You might also like
- PCOS Ebook v1.18Document22 pagesPCOS Ebook v1.18க100% (2)
- How To Reverse Polycystic Ovary SyndromeDocument24 pagesHow To Reverse Polycystic Ovary SyndromeJudi Ann MagsacayNo ratings yet
- Abnormal PsychologyDocument33 pagesAbnormal PsychologyChristie SabgaNo ratings yet
- 23 Understanding PCOS, The Hidden EpidemicDocument29 pages23 Understanding PCOS, The Hidden EpidemicgreenbeeNo ratings yet
- PCOS Patient HandoutDocument16 pagesPCOS Patient HandoutAnonymous NI5oJfd2cNo ratings yet
- How To Get Pregnant With PcosDocument20 pagesHow To Get Pregnant With PcosConfused parentNo ratings yet
- Polycystic Ovary Syndrome (PCOS)Document6 pagesPolycystic Ovary Syndrome (PCOS)saleemut3No ratings yet
- Polycystic Ovary Syndrome 2Document22 pagesPolycystic Ovary Syndrome 2Michelle Panlilio0% (1)
- Readers Digest Asia Feburary 2021Document134 pagesReaders Digest Asia Feburary 2021FURY FURIONNo ratings yet
- Polycystic Ovarian Syndrome (PCOS)Document10 pagesPolycystic Ovarian Syndrome (PCOS)Juliet Amondi100% (1)
- Polycystic Ovary Syndrome (PCOS) : Beyond InfertilityDocument32 pagesPolycystic Ovary Syndrome (PCOS) : Beyond InfertilityKristi Hollenbeck-NeufeldNo ratings yet
- Indian Research Funding AgenciesDocument6 pagesIndian Research Funding AgencieskcchtphdNo ratings yet
- Factories ActDocument64 pagesFactories ActKrishna Kaushik100% (1)
- Power Over Pcos EbookDocument160 pagesPower Over Pcos EbookIra Ayu Lestari100% (2)
- Polycystic Ovary Syndrome (PCOS) : Symptoms, Causes, and TreatmentDocument19 pagesPolycystic Ovary Syndrome (PCOS) : Symptoms, Causes, and TreatmentGrace Ann Rodriguez SanDiegoNo ratings yet
- Uworld RationalesDocument2 pagesUworld RationalesMelissa Sapp67% (3)
- OB 2.5 Intrapartum AssessmentDocument9 pagesOB 2.5 Intrapartum AssessmentisahNo ratings yet
- Chevron Thailand Employee and Contractor Handbook EngDocument200 pagesChevron Thailand Employee and Contractor Handbook EngAndré Lima100% (1)
- PCOS: A Step-By-Step Guide to Reverse Polycystic Ovary Syndrome, Balance Your Hormones, Boost Your Metabolism, & Restore Your FertilityFrom EverandPCOS: A Step-By-Step Guide to Reverse Polycystic Ovary Syndrome, Balance Your Hormones, Boost Your Metabolism, & Restore Your FertilityRating: 3.5 out of 5 stars3.5/5 (20)
- How to Beat PCOS Naturally & Regain a Healthy & Fertile Life Now ( A Simple Guide on PCOS Diet & Exercises to Conquer PCOS Permanently Today)From EverandHow to Beat PCOS Naturally & Regain a Healthy & Fertile Life Now ( A Simple Guide on PCOS Diet & Exercises to Conquer PCOS Permanently Today)Rating: 3.5 out of 5 stars3.5/5 (6)
- Brochure Philippine Laws On Environmental PollutionDocument8 pagesBrochure Philippine Laws On Environmental PollutionElvin JuniorNo ratings yet
- Levels of PreventionDocument23 pagesLevels of Preventionkuruvagadda sagar100% (1)
- PCOS No More: Take Control of PCOS Symptoms & Treatments - A Holistic System of Lifestyle Changes, Diet, & Exercises to Beat Polycystic Ovary Syndrome Naturally & Permanently. PCOS Recipes Included.From EverandPCOS No More: Take Control of PCOS Symptoms & Treatments - A Holistic System of Lifestyle Changes, Diet, & Exercises to Beat Polycystic Ovary Syndrome Naturally & Permanently. PCOS Recipes Included.Rating: 4 out of 5 stars4/5 (3)
- Intrebari Interviu Asistent MedicalDocument3 pagesIntrebari Interviu Asistent MedicalanaNo ratings yet
- Assignment: Polycystic Ovary Syndrome (PCOS)Document8 pagesAssignment: Polycystic Ovary Syndrome (PCOS)tehseenullahNo ratings yet
- Dark Green Vintage Minimalist Aesthetic Newspaper Fashion Marketing Ad Instagram StoryDocument4 pagesDark Green Vintage Minimalist Aesthetic Newspaper Fashion Marketing Ad Instagram StoryJana Emery SumagangNo ratings yet
- .K Uh, IDocument18 pages.K Uh, IRahul AgarwalNo ratings yet
- PCOSDocument3 pagesPCOSpravallikakvNo ratings yet
- Polycystic Ovarian SyndromeDocument18 pagesPolycystic Ovarian Syndromeshalika42598No ratings yet
- PcosDocument9 pagesPcosMonomay HalderNo ratings yet
- Polycystic Ovary SyndromeDocument5 pagesPolycystic Ovary SyndromeAle W.S.No ratings yet
- Pi Pcos Update-2022 230717 221503Document7 pagesPi Pcos Update-2022 230717 221503PeterNo ratings yet
- PCOS Booklet Final Low Quality Aster IVFDocument8 pagesPCOS Booklet Final Low Quality Aster IVFasterivfNo ratings yet
- Introduction PCOSDocument14 pagesIntroduction PCOSalex.avenko1030No ratings yet
- Pcos - Clinical Case DiscussionDocument4 pagesPcos - Clinical Case Discussionreham macadatoNo ratings yet
- Group 3 - PCOS and SD Written OutputDocument25 pagesGroup 3 - PCOS and SD Written OutputJolly S. SendinNo ratings yet
- Polycystic Ovary Syndrome (PCOS) - Johns Hopkins MedicineDocument5 pagesPolycystic Ovary Syndrome (PCOS) - Johns Hopkins MedicineWINDA NURHASANAHNo ratings yet
- Final Research Essay PcosDocument13 pagesFinal Research Essay Pcosapi-510714949No ratings yet
- Name Class Section Subject: Sohon Sen XI B BiologyDocument36 pagesName Class Section Subject: Sohon Sen XI B BiologySohon SenNo ratings yet
- Polycystic Ovary Syndrome (PCOS) Johns Hopkins MedicineDocument1 pagePolycystic Ovary Syndrome (PCOS) Johns Hopkins MedicinehercimacielNo ratings yet
- Pcod Natural TreatmentDocument4 pagesPcod Natural Treatmenttusharphale100% (1)
- Polycystic Ovarian Syndrome & Role of Homeopathy in PCOSDocument11 pagesPolycystic Ovarian Syndrome & Role of Homeopathy in PCOSSaurav Arora100% (2)
- Research EssayDocument3 pagesResearch Essayapi-510714949No ratings yet
- Polycystic Ovary Syndrome (PCOS) : February 2020Document5 pagesPolycystic Ovary Syndrome (PCOS) : February 2020Lia MeivianeNo ratings yet
- Hormonal Disorder AwarenessDocument6 pagesHormonal Disorder AwarenessRasell Fhaye A. RazonNo ratings yet
- Polycystic Ovary/Ovarian Syndrome (PCOS) : Underrecognized, Underdiagnosed, and UnderstudiedDocument16 pagesPolycystic Ovary/Ovarian Syndrome (PCOS) : Underrecognized, Underdiagnosed, and UnderstudiedcaneNo ratings yet
- What Causes Polycystic Ovarian SyndromeDocument8 pagesWhat Causes Polycystic Ovarian SyndromeKimsha ConcepcionNo ratings yet
- Huerto, Kathrina B. - Reflection - Reproduction CycleDocument2 pagesHuerto, Kathrina B. - Reflection - Reproduction CycleKathrina HuertoNo ratings yet
- Practical Research 2Document66 pagesPractical Research 2Cris Antonette AbataNo ratings yet
- 4 1 36 151Document4 pages4 1 36 151Shelly GargNo ratings yet
- Polycystic Ovary Syndrome (PCOS) - Symptoms, Causes, and TreatmentDocument19 pagesPolycystic Ovary Syndrome (PCOS) - Symptoms, Causes, and TreatmentAkshay HarekarNo ratings yet
- PCOS Forum: Research in Polycystic Ovary Syndrome Today and TomorrowDocument2 pagesPCOS Forum: Research in Polycystic Ovary Syndrome Today and TomorrowTrisha Marie JimenezNo ratings yet
- Grace Lipsini1 2 3Document4 pagesGrace Lipsini1 2 3api-548923370No ratings yet
- Kenneth NegsDocument2 pagesKenneth NegsGwen Stefani DaugdaugNo ratings yet
- Polycystic Ovary SyndromeDocument17 pagesPolycystic Ovary SyndromeramsaybajjuNo ratings yet
- Polycystic Ovarian Syndrome Protocol Carson Newman College Courtney ConnollyDocument7 pagesPolycystic Ovarian Syndrome Protocol Carson Newman College Courtney ConnollycourtneyNo ratings yet
- And Getting Pregnant: A Beginner'S Guide and Patient Stories of HopeDocument23 pagesAnd Getting Pregnant: A Beginner'S Guide and Patient Stories of HopehaurakhansaNo ratings yet
- GADHIYA SUDIP SEC A Endo Gynecology PDFDocument3 pagesGADHIYA SUDIP SEC A Endo Gynecology PDFSudeep GadhiyaNo ratings yet
- A Review and Current Situation of Pcos With InfertilityDocument15 pagesA Review and Current Situation of Pcos With InfertilityIJAR JOURNALNo ratings yet
- Befuddled Between PCOD Versus PCOSDocument2 pagesBefuddled Between PCOD Versus PCOSvedas02 curesNo ratings yet
- Herbal Drugs For The Treatment of Polycystic Ovary Syndrome (Pcos) and Its ComplicationsDocument9 pagesHerbal Drugs For The Treatment of Polycystic Ovary Syndrome (Pcos) and Its ComplicationsDoc MailNo ratings yet
- Polycystic Ovarian Syndrome (PCOS)Document57 pagesPolycystic Ovarian Syndrome (PCOS)Michelle FynesNo ratings yet
- 014 Gowri Pcos BloodDocument15 pages014 Gowri Pcos BloodPriyanka GandhiNo ratings yet
- Hyperandrogenism: Arrest Occurs When The Granulosa Cells of The Ovaries Normally Begin To ProduceDocument7 pagesHyperandrogenism: Arrest Occurs When The Granulosa Cells of The Ovaries Normally Begin To ProduceNathan JeffreyNo ratings yet
- PCODDocument16 pagesPCODfitfemme12126No ratings yet
- Pcod FnalDocument7 pagesPcod FnalpbalasankarNo ratings yet
- Polycystic Ovary SyndromeDocument8 pagesPolycystic Ovary SyndromeTahir BilalNo ratings yet
- Understanding Polycystic Ovary Syndrome: All You Need To KnowDocument32 pagesUnderstanding Polycystic Ovary Syndrome: All You Need To KnowJenNo ratings yet
- Plagrism Copy Last ModfiedDocument41 pagesPlagrism Copy Last ModfiedAfzal MuhammadNo ratings yet
- PcosDocument6 pagesPcosDana MradNo ratings yet
- Oncology Nursing Must Knows by Dr. Chris G. SorongonDocument2 pagesOncology Nursing Must Knows by Dr. Chris G. SorongonAleandro DizonNo ratings yet
- Oncology Nursing: A Sore That Does Not HealDocument2 pagesOncology Nursing: A Sore That Does Not HealAleandro DizonNo ratings yet
- Alzheimers Notes 2Document21 pagesAlzheimers Notes 2Aleandro DizonNo ratings yet
- Alzheimers NotesDocument3 pagesAlzheimers NotesAleandro DizonNo ratings yet
- Common Causes of Calf Pain in Endurance Athletes: by Brad J. Bernardini, MD, FAAOS, Reconstructive OrthopedicsDocument2 pagesCommon Causes of Calf Pain in Endurance Athletes: by Brad J. Bernardini, MD, FAAOS, Reconstructive Orthopedicsbila inunNo ratings yet
- ODMP Sustainable Livestock Management - Watering Points Appendix 1 - Borehole DataDocument35 pagesODMP Sustainable Livestock Management - Watering Points Appendix 1 - Borehole DataAse JohannessenNo ratings yet
- Johnson ReportDocument10 pagesJohnson ReportHarihar SharmaNo ratings yet
- AiepiDocument12 pagesAiepiRenzo Iván Marín DávalosNo ratings yet
- MSPE Noteworthy Characteristics Worksheet: Complete This Worksheet and Bring It To Your Mandatory Career Advising SessionDocument2 pagesMSPE Noteworthy Characteristics Worksheet: Complete This Worksheet and Bring It To Your Mandatory Career Advising SessionHải Dương NguyễnNo ratings yet
- Respaper 1Document48 pagesRespaper 1Xayezi AblenNo ratings yet
- Myocardial Protection - An UpdateDocument67 pagesMyocardial Protection - An UpdateRezwanul Hoque Bulbul100% (5)
- Hba1C: Quality System CertifiedDocument4 pagesHba1C: Quality System CertifiedNonameNo ratings yet
- Foundation of Professional Nursing PracticeDocument5 pagesFoundation of Professional Nursing PracticeIvan LouiseNo ratings yet
- Ergonomic Factors in Construction Industry: A Literature ReviewDocument14 pagesErgonomic Factors in Construction Industry: A Literature ReviewdhanarajNo ratings yet
- Lesson Plan-Pregnant WomenDocument5 pagesLesson Plan-Pregnant Womenapi-270972965No ratings yet
- Flux Cored Arc Welding NC IIDocument73 pagesFlux Cored Arc Welding NC IIAJ AcuñaNo ratings yet
- Assessment Diagnosis Outcomes Intervention Evaluation: Mabini Colleges, Inc. College of Nursing and MidwiferyDocument3 pagesAssessment Diagnosis Outcomes Intervention Evaluation: Mabini Colleges, Inc. College of Nursing and MidwiferyKathrina Mendoza HembradorNo ratings yet
- The Daily Tar Heel For April 12, 2016Document8 pagesThe Daily Tar Heel For April 12, 2016The Daily Tar HeelNo ratings yet
- Nepal New Emerging Pharma MarketDocument5 pagesNepal New Emerging Pharma MarketDeep_HeartNo ratings yet
- Bromine Water - Saturated MSDS: Section 1: Chemical Product and Company IdentificationDocument5 pagesBromine Water - Saturated MSDS: Section 1: Chemical Product and Company IdentificationWinonaNo ratings yet
- Good Practice Review - 8 - Revised2 PDFDocument323 pagesGood Practice Review - 8 - Revised2 PDFsteppevosNo ratings yet
- A Healthy Menopause: Diet, Nutrition and Lifestyle GuidanceDocument8 pagesA Healthy Menopause: Diet, Nutrition and Lifestyle GuidanceAnonymous bq4KY0mcWGNo ratings yet
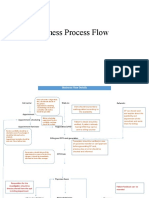
- Business Process FlowDocument12 pagesBusiness Process FlowKumar BalramNo ratings yet
- Catheter WiresDocument56 pagesCatheter WiresSaud ShirwanNo ratings yet