You might also like
- PharmacologyDocument25 pagesPharmacologygregNo ratings yet
- Krok1 2014pharmacology 170411104357Document25 pagesKrok1 2014pharmacology 170411104357JAGUNo ratings yet
- PharmacologyDocument22 pagesPharmacologyJack frimpongNo ratings yet
- Pharmacology Mid ExamDocument7 pagesPharmacology Mid ExamHSC UNITEDNo ratings yet
- Pharma 2Document3 pagesPharma 2zaydeeeeNo ratings yet
- Pharmacology BDocument5 pagesPharmacology Bttdjhg2p6kNo ratings yet
- CLINICAL PHARMA QuestionsDocument13 pagesCLINICAL PHARMA QuestionsAminatNo ratings yet
- Test Exam Pharmacology (Modul 1)Document120 pagesTest Exam Pharmacology (Modul 1)Musa yohanaNo ratings yet
- Pharma 1Document22 pagesPharma 1zaydeeeeNo ratings yet
- 2014 Internal COC PharmaDocument16 pages2014 Internal COC PharmategenezewudeNo ratings yet
- Test Tasks On Pharmacology Module2Document19 pagesTest Tasks On Pharmacology Module2Blessing NwosuNo ratings yet
- Q6 Cardiovascular PharmacologyDocument4 pagesQ6 Cardiovascular PharmacologyHainey GayleNo ratings yet
- PharmacologyDocument141 pagesPharmacologyOmowunmi KadriNo ratings yet
- Situational Tasks Such As KROK Pharmacology English Sem 6Document17 pagesSituational Tasks Such As KROK Pharmacology English Sem 6Mi PatelNo ratings yet
- Vocabulary Test Practice On Pharmacology.Document21 pagesVocabulary Test Practice On Pharmacology.illia1028No ratings yet
- General Pharma McqsDocument11 pagesGeneral Pharma McqsAyesha .No ratings yet
- ANS QuestionsDocument5 pagesANS Questionsparanoea911No ratings yet
- Krok - Base PharmacologyDocument149 pagesKrok - Base PharmacologyHemant GargNo ratings yet
- General Pharma Mcqs 2Document11 pagesGeneral Pharma Mcqs 2hassan qureshiNo ratings yet
- КРОК 02.2024 Мед, Стом, Фарм - Анг, УкрDocument22 pagesКРОК 02.2024 Мед, Стом, Фарм - Анг, УкрpharmacologyNo ratings yet
- MBBS Question Paper I 2023 NAKDocument4 pagesMBBS Question Paper I 2023 NAKsuhaiqbal16No ratings yet
- MCQ Base For Final Exam PreparationDocument131 pagesMCQ Base For Final Exam PreparationPurwa Rane100% (1)
- Pharm Retake QuestionsDocument16 pagesPharm Retake QuestionsUneke EdwardsNo ratings yet
- Module Tests V-1Document8 pagesModule Tests V-1ahmad summerNo ratings yet
- Type A Choice Questions (Only One Answer Is Correct) : A. B. C. D. EDocument10 pagesType A Choice Questions (Only One Answer Is Correct) : A. B. C. D. ERAED GhunaimNo ratings yet
- Pharma QuestionsDocument13 pagesPharma QuestionsSarah Mae SinceroNo ratings yet
- NP3 ExamDocument14 pagesNP3 ExamArnie Jude CaridoNo ratings yet
- LPN Jan 1Document49 pagesLPN Jan 1wltnz0418No ratings yet
- Chapter 22Document6 pagesChapter 22Danielle ShullNo ratings yet
- Study Questions-Medical Pharmacology - MED 301 - Drugs Used in Coardiovascular Disorders - Prof. Nedret AltıokDocument16 pagesStudy Questions-Medical Pharmacology - MED 301 - Drugs Used in Coardiovascular Disorders - Prof. Nedret Altıokفاعل خيرNo ratings yet
- Pharmacology FINALLLpdfDocument223 pagesPharmacology FINALLLpdfRitika NigamNo ratings yet
- Name Honor Pledge (Signature) : Questions 1 - 2 Refer To The Following CaseDocument9 pagesName Honor Pledge (Signature) : Questions 1 - 2 Refer To The Following CasegregstevensNo ratings yet
- Pharmacology Exam 4 ReviewDocument8 pagesPharmacology Exam 4 ReviewAnonymous 0Yvbef1xNo ratings yet
- Pharmacology Pgi Compre Recall & Ratio December 2017: Cardiovascular DrugsDocument16 pagesPharmacology Pgi Compre Recall & Ratio December 2017: Cardiovascular DrugsSaravanan DevarajNo ratings yet
- Pharmacology 2 (Phbs 107) Midterm Examination MULTIPLE CHOICE: Each of The Questions, Statements, or Incomplete Statements Can Be CorrectlyDocument17 pagesPharmacology 2 (Phbs 107) Midterm Examination MULTIPLE CHOICE: Each of The Questions, Statements, or Incomplete Statements Can Be CorrectlyT'amo HanashNo ratings yet
- Chapter 6 - Self-Assessment Q&ADocument8 pagesChapter 6 - Self-Assessment Q&AVijay SharmaNo ratings yet
- Module Pharma 1Document21 pagesModule Pharma 1Donya GholamiNo ratings yet
- When You Send Me The Answer Write Your Full Name and ID NumberDocument5 pagesWhen You Send Me The Answer Write Your Full Name and ID Numbermisgna bereketNo ratings yet
- Pharmacology MCQs 4Document6 pagesPharmacology MCQs 4Waseem SarwarNo ratings yet
- Pharm Exam III Nov 18 2014Document6 pagesPharm Exam III Nov 18 2014MouhamadNdGhinwaNo ratings yet
- Pharmacology ADocument4 pagesPharmacology Attdjhg2p6kNo ratings yet
- Drugs Affecting Neurologic SystemDocument5 pagesDrugs Affecting Neurologic SystemjustineGREATNo ratings yet
- MRCP 1 Last MinDocument10 pagesMRCP 1 Last MinDr.yeasin Arafat100% (1)
- Chapter 55 - Drugs Acting On The Lower Respiratory TractDocument13 pagesChapter 55 - Drugs Acting On The Lower Respiratory TractJonathonNo ratings yet
- NP3 RatioDocument17 pagesNP3 RatioArnie Jude CaridoNo ratings yet
- CVS Past Paper 2018Document10 pagesCVS Past Paper 2018Bigabwa BernardNo ratings yet
- CASESDocument36 pagesCASESRoro RageyNo ratings yet
- Tutorial II 2021 No AnsDocument4 pagesTutorial II 2021 No AnsmayaNo ratings yet
- Unit 1-4Document13 pagesUnit 1-4qweyo yhuNo ratings yet
- Dams Bishkek Mcqs Updated LogoDocument2 pagesDams Bishkek Mcqs Updated LogoSnamNo ratings yet
- KMMMMMMMMMMMMMMMMDocument14 pagesKMMMMMMMMMMMMMMMMJerecel Gapi VigoNo ratings yet
- Post Test - Pharma (Students Copy)Document5 pagesPost Test - Pharma (Students Copy)irish felix100% (1)
- GROUP3 Multiple-ChoiceDocument4 pagesGROUP3 Multiple-Choicelea mae andoloyNo ratings yet
- HypertensionDocument16 pagesHypertensionElias IbrahimNo ratings yet
- حل النموذج النصفيDocument2 pagesحل النموذج النصفيقابوس بن سعيدNo ratings yet
- 2Document13 pages2RAED GhunaimNo ratings yet
- Unit 9 Drugs Acting On The Cardiovascular SystemDocument72 pagesUnit 9 Drugs Acting On The Cardiovascular SystemTherese Margarette SantiagoNo ratings yet
- 18Document5 pages18Mekeshia SanchezNo ratings yet
- Splenomegaly: Involvement Is CommonDocument1 pageSplenomegaly: Involvement Is CommonMadeline WanhartNo ratings yet
- "Approwed" On The Meeting of The Department of Surgical Dentistry and Maxillofacial SurgeryDocument10 pages"Approwed" On The Meeting of The Department of Surgical Dentistry and Maxillofacial SurgeryMadeline WanhartNo ratings yet
- Topic 2Document3 pagesTopic 2Madeline WanhartNo ratings yet
- Topic 4Document3 pagesTopic 4Madeline WanhartNo ratings yet
- Topic 20. X-RayDocument4 pagesTopic 20. X-RayMadeline WanhartNo ratings yet
- "Approwed" On The Meeting of The Department of Surgical Dentistry and Maxillofacial SurgeryDocument9 pages"Approwed" On The Meeting of The Department of Surgical Dentistry and Maxillofacial SurgeryMadeline WanhartNo ratings yet
- Topic 3Document4 pagesTopic 3Madeline WanhartNo ratings yet
- Topic 22. X-RayDocument5 pagesTopic 22. X-RayMadeline WanhartNo ratings yet
- Gross-View Cases and Histological SlidesDocument1 pageGross-View Cases and Histological SlidesMadeline WanhartNo ratings yet
- Gross-View Samples and Histological SlidesDocument4 pagesGross-View Samples and Histological SlidesMadeline WanhartNo ratings yet
- Topic 23. X-RayDocument2 pagesTopic 23. X-RayMadeline WanhartNo ratings yet
- Theme 27. Chronic Obstructive Pulmonary Diseases. Pneumoconioses. Cor PulmonaleDocument3 pagesTheme 27. Chronic Obstructive Pulmonary Diseases. Pneumoconioses. Cor PulmonaleMadeline WanhartNo ratings yet
- Theme 21. Blood Cell DiseasesDocument3 pagesTheme 21. Blood Cell DiseasesMadeline WanhartNo ratings yet
- Topic 4Document2 pagesTopic 4Madeline WanhartNo ratings yet
- Topic 1Document2 pagesTopic 1Madeline WanhartNo ratings yet
- Topic 9 Nonparametric CriteriaDocument14 pagesTopic 9 Nonparametric CriteriaMadeline WanhartNo ratings yet
- Topic 3Document3 pagesTopic 3Madeline WanhartNo ratings yet
- Topic 5Document3 pagesTopic 5Madeline WanhartNo ratings yet
- Topic 2Document4 pagesTopic 2Madeline WanhartNo ratings yet
- Topic 6 Dynamic SeriesDocument29 pagesTopic 6 Dynamic SeriesMadeline WanhartNo ratings yet
- Topic 8 Parametric MethodsDocument14 pagesTopic 8 Parametric MethodsMadeline WanhartNo ratings yet
- Topic 10 Survival Analysis. LethalityDocument17 pagesTopic 10 Survival Analysis. LethalityMadeline WanhartNo ratings yet
- Topic 7 Method of StandardizationDocument11 pagesTopic 7 Method of StandardizationMadeline WanhartNo ratings yet
- Daftar ObatDocument27 pagesDaftar Obathanny nuguNo ratings yet
- Pebc Evaluating Exam Sample QuestionDocument50 pagesPebc Evaluating Exam Sample QuestionZain zanzoonNo ratings yet
- Manual Neo 900Document76 pagesManual Neo 900Bismarck Pablo Ibañez Piotti67% (3)
- SPC Marbonor 100 MLDocument6 pagesSPC Marbonor 100 MLJelena TerzicNo ratings yet
- Chalcone Synthesis, Structure DiversityDocument13 pagesChalcone Synthesis, Structure DiversityDini Elsi ANo ratings yet
- Endocrine Glands The Producers of Chemical MessengersDocument10 pagesEndocrine Glands The Producers of Chemical Messengersahmed100% (1)
- Materi IAI Palangka Raya - Rev PDFDocument55 pagesMateri IAI Palangka Raya - Rev PDFNopernas CahayaNo ratings yet
- Reiki 1Document19 pagesReiki 1api-246890707No ratings yet
- Buffalo LeprosyDocument4 pagesBuffalo LeprosyALTAF HUSAINNo ratings yet
- Corpal Nindya Duri IkanDocument10 pagesCorpal Nindya Duri IkanRadianNasutionNo ratings yet
- Negative Effects of Video GamesDocument5 pagesNegative Effects of Video GamesMadeNo ratings yet
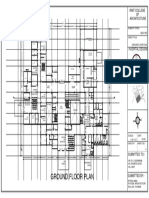
- Ground Floor Plan Sheet 2Document1 pageGround Floor Plan Sheet 2riteshNo ratings yet
- Health Services in WADocument10 pagesHealth Services in WAlaureeateNo ratings yet
- Stages of Labor and DeliveryDocument4 pagesStages of Labor and DeliveryvienreyNo ratings yet
- Evaluation Checklist Case 7 Bronchial AsthmaDocument7 pagesEvaluation Checklist Case 7 Bronchial AsthmaChristian MendiolaNo ratings yet
- D. Santhi Krupa, Et Al IJAPRDocument6 pagesD. Santhi Krupa, Et Al IJAPRAtraoNo ratings yet
- DolcetDocument3 pagesDolcetConn_Casipe_8158100% (4)
- Methods of ToiletDocument180 pagesMethods of Toiletathegeha100% (2)
- MedicineDocument17 pagesMedicineSubhashini R0% (1)
- EDIC Guidelines 2017 PDFDocument22 pagesEDIC Guidelines 2017 PDFZia ShaikhNo ratings yet
- Full Text of PT-OT Exam Results (Top 10)Document2 pagesFull Text of PT-OT Exam Results (Top 10)TheSummitExpressNo ratings yet
- Basic Priciples of Heart SurgeryDocument6 pagesBasic Priciples of Heart SurgeryprofarmahNo ratings yet
- AJODO 1993 Facial Keys To Orth DX and TX Plann Part I ARNETTDocument14 pagesAJODO 1993 Facial Keys To Orth DX and TX Plann Part I ARNETTCarito Aguirre Lindo100% (1)
- Drug Descrubrimiento de FarmacosDocument302 pagesDrug Descrubrimiento de FarmacosdavidNo ratings yet
- +bashkir State Medical UniversityDocument2 pages+bashkir State Medical UniversityCB SharmaNo ratings yet
- Turkey Tail MushroomDocument10 pagesTurkey Tail Mushroomjuanitos111100% (2)
- JCIA Handbook 2020Document61 pagesJCIA Handbook 2020WAQASNo ratings yet
- Homeless Veterans 1Document2 pagesHomeless Veterans 1api-317128838No ratings yet
- Connecticut Health PlanDocument2 pagesConnecticut Health PlanHelen BennettNo ratings yet
- Cardiac PoisonsDocument36 pagesCardiac PoisonsTARIQNo ratings yet