Professional Documents
Culture Documents
Accidente Ofidico NEJM
Uploaded by
Nicole IriarteCopyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
Accidente Ofidico NEJM
Uploaded by
Nicole IriarteCopyright:
Available Formats
The n e w e ng l a n d j o u r na l of m e dic i n e
Review Article
Dan L. Longo, M.D., Editor
Snake Envenomation
Steven A. Seifert, M.D., James O. Armitage, M.D., and Elda E. Sanchez, Ph.D.
S
From the Department of Emergency nake envenomation represents an important health problem in
Medicine and the New Mexico Poison much of the world. In 2009, it was recognized by the World Health Organi-
and Drug Information Center, University
of New Mexico Health Sciences Center, zation (WHO) as a neglected tropical disease, and in 2017, it was elevated
Albuquerque (S.A.S.); the Department of into Category A of the Neglected Tropical Diseases list, further expanding access
Internal Medicine, University of Nebraska to funding for research and antivenoms.1 However, snake envenomation occurs in
Medical Center, Omaha (J.O.A.); and the
National Natural Toxins Research Center both tropical and temperate climates and on all continents except Antarctica.
and the Department of Chemistry, Texas Worldwide, the estimated number of annual deaths due to snake envenomation
A&M University–Kingsville, Kingsville (80,000 to 130,000) is similar to the estimate for drug-resistant tuberculosis and
(E.E.S.). Dr. Seifert can be contacted at
sseifert@salud.unm.edu or at New Mexi- for multiple myeloma.2,3 In countries with adequate resources, deaths are infre-
co Poison and Drug Information Center, quent (e.g., <6 deaths per year in the United States, despite the occurrence of 7000
University of New Mexico Health Sciences to 8000 bites), but in countries without adequate resources, deaths may number in
Center, Albuquerque, NM 87131-0001. Dr.
Armitage can be contacted at joarmita@ the tens of thousands. Venomous snakes kept as pets are not rare, and physicians
unmc.edu or at Department of Internal anywhere might be called on to manage envenomation by a nonnative snake. Im-
Medicine, University of Nebraska Medical portant advances have occurred in our understanding of the biology of venom and
Center, Omaha, NE 68198-6840. Dr. San-
chez can be contacted at e lda.sanchez@ the management of snake envenomation since this topic was last addressed in the
tamuk.edu or at National Natural Toxins Journal two decades ago.4 For the general provider, it is important to understand
Research Center, Department of Chemis- the spectrum of snake envenomation effects and approaches to management and
try, Texas A&M University–Kingsville,
Kingsville, TX 78363-8202. to obtain specific guidance, when needed.
N Engl J Med 2022;386:68-78.
DOI: 10.1056/NEJMra2105228 Epidemiol o gy
Copyright © 2022 Massachusetts Medical Society.
Snakes are predators, and with exceptions (e.g., egg-eating snakes), they subdue
CME their prey through constriction, aggressive biting, and chewing or by using venom.
at NEJM.org
The mechanism of venom delivery varies among major groups of snakes (Fig. 1).
Snakes generally avoid human contact by retreating or hiding. Many species
have defensive mechanisms (e.g., the rattlesnake’s rattle and the cobra’s hooding)
to ward off an organism perceived as a threat.
A person can be bitten by a snake for several reasons. Accidental causes include
reaching or stepping without looking, not being aware of the danger, rolling over
onto a snake while sleeping, and being unaware of the presence of a snake because
of poor hearing or vision. Handling of a venomous snake by a person who is in-
experienced, careless, inattentive, overconfident, or intoxicated can also result in
a snakebite. In addition, snake envenomation may occur in an attempt to capture
or kill a snake or as part of a religious ceremony. Finally, some cases of enven-
omation are intentional (e.g., as an attempt to induce tolerance of venom or for
pleasure).5
Bites most commonly involve the extremities. Unprovoked bites are more likely
to involve females and the lower extremities. Provoked bites are more likely to
involve males and the upper extremities. The intentionality of the interaction does
not appear to be associated with the likelihood or severity of envenomation. The
continent with the lowest occurrence of snake envenomation is Europe, and the
highest occurrences are in Africa and Asia.6 In Australia, deaths from envenom-
68 n engl j med 386;1 nejm.org January 6, 2022
The New England Journal of Medicine
Downloaded from nejm.org by Nicole Iriarte Acuña on March 6, 2022. For personal use only. No other uses without permission.
Copyright © 2022 Massachusetts Medical Society. All rights reserved.
Snake Envenomation
A Viperidae B Elapidae
Primary Main venom Compressor muscle Accessory Primary Main venom Compressor muscle
Accessory duct gland venom duct gland
venom gland
gland
Secondary
duct
Secondary
duct
Discharge
aperture
Discharge
aperture
C Atractaspidinae
D Colubridae
Primary Main venom Compressor muscle Duvernoy’s gland
Accessory duct gland Main duct
venom
gland
Secondary
duct
Discharge aperture
Grooved fang
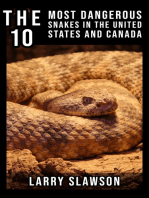
Figure 1. Venom Delivery Systems of Snakes.
All venom delivery systems involve either venom glands or, in the case of colubrids, Duvernoy’s glands, which unlike venom glands,
do not have a large reservoir of venom. Venom glands are attached to tubular fangs through a duct. In Viperidae, Elapidae, and Atracta
spidinae (Panels A, B, and C, respectively), contraction of muscles around the venom glands propels the venom into the fangs and
eventually into bitten tissue through openings near the tips. In Colubridae (Panel D), low-pressure channeling of venom into the bite
site through grooved fangs occurs. All snakes have teeth on the lower jaw for better tissue purchase.
ation are infrequent, despite the presence of snakebite-related deaths and disabilities by 2030,
many highly venomous snakes.7 Snakebites and key aspects of which include preventive efforts,
death from envenomation are most frequent in improved treatments, and enhanced access to
rural, low-income regions, where health care care.8 That program is currently in a scaling-up
often cannot be accessed quickly and antivenom phase.
and intensive supportive care might not be avail-
able. Among patients who survive, delayed or Pathoph ysiol o gy of V enomous
inadequate care can lead to permanent disability Sna k ebi te s
(e.g., amputations and blindness).
An understanding of the epidemiology of Not all bites by venomous snakes involve enven-
envenomation is useful in developing preventive omation; “dry” bites occur in 2 to 50% of cases.9
and management efforts. In 2019, the WHO When envenomation does occur, the clinical ef-
established a program to halve the number of fects depend on the toxins in the venom. Snake
n engl j med 386;1 nejm.org January 6, 2022 69
The New England Journal of Medicine
Downloaded from nejm.org by Nicole Iriarte Acuña on March 6, 2022. For personal use only. No other uses without permission.
Copyright © 2022 Massachusetts Medical Society. All rights reserved.
The n e w e ng l a n d j o u r na l of m e dic i n e
venom contains an array of toxins that can in- consumption coagulopathy are categorized ac-
duce clinical effects that can be both local and cording to where they act on the clotting cas-
systemic and range from mild to fatal, as out- cade. Some of the most relevant procoagulant
lined below. toxins, such as metalloproteinases, are activators
of prothrombin, factor V, factor X, or thrombinlike
Cytotoxicity enzymes (fibrinogenases).15 Thrombotic micro-
Local tissue injury and inflammation are caused angiopathy, which may accompany venom-
by enzymes such as hyaluronidase and collage- induced consumption coagulopathy, is character-
nase, as well as proteinases and phospholipases. ized by thrombocytopenia, microangiopathic
The results are pain and edema; edema can hemolytic anemia, and acute kidney injury.16
spread from the site of the bite and may also
lead to bullae and dermonecrosis. Local ecchy- Thrombosis
mosis may be the result of increased vascular Snake envenomation can result in myocardial
permeability, systemic coagulopathies, or both. infarction, stroke, or other thrombotic effects.
The effect of snake venom metalloproteinases Twenty-two cases of myocardial infarction after
on the extracellular matrix results in the release snake envenomation have been reported.17 Pro-
of extracellular matrix–derived peptides that ex- posed mechanisms of myocardial infarction in-
ert diverse actions in the tissue. Some of the clude hypovolemia, anaphylactic shock, coronary
peptides cause additional tissue destruction and thrombosis from procoagulant factors, a direct
others are involved in reparative actions. In ad- effect of venom on cardiomyocytes, decreased
dition, snake venom metalloproteinases may oxygen-carrying capacity, vasoconstriction, myo-
cause microvascular damage leading to hemor- cardial necrosis and hemorrhage, and microvas-
rhage,10 skeletal-muscle necrosis and lack of cular thrombin deposition. Strokes may be either
muscle restoration,11 blistering, and dermone- hemorrhagic or ischemic, but ischemic strokes
crosis,12 as well as inflammatory mediators that are more prevalent.18
account for pain, swelling, and leukocyte infil-
tration.13 Although elevated compartmental tis- Thrombocytopenia or Altered Platelet
sue pressure (due to edema in a space bounded Function
by a rigid fascia) or elevated subcutaneous tissue In severe cases of envenomation from Crotalinae
pressure (due to swelling exceeding the elastic (New World pit vipers), thrombocytopenia is
limits of the skin) may occur, the direct effects common. It can occur alone or in combination
of venom can mimic the symptoms and signs of with other coagulopathies, and the consumption
true compartment syndrome, and pressures may of platelets can contribute to the complications
be normal. associated with venom-induced consumption co-
agulopathy. Venom-induced thrombocytopenia
Lymphatic System appears to be associated with the specific venom
In snake envenomation, injury to the lymphatic composition and the quantity of venom intro-
system plays a role in the development of edema. duced with the bite. The mechanisms by which
The lymphatic system is also involved in sys- snake envenomation results in thrombocytope-
temic absorption of venom toxins from tissues. nia are unclear; suggested mechanisms include
In addition, some venom components are neu- platelet aggregation, platelet sequestration, and
tralized in the lymphatics, although the process decreased platelet production. Profound throm-
is slow and incomplete.14 bocytopenia may result in either spontaneous or
uncontrolled hemorrhage.19 In addition, platelets
Venom-Induced Consumption Coagulopathy may be inhibited or activated by various venom
Procoagulant toxins in snake venoms promote components (metalloproteinases and lectins),
consumption coagulopathy, which causes the resulting in normal platelet counts but platelet
depletion of factors in the clotting cascade and dysfunction.20
may result in either spontaneous or uncontrolled
bleeding. Venoms of different types of snakes Neurotoxicity
vary in the extent to which they affect clotting Neuromuscular paralysis is one of the leading
factors. Toxins in snake venom that promote clinical disorders due to envenomation from ela-
70 n engl j med 386;1 nejm.org January 6, 2022
The New England Journal of Medicine
Downloaded from nejm.org by Nicole Iriarte Acuña on March 6, 2022. For personal use only. No other uses without permission.
Copyright © 2022 Massachusetts Medical Society. All rights reserved.
Snake Envenomation
pids (snakes in the Elapidae family) such as naja,
bungarus, and micrurus species21 and can also
be seen with envenomation from other snake
families such as Crotalinae in the United States
and Hydrophiidae. Neurotoxic snake venoms
may contain exclusively postneuromuscular or
preneuromuscular synaptic toxins or a mixture
of the two types. Postsynaptic neurotoxins bind
to and block membrane receptors but remain
extracellular. Presynaptic neurotoxins, such as
alpha-bungarotoxin, are taken up into the pre-
synaptic membrane and impair the release of
neurotransmitters. Either type of neurotoxin
may cause a descending, flaccid paralysis
(Fig. 2) that progresses to airway compromise
and life-threatening respiratory insufficiency.22
Progressive paralysis from postsynaptic neuro-
toxins may be reversed because they remain
available to neutralization by antivenom. Pro-
gression of the paralytic effects of presynaptic
toxins may be halted by antivenom, but because
the neurotoxins are intracellular and no longer
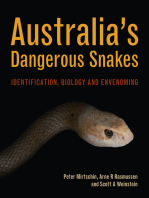
Figure 2. Neurotoxic Effects of Snake Venom.
available for neutralization, the effects are not
Neurotoxins generally cause a progressive, descending paralysis, beginning
readily reversible. Prolonged respiratory support with bulbar muscles (ptosis and dysarthria) and progressing to respiratory
may be needed once respiratory compromise has compromise.
occurred.
Myotoxicity, Cardiotoxicity, Nephrotoxicity
and Hypotension Snake envenomation can result in acute kidney
Myotoxicity may develop as a result of the di- injury, which may progress to chronic kidney
rect effect of venom on muscle through myo- disease or renal failure. A variety of snake ven-
toxic phospholipase A2, which disrupts the in- oms — including venom from bothrops species
tegrity of the plasma membrane and provokes (lancehead pit vipers), crotalus species (e.g.,
calcium influx. This process initiates a series tropical rattlesnakes), and micrurus species
of degenerative events, pressure-related effects (coral snakes) in Central and South America, as
in a muscle compartment, or inflammation well as species in Africa, such as bitis species
overlying muscle and may also directly affect (puff adders), and daboia species (Russell’s vi-
the myocardium.23 Myokymia of skeletal mus- pers) in the Asia–Pacific region — can cause
cle may result in rhabdomyolysis, respiratory nephrotoxicity through direct venom-related in-
compromise, or both. Hypotension may devel- jury mediated by inflammatory cytokines, which
op from bradykinin-potentiating peptides, na- results in glomerular degeneration and atrophy,
triuretic peptides, phospholipase A2, proteases, with deposition of proteinaceous material in
vascular endothelial growth factors, three-finger Bowman’s space.25 Nephrotoxicity as a direct ef-
toxins (a superfamily defined by a common ter- fect of venom is commonly seen with Russell’s
tiary structure consisting of three beta strand– viper envenomation.26 Mexican coral snake ven-
containing loops projecting from a small hy- om has been shown to induce oxidative stress
drophobic core containing four conserved and decrease renal perfusion and the glomeru-
disulfide bonds), and 5′ nucleotidases.24 Hypo- lar filtration rate.27 Nephrotoxicity may also
tension may reflect hypovolemia due to in- result from microangiopathy and microangio-
creased vascular permeability, loss of fluid into pathic hemolytic anemia or from rhabdomyoly-
soft tissues, myocardial depression, or anaphy- sis, altered clearance of blood degradation prod-
laxis.24 ucts, immune complexes, or from a shock state.
n engl j med 386;1 nejm.org January 6, 2022 71
The New England Journal of Medicine
Downloaded from nejm.org by Nicole Iriarte Acuña on March 6, 2022. For personal use only. No other uses without permission.
Copyright © 2022 Massachusetts Medical Society. All rights reserved.
The n e w e ng l a n d j o u r na l of m e dic i n e
tion to venom components, either from previous
A Initial Bite
envenomation or from the handling of venom-
Break in the skin ous snakes.
Di agnosis
A snakebite or envenomation may not be recog-
nized because of factors pertaining to the pa-
tient or the bite. Only one fang may have
B Pain, Swelling, and Progressive Edema achieved penetration, the punctures may be ob-
scured by edema, or an abrasion may be the only
Edema finding28 (Fig. 3). Although venom does not
Leading edge
cross intact skin or mucous membranes or usu-
ally cause injury if swallowed, it may cause oph-
thalmic injury.29 The distance between fangs
may indicate the size of the snake, with larger
snakes potentially containing larger venom
C Blisters and Ecchymosis loads, but the amount of venom injected can
vary. The degree of toxicity also may be related
Ecchymosis Blisters to the specific venom components, which are a
function of the genetic and epigenetic factors of
the snake. Children pose a particular diagnostic
challenge, since they may not be able to relate
the relevant history. Context and specific find-
ings may provide clues to the diagnosis. For
example, snake envenomation may be the cause
of otherwise unexplained coagulopathy, neuropa-
D Fasciotomy
thy, or abdominal pain (e.g., in the case of krait
Fasciotomy
(disfiguring procedure without [bungarus species] envenomation).28
demonstrated benefit) In Australia, venom detection kits consisting
of enzyme immunoassays30 are available for
identifying a snake envenomation and the spe-
cies of snake. However, in the rest of the world,
in the absence of observation of the bite and
accurate identification of the biting species, the
patient’s presentation, the appearance of the
wound, and the clinical course may be the basis
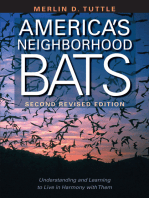
Figure 3. Clinical Appearance, Assessment, and Management of Snakebites. for diagnosing envenomation and identifying the
After a snakebite, a break in the skin is usually seen. This may be a scratch, likely snake species. Species-specific, polyvalent,
a single or double puncture, or multiple punctures. Teeth in the lower jaw or paraspecific antivenoms may be needed. In
may also produce multiple, linear punctures (Panel A). Pain, swelling, and
progressive edema with a leading edge may be seen with cytotoxic venoms,
instances in which snake families, genera, or
a finding that may be more tactile than visual (Panel B). Blisters may form species overlap, identification of the envenomat-
at the bite site and elsewhere on the bitten extremity, and ecchymosis and ing snake may be difficult, and in cases in
bruising may occur as a result of coagulopathy (Panel C). Fasciotomy is a which various antivenoms may be available, im-
disfiguring procedure without a demonstrated benefit (Panel D). proper identification sometimes results in incor-
rect management.31 Nonnative, captive snakes
may pose challenges to species identification
Other Effects and case management. The prehospital applica-
Other systemic effects of venom can include tion of ineffective and possibly harmful thera-
nausea, vomiting, diarrhea, and diaphoresis. A pies, plus any delay in obtaining competent and
complex regional pain syndrome may develop, definitive care, may also complicate both diag-
and anaphylaxis may result from prior sensitiza- nosis and management.
72 n engl j med 386;1 nejm.org January 6, 2022
The New England Journal of Medicine
Downloaded from nejm.org by Nicole Iriarte Acuña on March 6, 2022. For personal use only. No other uses without permission.
Copyright © 2022 Massachusetts Medical Society. All rights reserved.
Snake Envenomation
Cl inic a l S y ndrome s are trained in its application), or a blood pres-
sure cuff placed proximal to the bite and inflated
In geographic regions where multiple families, to sufficient pressure (approximately 50 mm Hg
genera, and species overlap, distinguishing [upper extremity] or 70 mm Hg [lower extrem-
among snake taxa may be advantageous for ity]) may be considered if there are minimal or
selection of a specific antivenom. However, the no local effects of envenomation and if there is
division of snake envenomation into distinct concern about the possibility of a rapid onset of
syndromes (e.g., neurologic, cytotoxic, and coag- neurotoxicity. Other prehospital interventions,
ulopathic) that are species-specific is simplistic. such as the use of arterial or venous tourniquets,
Envenomation syndromes may vary widely among incision, suction, heat, cold, electricity, and folk
different species within a geographic region, treatments, delay access to definitive treatment
and identification of a specific snake on the and may result in additional trauma.
basis of envenomation effects may not be pos-
sible. Although venoms can derive from diverse Hospi ta l C a r e
genetic forebears, their effects may have many
clinical similarities. Conversely, venoms from Management of snake envenomation comprises
within a family, genus, or species may have sub- the administration of antivenom (if available),
stantially different clinical effects as a result other specific local and systemic treatments,
of snake venomics, variable gene expression, and symptomatic and supportive care. Manage-
and epigenetic factors.32 As examples, myotoxic- ment approaches generally have poor scientific
ity and neurotoxicity are typically seen in elapid bases, however, with systematic reviews provid-
envenomation but also occur in Crotalinae en- ing critically low confidence for most interven-
venomation in Central and South America.33 tions and conflicting findings about specific
Some Mojave rattlesnakes (Crotalus scutulatus) antivenoms.39,40 In the absence of high-quality
contain large amounts of Mojave toxin, a potent data for management decisions, consensus guide-
neurotoxin, whereas others have none at all.34 lines and expert opinion predominate, some-
Even in the same snake, different venom effects times with differing recommendations.39,41-43
are the result of ontogenic changes expressed Once the patient has arrived at a health care
over time, from newborn, to juvenile, to adult.35 facility, vital signs should be obtained and
Thus, knowledge of the family, genus, and spe- monitored. Restrictive clothing and clothing
cies of an envenomating snake may not allow covering the wound should be removed, the pa-
accurate prediction of the likelihood of venom- tient examined, and an intravenous catheter
induced toxic effects.36 placed. Tetanus status should be updated as
needed, and the wound (or wounds) should be
cleaned and inspected for retained foreign bod-
Pr ehospi ta l C a r e
ies (e.g., fangs or teeth).41 Ultrasonography may
Because of the wide variety of presentations and show retained fangs or teeth, as well as the loca-
management challenges, expert assistance should tion of edema.44 If the bite does not appear to
be sought early. The primary priorities of the contain venom, the patient should be observed
prehospital assessment and management of for a long enough period to confirm that enven-
snakebite are, first, to get away from the snake omation has not occurred. The duration of ob-
and identify it, if possible; second, to loosely servation varies according to snake taxa and
splint the bitten body part, with a default of geographic factors, but periods between 6 and
heart-neutral positioning37; third, to anticipate 24 hours have been suggested.41,45
swelling (e.g., remove jewelry); and finally, to Studies have shown that antivenoms are a
obtain transport (with personnel competent in definitive treatment, and these agents are be-
advanced life support) to a capable health care lieved to be responsible for reducing the morbid-
facility. Because the majority of venom enters the ity and mortality associated with envenomation.
circulation through the lymphatics,38 impairing Early evidence of efficacy was based on an in-
lymphatic flow may slow the systemic effects crease in the survival rate or survival time in
of the venom. A compressive bandage, wrapped crude animal models, on retrospective clinical
from distal to proximal extremity (if personnel data showing reduced mortality after antivenom
n engl j med 386;1 nejm.org January 6, 2022 73
The New England Journal of Medicine
Downloaded from nejm.org by Nicole Iriarte Acuña on March 6, 2022. For personal use only. No other uses without permission.
Copyright © 2022 Massachusetts Medical Society. All rights reserved.
The n e w e ng l a n d j o u r na l of m e dic i n e
A Mammalian IgG B Pepsin Cleave Antigen
Antigen
Heavy chain
F(ab')2
Fab domain fragment
Hinge Antigen
binding site
Light chain
C Papain Cleave
Fc domain Heavy chain Fab
fragments
Fc remnant
Constant region
Variable region
Figure 4. IgG and IgG Fragments Developed against Snake Venom Components.
The mammalian IgG molecule (Panel A) consists of an Fc (heavy) chain, a hinge, and two Fab (light) chains. The light chains have con-
stant and variable regions, which allow the IgG to bind to certain antigens (Ag), such as venom components. When the IgG is treated
with pepsin, the IgG molecule is cleaved below the hinge (comprising two disulfide bridges), and an F(ab′)2 fragment is produced (Panel B).
When the IgG is treated with papain, the cleavage occurs above the hinge, and two Fab fragments are produced (Panel C). The Fc remnant
or chain, which is more immunogenic than the Fab chains, can be removed from the remaining solution by means of various purification
techniques.
administration, and on suggestive individual dose is selected to arrest or reverse the immedi-
case reports and case series.46 More recently, ate effects of the venom, with subsequent adjust-
sophisticated in vitro and animal models, as ment according to the response to the initial
well as prospective clinical studies, have con- dose. Because the venom load may be as large in
firmed a reduction in morbidity and mortality a child as in an adult, children require at least
with the use of antivenoms.46,47 the same amount of antivenom as adults. Chil-
Antivenom antibodies — IgG, F(ab′)2, or Fab dren may need larger amounts initially, since
fragments — (Fig. 4) that have been developed their smaller vascular volume can result in an in-
in a source animal (e.g., horse or sheep) neutral- creased concentration of circulating venoms. In
ize antigenic components of venom that they addition, children may require more concentrated
encounter in circulation or in tissue, although antivenom to reduce infused fluid volumes.
edema or venom sequestration in lymphatics Pregnant women also constitute a special sub-
may limit the presence of venom components in group of patients with envenomation. Fetal loss
tissue. The efficacy and adverse-effect profiles may occur, particularly if the bite occurs before
of antivenoms depend on the source animal, type 20 weeks of gestation, but most envenomations
and degree of purification, specific antibody have minor or no effects and good outcomes.
fraction, host, and other factors. Smaller anti- Although no studies have evaluated antivenom
body fragments (e.g., Fab) have larger volumes safety during pregnancy, antivenom is generally
of distribution and shorter half-lives than larger used for the same indications in pregnant pa-
fragments.48 tients as in nonpregnant patients, with no re-
Because the neutralizing power per vial var- ports of adverse reactions.49
ies, antivenoms are dosed by the vial. Since nei- Since unneutralized venom may remain in
ther the total venom load nor the load of spe- tissues and continue to have local and systemic
cific components is known, the initial antivenom effects, antivenom may need to be readminis-
74 n engl j med 386;1 nejm.org January 6, 2022
The New England Journal of Medicine
Downloaded from nejm.org by Nicole Iriarte Acuña on March 6, 2022. For personal use only. No other uses without permission.
Copyright © 2022 Massachusetts Medical Society. All rights reserved.
Snake Envenomation
tered to align venom and antivenom kinetics produced; further purification techniques; and
within the first 24 hours for local effects and in host factors. Skin testing before administration
a period of days to weeks for systemic effects.48,50 is discouraged because the results are insuffi-
Some venom-induced effects may not be easily ciently sensitive to be of value or may be subject
reversed or may result in long-term or perma- to misinterpretation,58 but pretreatment with
nent injury. Thus, once envenomation has been epinephrine may be recommended for certain
confirmed, early administration of antivenom is antivenoms with high rates of type 1 hypersen-
indicated. sitivity (anaphylactic) reactions.59 When a choice
Information regarding antivenoms for spe- of antivenom is available, the selection is based
cific snakes can most reliably be found at a re- on safety, kinetic factors, cost, and whether
gional poison center. A WHO database is avail- monovalent or polyvalent antivenom is more ap-
able online.51 The Clinical Toxinology Resources propriate, as well as other considerations.
website, based at the University of Adelaide,
contains detailed information on envenomations Org a n-S ys tem –B a sed A sse ssmen t
and antivenoms worldwide.52 The online Anti- a nd M a nagemen t
venom Index includes the package inserts of many
antivenoms, with their manufacturer-attributed Cytotoxicity
indications and their locations at zoos in the Cytotoxicity may serve as an indication for anti-
United States.53 When envenomation from an venom, and the earliest appropriate use of anti-
indigenous snake has occurred, local health care venom is associated with the best outcomes.60,61
facilities either stock or should know how to During antivenom infusion, the bitten body part
obtain an appropriate antivenom. Because of the should be elevated. Opioid-level pain control
large crossover of venom constituents across may be needed; however, antivenom treatment
species and genera, an antivenom developed for of envenomation from a copperhead snake
a small subset of snake species may treat a large (Agkistrodon contortrix) has been shown to reduce
variety of regional snakes.54 For nonnative snakes, the use of opioids.62 When tissue pressures are
different systems exist, including centralized suspected to be elevated, appropriate assess-
antivenom depots,55 zoo-based sources,56 and ments include ultrasonography, magnetic reso-
online resources.53,56 If a poison center network nance imaging, direct measurement of tissue
is available, associated toxicologists will proba- and compartment pressures, or a combination of
bly know how to source appropriate antivenoms these approaches.44 Increased pressures, either in
in a timely manner. Package inserts may provide deep compartments or in subcutaneous tissue,
appropriate dosing information. However, since should be considered indications for additional
the information may be outdated or may not antivenom, elevation of the bitten body part (be-
conform to current practices, expert guidance cause most if not all edema is located in the
should be sought. subcutaneous space and is amenable to gravity-
Antivenoms are not available for bites from assisted lymphatic drainage), and possibly man-
certain venomous snakes, such as Thelotornis nitol. Fasciotomy has not been shown to im-
capensis (one of the twig snakes) and the Atracta prove outcomes, as compared with antivenom
spidinae (burrowing asps, mole vipers, and sti- and elevation alone or with fasciotomy plus
letto snakes). This lack of availability has re- antivenom.63 Prophylactic antibiotics to prevent
sulted in substantial morbidity and mortality. infection have not proved useful. Necrosis is a
Even when antivenoms do exist, they may be too known risk factor for infection and may be an
expensive for local health care use, may not be indication for antibiotic use.64
available in the geographic region where they
are needed, or may not be currently available Hemotoxicity
from the manufacturer.57 In some cases of venom-induced consumption
The risk of hypersensitivity reactions to anti- coagulopathy, antivenom has been effective,
venoms ranges from very low to high (type 1, or although the rate and degree of improvement
acute), generally depending on the source ani- varies. Heparin is ineffective.15 Either bleeding
mal; whether an IgG, F(ab′)2, or Fab fragment is or thrombosis with infarction may be seen with
n engl j med 386;1 nejm.org January 6, 2022 75
The New England Journal of Medicine
Downloaded from nejm.org by Nicole Iriarte Acuña on March 6, 2022. For personal use only. No other uses without permission.
Copyright © 2022 Massachusetts Medical Society. All rights reserved.
The n e w e ng l a n d j o u r na l of m e dic i n e
venom-induced consumption coagulopathy.65 are characterized by rapidly falling serum con-
Standard testing includes a platelet count, pro- centrations and are cleared more quickly from
thrombin time and international normalized the body, conferring a predisposition to recur-
ratio, activated partial-thromboplastin time, fi- rent venom effects and making F(ab′)2 antiven-
brinogen level, and d-dimer level (as a marker oms the current standard.48 However, the price
of fibrinogenolysis), as well as the 20-minute of antivenoms may render their use impossible
whole-blood clotting test.66 Thromboelastogra- in many developing countries. Investigations are
phy provides information that is similar to that therefore exploring the efficacy of making anti-
provided by standard laboratory assays, although bodies in other animals (e.g., camels, chick-
it may be useful in anticipation of hypofibrino- ens, and sharks) or humanizing animal anti-
genemia.67 Hematologic effects may persist for bodies.
several days to more than 2 weeks68 and may
respond less well to late administration of anti- Natural Venom Inhibitors
venom or may require periodic or continued Many animal serums and some plant extracts
infusion of antivenom.69 Blood products can be can neutralize snake venom.71 For instance,
given, if needed, but should be administered LTNF-11, a peptide derived from the American
simultaneously with additional antivenom.41 opossum (Didelphis virginiana), inhibits the lethal-
ity of hemorrhagic snake venoms.72 With further
Myotoxicity development, such inhibitors may be useful as
Myokymia may result in rhabdomyolysis, respira- alternative or supplemental treatments.
tory compromise, or both. Antivenom treatment
targets direct myotoxic effects. Rhabdomyolysis Synthetic Peptides, Phospholipase A2
is managed according to standard protocols. Inhibitors, and Metalloproteinase Inhibitors
Some synthetic peptides and secretory phospho-
Nephrotoxicity lipase A2 inhibitors that have the ability to
It is appropriate to screen for nephrotoxicity in neutralize snake venoms are promising. Vares-
all cases of envenomation. Antivenom against pladib, originally designed to treat acute chest
Russell’s viper has been shown to reduce renal syndrome, has inhibitory effects on secretory
injury,26 and appropriate antivenom therapy phospholipase A2 and may be of value against a
should be considered in any case of renal injury. broad spectrum of snake venoms. Batimastat
and marimastat are matrix metalloproteinase
Neurotoxicity inhibitors that have been shown to inhibit some
Antivenom treatment is most effective against of the coagulopathies caused by hemorrhagic
postsynaptic venoms, and early administration venoms.73 Other inhibiting peptides are the nucle-
is important for presynaptic venoms, while they otide-based and amino acid–based aptamers and
are still extracellular. Airway management is X-aptamers, which can be made toxin-specific,
based on the same principles that guide the especially against small-molecule venom toxins
management of other conditions involving respi- that may not be immunogenic.74
ratory compromise.
C onclusions
F u t ur e Dir ec t ions
Snakebite envenomation continues to be a major
Antibody-Based Antivenoms global health burden. Current technical advances
Antivenoms made in horses or sheep are cur- are focused on snake envenomation treatments,
rently the only effective treatment for snake en- including more effective and safer antivenoms.
venomation. IgG-based or incompletely purified Current efforts aimed at prevention, diagnosis,
antivenoms may be more likely than others to and increased access to timely and effective
produce type 1 reactions (anaphylaxis), type 3 treatments are still in early stages of develop-
reactions (serum sickness), or both, with only ment in much of the world.
about 30% of the immunoglobulins directed Disclosure forms provided by the authors are available with
toward the actual snake toxins.70 Fab antivenoms the full text of this article at NEJM.org.
76 n engl j med 386;1 nejm.org January 6, 2022
The New England Journal of Medicine
Downloaded from nejm.org by Nicole Iriarte Acuña on March 6, 2022. For personal use only. No other uses without permission.
Copyright © 2022 Massachusetts Medical Society. All rights reserved.
Snake Envenomation
References
1. Chippaux JP. Snakebite envenomation 15. Maduwage K, Isbister GK. Current 29. Tsai TH, Lin CC, Mao YC, et al. Naja
turns again into a neglected tropical dis- treatment for venom-induced consump- atra venom-spit ophthalmia in Taiwan:
ease! J Venom Anim Toxins Incl Trop Dis tion coagulopathy resulting from snake- an epidemiological survey from 1990 to
2017;23:38. bite. PLoS Negl Trop Dis 2014;8(10):e3220. 2016. J Chin Med Assoc 2020;83:77-83.
2. GBD 2017 Causes of Death Collabora- 16. Isbister GK. Snakebite doesn’t cause 30. Johnston CI, Ryan NM, Page CB, et al.
tors. Global, regional, and national age- disseminated intravascular coagulation: The Australian Snakebite Project, 2005–
sex-specific mortality for 282 causes of coagulopathy and thrombotic microan- 2015 (ASP-20). Med J Aust 2017;207:119-
death in 195 countries and territories, giopathy in snake envenoming. Semin 25.
1980-2017: a systematic analysis for the Thromb Hemost 2010;36:444-51. 31. Bolon I, Durso AM, Botero Mesa S,
Global Burden of Disease Study 2017. 17. Kariyanna PT, Jayarangaiah A, Kam- et al. Identifying the snake: first scoping
Lancet 2018;392:1736-88. ran H, et al. Myocardial infarction after review on practices of communities and
3. Longbottom J, Shearer FM, Devine M, snakebite envenomation: a scoping study. healthcare providers confronted with
et al. Vulnerability to snakebite envenom- Scifed J Cardiol 2018;2:21. snakebite across the world. PLoS One
ing: a global mapping of hotspots. Lancet 18. Al-Sadawi M, Mohamadpour M, 2020;15(3):e0229989.
2018;392:673-84. Zhyvotovska A, et al. Cerebrovascular ac- 32. Ali AJ, Horwitz DA, Mullins ME. Lack
4. Warrell DA. Bites of venomous snakes. cident and snake envenomation: a scop- of coagulopathy after copperhead snake-
N Engl J Med 2002;347:1804-5. ing study. Int J Clin Res Trials 2019;4:133. bites. Ann Emerg Med 2015;65:404-9.
5. Senthilkumaran S, Shah S, Balamuru- 19. Oliveira SS, Alves EC, Santos AS, et al. 33. Keyler DE, Saini V, O’Shea M, Gee J,
gan N, Menezes RG, Thirumalaikolundu- Bleeding disorders in Bothrops atrox enven- Smith CF, Mackessy SP. Crotalus orega-
subramanian P. Repeated snake bite for omations in the Brazilian Amazon: par- nus concolor: envenomation case with
recreation: mechanisms and implications. ticipation of hemostatic factors and the venom analysis and a diagnostic conun-
Int J Crit Illn Inj Sci 2013;3:214-6. impact of tissue factor. Toxins (Basel) drum of myoneurologic symptoms. Wil-
6. Chippaux JP. Snake-bites: appraisal of 2020;12:554. derness Environ Med 2020;31:220-5.
the global situation. Bull World Health 20. Clemetson KJ. Snaclecs (snake C-type 34. Massey DJ, Calvete JJ, Sánchez EE, et al.
Organ 1998;76:515-24. lectins) that inhibit or activate platelets by Venom variability and envenoming sever-
7. Welton RE, Liew D, Braitberg G. Inci- binding to receptors. Toxicon 2010;56: ity outcomes of the Crotalus scutulatus
dence of fatal snake bite in Australia: 1236-46. scutulatus (Mojave rattlesnake) from
a coronial based retrospective study (2000– 21. Silva A, Maduwage K, Sedgwick M, southern Arizona. J Proteomics 2012;75:
2016). Toxicon 2017;131:11-5. et al. Neuromuscular effects of common 2576-87.
8. Minghui R, Malecela MN, Cooke E, krait (Bungarus caeruleus) envenoming in 35. Lomonte B, Fernández J, Sanz L, et al.
Abela-Ridder B. WHO’s Snakebite Enven- Sri Lanka. PLoS Negl Trop Dis 2016;10(2): Venomous snakes of Costa Rica: biologi-
oming Strategy for prevention and con- e0004368. cal and medical implications of their ven-
trol. Lancet Glob Health 2019;7(7):e837- 22. Harris JB, Scott-Davey T. Secreted phos- om proteomic profiles analyzed through
e838. pholipases A2 of snake venoms: effects the strategy of snake venomics. J Pro-
9. Pucca MB, Knudsen C, S Oliveira I, et al. on the peripheral neuromuscular system teomics 2014;105:323-39.
Current knowledge on snake dry bites. with comments on the role of phospholi- 36. Casewell NR, Jackson TNW, Laustsen
Toxins (Basel) 2020;12:668. pases A2 in disorders of the CNS and AH, Sunagar K. Causes and consequences
10. Escalante T, Ortiz N, Rucavado A, et al. their uses in industry. Toxins (Basel) of snake venom variation. Trends Phar-
Role of collagens and perlecan in micro- 2013;5:2533-71. macol Sci 2020;41:570-81.
vascular stability: exploring the mecha- 23. Reis LPG, Botelho AFM, Novais CR, 37. Seifert S, White J, Currie BJ. Pressure
nism of capillary vessel damage by snake et al. Cardiotoxic effects of Micrurus suri- bandaging for North American snake bite?
venom metalloproteinases. PLoS One 2011; namensis (Cuvier, 1817) snake venom. No! Clin Toxicol (Phila) 2011;49:883-5.
6(12):e28017. Cardiovasc Toxicol 2021;21:462-71. 38. Vergara I, Castillo EY, Romero-Piña
11. Hernández R, Cabalceta C, Saravia- 24. Péterfi O, Boda F, Szabó Z, Ferencz E, ME, et al. Biodistribution and lymphatic
Otten P, Chaves A, Gutiérrez JM, Ruca- Bába L. Hypotensive snake venom compo- tracking of the main neurotoxin of Micru-
vado A. Poor regenerative outcome after nents — a mini-review. Molecules 2019; rus fulvius venom by molecular imaging.
skeletal muscle necrosis induced by Bo- 24:2778. Toxins (Basel) 2016;8:85.
throps asper venom: alterations in micro- 25. Marinho AD, Silveira JAM, Chaves 39. Bhaumik S, Beri D, Lassi ZS, Jagnoor J.
vasculature and nerves. PLoS One 2011; Filho AJM, et al. Bothrops pauloensis Interventions for the management of snake-
6(5):e19834. snake venom-derived Asp-49 and Lys-49 bite envenoming: an overview of system-
12. Jiménez N, Escalante T, Gutiérrez JM, phospholipases A2 mediates acute kidney atic reviews. PLoS Negl Trop Dis 2020;
Rucavado A. Skin pathology induced by injury by oxidative stress and release of 14(10):e0008727.
snake venom metalloproteinase: acute inflammatory cytokines. Toxicon 2021; 40. Noutsos T, Currie BJ, Lek RA, Isbister
damage, revascularization, and re-epithe- 190:31-8. GK. Snakebite associated thrombotic mi-
lization in a mouse ear model. J Invest 26. Hung DZ, Yu YJ, Hsu CL, Lin TJ. Anti- croangiopathy: a systematic review of clin-
Dermatol 2008;128:2421-8. venom treatment and renal dysfunction in ical features, outcomes, and evidence for
13. Fernandes CM, Pereira Teixeira CF, Russell’s viper snakebite in Taiwan: a case interventions including plasmapheresis.
Leite AC, Gutiérrez JM, Rocha FA. The series. Trans R Soc Trop Med Hyg 2006; PLoS Negl Trop Dis 2020;14(12):e0008936.
snake venom metalloproteinase BaP1 in- 100:489-94. 41. Lavonas EJ, Ruha AM, Banner W, et al.
duces joint hypernociception through 27. Braga JRM, Jorge ARC, Marinho AD, Unified treatment algorithm for the man-
TNF-alpha and PGE2-dependent mecha- et al. Renal effects of venoms of Mexican agement of crotaline snakebite in the
nisms. Br J Pharmacol 2007;151:1254-61. coral snakes Micrurus browni and Micru- United States: results of an evidence-in-
14. Paniagua D, Vergara I, Román R, et al. rus laticollaris. Toxicon 2020;181:45-52. formed consensus workshop. BMC Emerg
Antivenom effect on lymphatic absorp- 28. Le Geyt J, Pach S, Gutiérrez JM, et al. Med 2011;11:2.
tion and pharmacokinetics of coral snake Paediatric snakebite envenoming: recog- 42. Di Nicola MR, Pontara A, Kass GEN,
venom using a large animal model. Clin nition and management of cases. Arch et al. Vipers of major clinical relevance in
Toxicol (Phila) 2019;57:727-34. Dis Child 2021;106:14-9. Europe: taxonomy, venom composition,
n engl j med 386;1 nejm.org January 6, 2022 77
The New England Journal of Medicine
Downloaded from nejm.org by Nicole Iriarte Acuña on March 6, 2022. For personal use only. No other uses without permission.
Copyright © 2022 Massachusetts Medical Society. All rights reserved.
Snake Envenomation
toxicology and clinical management of hu- 54. Pla D, Quesada-Bernat S, Rodríguez Y, a cobra BITE study. Toxins (Basel) 2021;
man bites. Toxicology 2021;453:152724. et al. Dagestan blunt-nosed viper, Macro- 13:183.
43. Turner D, Winter S, Winkel K, MacIsaac vipera lebetina obtusa (Dwigubsky, 1832), 65. Zeng X, Hu J, Liang X, et al. Acute ce-
C, Padula A, Braitberg G. Review article: venom. Venomics, antivenomics, and neu- rebral infarction following a Trimeresu-
let us talk about snakebite management: tralization assays of the lethal and toxic rus stejnegeri snakebite: a case report.
a discussion on many levels. Emerg Med venom activities by anti-Macrovipera leb- Medicine (Baltimore) 2019;98(23):e15684.
Australas 2019;31:542-5. etina turanica and anti-Vipera berus berus anti- 66. Ratnayake I, Shihana F, Dissanayake
44. Wood D, Sartorius B, Hift R. Ultra- venoms. Toxicon X 2020;6:100035. DM, Buckley NA, Maduwage K, Isbister
sound findings in 42 patients with cyto- 55. de Haro L. Management of snakebites GK. Performance of the 20-minute whole
toxic tissue damage following bites by in France. Toxicon 2012;60:712-8. blood clotting test in detecting venom in-
South African snakes. Emerg Med J 2016; 56. Warrick BJ, Boyer LV, Seifert SA. Non- duced consumption coagulopathy from
33:477-81. native (exotic) snake envenomations in Russell’s viper (Daboia russelii) bites.
45. Hughes A. Observation of snakebite the U.S., 2005–2011. Toxins (Basel) 2014; Thromb Haemost 2017;117:500-7.
victims: is twelve hours still necessary? 6:2899-911. 67. Leffers P, Ferreira J, Sollee D, Schauben
Emerg Med (Fremantle) 2003;15:511-7. 57. Habib AG, Musa BM, Iliyasu G, Hamza J. Thromboelastography in the manage-
46. Dart RC, McNally J. Efficacy, safety, M, Kuznik A, Chippaux JP. Challenges and ment of snakebite-induced coagulopathy:
and use of snake antivenoms in the prospects of snake antivenom supply in a case series and literature review. Blood
United States. Ann Emerg Med 2001;37: sub-Saharan Africa. PLoS Negl Trop Dis Coagul Fibrinolysis 2018;29:656-60.
181-8. 2020;14(8):e0008374. 68. Seifert SA, Kirschner RI, Martin N.
47. Bush SP, Ruha AM, Seifert SA, et al. 58. Chuang PC, Chang KW, Cheng FJ, Wu Recurrent, persistent, or late, new-onset
Comparison of F(ab′)2 versus Fab anti MH, Tsai MT, Li CJ. Risk factors associ- hematologic abnormalities in Crotaline
venom for pit viper envenomation: a pro- ated with snake antivenom reaction and snakebite. Clin Toxicol (Phila) 2011;49:
spective, blinded, multicenter, random- the role of skin test. Acta Trop 2020;203: 324-9.
ized clinical trial. Clin Toxicol (Phila) 105293. 69. Bush SP, Seifert SA, Oakes J, et al.
2015;53:37-45. 59. Habib AG. Effect of pre-medication Continuous IV Crotalidae polyvalent im-
48. Seifert SA, Boyer LV. Recurrence phe- on early adverse reactions following anti- mune Fab (ovine) (FabAV) for selected
nomena after immunoglobulin therapy for venom use in snakebite: a systematic re- North American rattlesnake bite patients.
snake envenomations. 1. Pharmacokinet- view and meta-analysis. Drug Saf 2011; Toxicon 2013;69:29-37.
ics and pharmacodynamics of immuno- 34:869-80. 70. Laustsen AH. Guiding recombinant
globulin antivenoms and related antibod- 60. Chuang PC, Chang KW, Cheng SY, et al. antivenom development by omics technol-
ies. Ann Emerg Med 2001;37:189-95. Benefits of early in-hospital antivenom ogies. N Biotechnol 2018;45:19-27.
49. Ramirez-Cruz MP, Smolinske SC, administration to patients with Protobo- 71. Sánchez EE, Rodríguez-Acosta A. In-
Warrick BJ, Rayburn WF, Seifert SA. En- throps mucrosquamatus envenomation. Am J hibitors of snake venoms and develop-
venomations during pregnancy reported Trop Med Hyg 2021;104:323-8. ment of new therapeutics. Immunophar-
to the national poison data system, 2009– 61. Anderson VE, Gerardo CJ, Rapp-Olsson macol Immunotoxicol 2008;30:647-78.
2018. Toxicon 2020;186:78-82. M, et al. Early administration of Fab anti- 72. Komives CF, Sanchez EE, Rathore AS,
50. Seifert SA, Mascarenas DN, Fullerton venom resulted in faster limb recovery in et al. Opossum peptide that can neutralize
L, Warrick BJ, Smolinske SC. Unpredicted copperhead snake envenomation patients. rattlesnake venom is expressed in Esche-
late-, new-onset thrombocytopenia and Clin Toxicol (Phila) 2019;57:25-30. richia coli. Biotechnol Prog 2017;33:81-6.
hypofibrinogenemia in Fab antivenom- 62. Freiermuth CE, Lavonas EJ, Anderson 73. Arias AS, Rucavado A, Gutiérrez JM.
treated rattlesnake envenomation. Toxicon VE, et al. Antivenom treatment is associ- Peptidomimetic hydroxamate metallopro-
2020;184:55-6. ated with fewer patients using opioids af- teinase inhibitors abrogate local and sys-
51. World Health Organization. Snake- ter copperhead envenomation. West J Emerg temic toxicity induced by Echis ocellatus
bite (https://www.who.int/health-topics/ Med 2019;20:497-505. (saw-scaled) snake venom. Toxicon 2017;
snakebite#tab=t ab_1). 63. Cumpston KL. Is there a role for fasci- 132:40-9.
52. University of Adelaide. Clinical toxinol- otomy in Crotalinae envenomations in 74. Lauridsen LH, Shamaileh HA, Ed-
ogy resources, 2018 (http://www.toxinology North America? Clin Toxicol (Phila) 2011; wards SL, Taran E, Veedu RN. Rapid one-
.com). 49:351-65. step selection method for generating
53. Association of Zoos and Aquariums. 64. Yeh H, Gao SY, Lin CC. Wound infec- nucleic acid aptamers: development of
Antivenom index. University of Arizona tions from Taiwan cobra (Naja atra) bites: a DNA aptamer against α-bungarotoxin.
(https://avi.pharmacy.a rizona.edu/a/ determining bacteriology, antibiotic sus- PLoS One 2012;7(7):e41702.
index#top). ceptibility, and the use of antibiotics — Copyright © 2022 Massachusetts Medical Society.
78 n engl j med 386;1 nejm.org January 6, 2022
The New England Journal of Medicine
Downloaded from nejm.org by Nicole Iriarte Acuña on March 6, 2022. For personal use only. No other uses without permission.
Copyright © 2022 Massachusetts Medical Society. All rights reserved.
You might also like
- Nej MR A 2105228Document11 pagesNej MR A 2105228noel romeroNo ratings yet
- Primeros Auxilios MordeduraDocument5 pagesPrimeros Auxilios MordeduraJavier MartinezNo ratings yet
- Envenomations: Wonder Abotsi, PHDDocument123 pagesEnvenomations: Wonder Abotsi, PHDKofi Frimpong-Manson100% (1)
- The Bite That HealsDocument11 pagesThe Bite That Healshằng nguyễnNo ratings yet
- Literature Review of Snake BiteDocument5 pagesLiterature Review of Snake Bitec5p6e5z1No ratings yet
- The Bite That HeatDocument4 pagesThe Bite That HeatLâm Khánh TrangNo ratings yet
- Gan 2002Document14 pagesGan 2002Muhammad ArifinNo ratings yet
- Gan 2002Document14 pagesGan 2002Muhammad ArifinNo ratings yet
- Thesis Topics On Snake BiteDocument4 pagesThesis Topics On Snake Biteshannonsandbillings100% (2)
- Snake BiteDocument23 pagesSnake BiteAndika MetrisiawanNo ratings yet
- (A Golden Guide) Venomous AnimalsDocument164 pages(A Golden Guide) Venomous AnimalsDoloma50% (2)
- Ilovepdf Merged 17Document148 pagesIlovepdf Merged 17FournierNo ratings yet
- Snake Bite Management FinalDocument88 pagesSnake Bite Management Finalimprema8No ratings yet
- Bitten: True Medical Stories of Bites and StingsFrom EverandBitten: True Medical Stories of Bites and StingsRating: 4 out of 5 stars4/5 (44)
- Pin WormDocument6 pagesPin WormAbang SupriantoNo ratings yet
- Objectives:: Pediculus Humanus Capitis Female, Pediculus Humanus Capitis Male, Cimex LectulariusDocument13 pagesObjectives:: Pediculus Humanus Capitis Female, Pediculus Humanus Capitis Male, Cimex LectulariusRaymond Martin CorpusNo ratings yet
- The Global Epidemiology, Syndromic Classification, Management, and Prevention of Spider BitesDocument12 pagesThe Global Epidemiology, Syndromic Classification, Management, and Prevention of Spider BitesIstianaNo ratings yet
- Venom Antivenom and ImmunityDocument80 pagesVenom Antivenom and ImmunityAris DedovićNo ratings yet
- The War Within Us: Everyman's Guide to Infection and ImmunityFrom EverandThe War Within Us: Everyman's Guide to Infection and ImmunityNo ratings yet
- Arthropods 121228103317 Phpapp02Document110 pagesArthropods 121228103317 Phpapp02Purwaningtyas KusumaningsihNo ratings yet
- 39 HelminthiasisDocument87 pages39 HelminthiasisArlini Nurul YuliantiNo ratings yet
- The Very Hungry Parasite: It's Not What You're Eating, It's What's Eating YouFrom EverandThe Very Hungry Parasite: It's Not What You're Eating, It's What's Eating YouNo ratings yet
- The Deadly Mosquito: The Diseases These Tiny Insects Carry - Health Book for Kids | Children's Diseases BooksFrom EverandThe Deadly Mosquito: The Diseases These Tiny Insects Carry - Health Book for Kids | Children's Diseases BooksNo ratings yet
- Management Insect BitesDocument1 pageManagement Insect BitesPujiana ashariNo ratings yet
- “Venomous Bites from Non-Venomous Snakes: A Critical Analysis of Risk and Management of “Colubrid Snake BitesFrom Everand“Venomous Bites from Non-Venomous Snakes: A Critical Analysis of Risk and Management of “Colubrid Snake BitesNo ratings yet
- Snake Bite PubmedDocument19 pagesSnake Bite PubmedMade Ayu IntanNo ratings yet
- Australia's Dangerous Snakes: Identification, Biology and EnvenomingFrom EverandAustralia's Dangerous Snakes: Identification, Biology and EnvenomingRating: 5 out of 5 stars5/5 (1)
- Ecdysozoa: Protostomes Are Divided Into Two Large Groups The Lophotrochozoa and The EcdysozoaDocument56 pagesEcdysozoa: Protostomes Are Divided Into Two Large Groups The Lophotrochozoa and The EcdysozoaOnyx CambalizaNo ratings yet
- Snakebite Symptoms, Causes, and Occupations at RiskDocument95 pagesSnakebite Symptoms, Causes, and Occupations at RisksrinivasNo ratings yet
- Do Assassin Bugs Exist? Fact-Checking Claims About the 'Hitman' InsectDocument6 pagesDo Assassin Bugs Exist? Fact-Checking Claims About the 'Hitman' InsecthalaNo ratings yet
- Explainer: Animals' Role in Human DiseaseDocument5 pagesExplainer: Animals' Role in Human DiseasejmorenograciaNo ratings yet
- America's Neighborhood Bats: Understanding and Learning to Live in Harmony with ThemFrom EverandAmerica's Neighborhood Bats: Understanding and Learning to Live in Harmony with ThemRating: 4 out of 5 stars4/5 (22)
- Chapter 13 Arthropods-TorresDocument20 pagesChapter 13 Arthropods-TorresRiven TruceNo ratings yet
- Insect Bites: Statpearls (Internet) - Treasure Island (FL) : Statpearls Publishing 2019 JanDocument12 pagesInsect Bites: Statpearls (Internet) - Treasure Island (FL) : Statpearls Publishing 2019 JanSrikitta DanieliaNo ratings yet
- Tears of the Cheetah: The Genetic Secrets of Our Animal AncestorsFrom EverandTears of the Cheetah: The Genetic Secrets of Our Animal AncestorsRating: 4.5 out of 5 stars4.5/5 (14)
- Full TextDocument59 pagesFull TextMohammed GaberNo ratings yet
- Chen2010_Article_NasalLeechInfestationReportOfSDocument5 pagesChen2010_Article_NasalLeechInfestationReportOfSronaldyohanesfNo ratings yet
- Special Topics and General Characteristics: Diseases Caused by ProtistaFrom EverandSpecial Topics and General Characteristics: Diseases Caused by ProtistaDavid WeinmanNo ratings yet
- Emergency Treatment of A Snake Bite: Pearls From LiteratureDocument13 pagesEmergency Treatment of A Snake Bite: Pearls From LiteratureLorentina Den PanjaitanNo ratings yet
- The Mosquito Book: An Entertaining, Fact-filled Look at the Dreaded Pesky BloodsuckersFrom EverandThe Mosquito Book: An Entertaining, Fact-filled Look at the Dreaded Pesky BloodsuckersNo ratings yet
- MAKALAH Snake BiteDocument6 pagesMAKALAH Snake BiteMutiara YuliantikaNo ratings yet
- Snake Bite Snake Venom Anti-Venom and Herbal AntidDocument8 pagesSnake Bite Snake Venom Anti-Venom and Herbal AntidJohn SnowNo ratings yet
- Parasites: Tales of Humanity's Most Unwelcome GuestsFrom EverandParasites: Tales of Humanity's Most Unwelcome GuestsRating: 3.5 out of 5 stars3.5/5 (6)
- First Aid For Snake BiteDocument11 pagesFirst Aid For Snake BiteHenryVanDerSchyffNo ratings yet
- Intestinal Nematodes: A Review.: Olushola S. Ayanda, M.Sc. Omolola T. Ayanda, B.Sc. and Folashade B. Adebayo, B.SCDocument12 pagesIntestinal Nematodes: A Review.: Olushola S. Ayanda, M.Sc. Omolola T. Ayanda, B.Sc. and Folashade B. Adebayo, B.SCmei purba100% (1)
- Parasitology 3 PDFDocument24 pagesParasitology 3 PDFEdgar MandengNo ratings yet
- Rabies An OverviewDocument6 pagesRabies An OverviewShahzad ZakiNo ratings yet
- Insects FriendsorenemiesDocument8 pagesInsects FriendsorenemiesOni MichaelNo ratings yet
- Desordenes Comunes de AmazonasDocument6 pagesDesordenes Comunes de AmazonasJessica RuizNo ratings yet
- Nematoda Roundworms IntroDocument4 pagesNematoda Roundworms IntroNICOLAS BORJA MARTINEZNo ratings yet
- Viper SnakeDocument12 pagesViper Snakejayasruthilaya18No ratings yet
- RECMOD10 Toxinology Bites and StingsDocument39 pagesRECMOD10 Toxinology Bites and Stingsdragon66No ratings yet
- Mind Power SecretsDocument38 pagesMind Power SecretsIan Faian92% (52)
- Vrs PresentationDocument24 pagesVrs PresentationshrutipalkarNo ratings yet
- School and CentreDocument24 pagesSchool and CentreThrilling PrinceNo ratings yet
- Laporan FaalDocument25 pagesLaporan FaalAgnes NathaniaNo ratings yet
- The Electrooculogram (EOG)Document34 pagesThe Electrooculogram (EOG)Prasidha PrabhuNo ratings yet
- Dupont Heir Sexually Abuses DaughterDocument3 pagesDupont Heir Sexually Abuses DaughterJuandelaCruzNo ratings yet
- Product Overview: NCV71208: Octal Solenoid Current Controller With N-FET PredriversDocument1 pageProduct Overview: NCV71208: Octal Solenoid Current Controller With N-FET PredriversDimitar PetrovNo ratings yet
- Duconmix CRP 400Document2 pagesDuconmix CRP 400FounTech612No ratings yet
- Training To See Auras v4 - Robert BruceDocument68 pagesTraining To See Auras v4 - Robert BruceYazan Ali100% (1)
- Edc Power Plant FacilitiesDocument32 pagesEdc Power Plant FacilitiesMichael TayactacNo ratings yet
- Aircraft Instruments and Avionics PDFDocument211 pagesAircraft Instruments and Avionics PDFairbuk doeing88% (8)
- Working Length Determination in RCTDocument38 pagesWorking Length Determination in RCTDidar Sadiq Kwekha100% (1)
- Silver Rain Svetlana Perevalova PDFDocument9 pagesSilver Rain Svetlana Perevalova PDFAndrea Koumarian100% (1)
- Fertilization to Implantation StagesDocument18 pagesFertilization to Implantation StagesNurulAqilahZulkifliNo ratings yet
- Beginning Algebra 9th Edition Tobey Solutions Manual 1Document39 pagesBeginning Algebra 9th Edition Tobey Solutions Manual 1kyle100% (30)
- Boiler Feedwater ControlDocument14 pagesBoiler Feedwater ControlJonas PeraterNo ratings yet
- Bill of Qty. N.C. Sharma, BILSI, BadaunDocument47 pagesBill of Qty. N.C. Sharma, BILSI, BadaunNazim AliNo ratings yet
- TDI - Full Cave Diver Course: TDI Instructor Manual Part 2 - Diver Standards Date: 12/31/2009 Revision: 10.0Document5 pagesTDI - Full Cave Diver Course: TDI Instructor Manual Part 2 - Diver Standards Date: 12/31/2009 Revision: 10.0BraulioNo ratings yet
- Arya Steels Ratings Remain StableDocument4 pagesArya Steels Ratings Remain StableData CentrumNo ratings yet
- Detox 101Document31 pagesDetox 101Botoşanu Diana-LarisaNo ratings yet
- MYK Grout Card 2Document2 pagesMYK Grout Card 2Abdul Raheem SyedNo ratings yet
- Kshitija's ResumeDocument1 pageKshitija's ResumeNavinNo ratings yet
- Method of Statement For Pipeline WorkDocument15 pagesMethod of Statement For Pipeline WorkHalil Güney100% (3)
- English Try Out UN 1 2008/2009Document4 pagesEnglish Try Out UN 1 2008/2009Cepiana Abas100% (10)
- Master FormDocument62 pagesMaster FormsamsulNo ratings yet
- Performance Evaluation of Sewage Treatment Plants (STPS) in Multistoried BuildingsDocument6 pagesPerformance Evaluation of Sewage Treatment Plants (STPS) in Multistoried BuildingsAnonymous iTzCnMNo ratings yet
- Chapter 11 Post-Emulsified Fluorescent (Hydrophilic & Lipophilic)Document13 pagesChapter 11 Post-Emulsified Fluorescent (Hydrophilic & Lipophilic)maxpan maxNo ratings yet
- 2requirements Permit PDFDocument1 page2requirements Permit PDFHazel CorralNo ratings yet
- Wazaif Totaky Home Remedies Receiver Software Powervu Key-1Document18 pagesWazaif Totaky Home Remedies Receiver Software Powervu Key-1Habib MohammedNo ratings yet
- Wolf Gone Wild - Juliette CrossDocument312 pagesWolf Gone Wild - Juliette CrossAbdelhediNo ratings yet