentsDocument1 pageAcute Otitis Media Children and AdolescentsSreya SanilNo ratings yet
- BreastfeedingDocument144 pagesBreastfeedingayu_pieterNo ratings yet
- Transplantation Immunology: Dr.T.V.Rao MDDocument59 pagesTransplantation Immunology: Dr.T.V.Rao MDtummalapalli venkateswara rao100% (2)
- Immuno Hematology Blood TransfusionDocument1 pageImmuno Hematology Blood Transfusionudiptya_papai2007No ratings yet
- Antibiotik Pada Infeksi Tropis (PERSI)Document42 pagesAntibiotik Pada Infeksi Tropis (PERSI)YULINo ratings yet