You might also like
- Hirschsprung’s Disease, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandHirschsprung’s Disease, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Learning: St. Mary'S College of Tagum, IncDocument37 pagesLearning: St. Mary'S College of Tagum, IncAlyssa Gaile EspirituNo ratings yet
- ASSESSMENT OF FETAL GROWTH AND DEVELOPMENTDocument84 pagesASSESSMENT OF FETAL GROWTH AND DEVELOPMENTAlessandra Franchesca CortezNo ratings yet
- Nursing As An ArtDocument4 pagesNursing As An ArtEmjae Colmenares100% (1)
- Fundamentals of Nursing Midterm ReviewDocument29 pagesFundamentals of Nursing Midterm ReviewCharisse CaydanNo ratings yet
- C5 - Eukayotic MicrobesDocument5 pagesC5 - Eukayotic MicrobesSchool driveNo ratings yet
- MS Eent (Nle)Document3 pagesMS Eent (Nle)Maginalyn CangasNo ratings yet
- STUDENTS' NOTES ON Assessment of Mouth, Throat, Nose andDocument8 pagesSTUDENTS' NOTES ON Assessment of Mouth, Throat, Nose andRolandNo ratings yet
- Medical Surgical Nursing Module 4Document17 pagesMedical Surgical Nursing Module 4weissNo ratings yet
- Mariano Marcos State University: College of Health SciencesDocument5 pagesMariano Marcos State University: College of Health SciencesLyca Mae Aurelio100% (1)
- Unit 4 Maternal ConceptsDocument8 pagesUnit 4 Maternal ConceptsEunice TrinidadNo ratings yet
- 41 Lecture AnimationDocument49 pages41 Lecture AnimationGissele AbolucionNo ratings yet
- Biochem Nutrition TransDocument7 pagesBiochem Nutrition TransCyril Dayne Marie BaldeNo ratings yet
- 3.3 Family PlanningDocument9 pages3.3 Family PlanningGayle Regine DaquialNo ratings yet
- Battery ExamsDocument71 pagesBattery ExamsJoana Grace CortezNo ratings yet
- Eye & Ear IrrigationDocument34 pagesEye & Ear IrrigationdaisyNo ratings yet
- HysterectomyDocument10 pagesHysterectomyJORINA PUMIHICNo ratings yet
- Nursing Care Plan: Submitted By: Sabay, Kyle VDocument11 pagesNursing Care Plan: Submitted By: Sabay, Kyle VKYLE SABAYNo ratings yet
- BIOETHICS: A STUDY OF ETHICAL ISSUES IN BIOLOGY AND MEDICINEDocument42 pagesBIOETHICS: A STUDY OF ETHICAL ISSUES IN BIOLOGY AND MEDICINERaven Evangelista CanaNo ratings yet
- Diabetes Mellitus NCPDocument6 pagesDiabetes Mellitus NCPJOHN CARLO APATANNo ratings yet
- Level III Performance ChecklistDocument43 pagesLevel III Performance ChecklistMikhaela Andree MarianoNo ratings yet
- Prepare and Care For Clients Scheduled For Medical ProcedureDocument40 pagesPrepare and Care For Clients Scheduled For Medical ProcedureAbekail BryanNo ratings yet
- I. Elimination Urinary CatheterizationDocument13 pagesI. Elimination Urinary CatheterizationEmma IntiaNo ratings yet
- Pathogenesis of Infectious Diseases ChapterDocument4 pagesPathogenesis of Infectious Diseases ChapterAllynne Jane DagasdasNo ratings yet
- Hand Hygiene: Alcohol Based Hand RubDocument2 pagesHand Hygiene: Alcohol Based Hand RubKIERSTINE MARIE BARCELONo ratings yet
- Don Mariano Marcos Memorial State University South La Union Campus Disaster Nursing CourseDocument24 pagesDon Mariano Marcos Memorial State University South La Union Campus Disaster Nursing CourseDenver M. OficiarNo ratings yet
- Bandaging 140511011904 Phpapp02Document46 pagesBandaging 140511011904 Phpapp02Kristela Mae ColomaNo ratings yet
- Frando-Detailed Learning Module 7.2.Document15 pagesFrando-Detailed Learning Module 7.2.Ranz Kenneth G. FrandoNo ratings yet
- FUNDA HAND-OUT - Nursing As A ProfessionDocument7 pagesFUNDA HAND-OUT - Nursing As A ProfessionYsabel Francesca AbadNo ratings yet
- Hand Out For Module 1.5Document17 pagesHand Out For Module 1.5weissNo ratings yet
- TAHBSO Procedure ExplainedDocument14 pagesTAHBSO Procedure ExplainedDafny CzarinaNo ratings yet
- Six Key Nursing Ethics: Autonomy, Privacy, ConfidentialityDocument17 pagesSix Key Nursing Ethics: Autonomy, Privacy, ConfidentialityRica ParcasioNo ratings yet
- In The Name of Allah, The Most Beneficent and MercifulDocument35 pagesIn The Name of Allah, The Most Beneficent and MercifulAhmedMenshawyNo ratings yet
- Adaptation ModelDocument7 pagesAdaptation ModelMichelle T. DimaanoNo ratings yet
- Module 1 - CytogeneticsDocument5 pagesModule 1 - CytogeneticsNursida LadjalawieNo ratings yet
- Ret DemsDocument103 pagesRet DemsPRECIOUS LOVE LAGRIMASNo ratings yet
- Pregnancy Lab Tests ExplainedDocument55 pagesPregnancy Lab Tests ExplainedJoseph DusichNo ratings yet
- Principles of Sterile Technique: Them That Varies. These Principles Are Applied in TheDocument22 pagesPrinciples of Sterile Technique: Them That Varies. These Principles Are Applied in Thecoosa liquorsNo ratings yet
- 2.1. Pharmacological Therapeutics. 2.2. Basic Cardiac Life Support (BCLS) and Advanced Cardiac Life Support (ACLS) in Neonates and ChildDocument3 pages2.1. Pharmacological Therapeutics. 2.2. Basic Cardiac Life Support (BCLS) and Advanced Cardiac Life Support (ACLS) in Neonates and Childclint xavier odangoNo ratings yet
- Aseptic TechniqueDocument9 pagesAseptic TechniqueFaith IriemiNo ratings yet
- Modes of InfectionDocument19 pagesModes of InfectionLinguumNo ratings yet
- Disaster NursingDocument15 pagesDisaster NursingDr. Jayesh PatidarNo ratings yet
- 2022 May CHN CD 1 TeamsDocument8 pages2022 May CHN CD 1 TeamsCrystal Ann TadiamonNo ratings yet
- Maternal and Child Nursing Case Presentation on Normal Spontaneous Vaginal DeliveryDocument100 pagesMaternal and Child Nursing Case Presentation on Normal Spontaneous Vaginal DeliveryJoj BagnateNo ratings yet
- H1N1 Diagnosis, Management and TreatmentDocument56 pagesH1N1 Diagnosis, Management and TreatmentNishanth BabuNo ratings yet
- Dietary Fiber - WikipediaDocument21 pagesDietary Fiber - WikipediaJohnNo ratings yet
- Roller Bandages: Head BandageDocument9 pagesRoller Bandages: Head BandageNicole AlemaniaNo ratings yet
- Vaccination or ImmunizationDocument4 pagesVaccination or ImmunizationPrincessNo ratings yet
- Bed MakingDocument9 pagesBed MakingandreabreeNo ratings yet
- Introduction To The Musculoskeletal SystemDocument39 pagesIntroduction To The Musculoskeletal SystemdesyNo ratings yet
- IntradermalDocument7 pagesIntradermalKyle Dapulag100% (1)
- Chapter 17 The Breasts and AxillaeDocument4 pagesChapter 17 The Breasts and AxillaeKhanh HoangNo ratings yet
- Communicable Diseases 2.4-5.22Document9 pagesCommunicable Diseases 2.4-5.22Vhince PiscoNo ratings yet
- Cell Ab Midterm MesiDocument7 pagesCell Ab Midterm MesiSamantha VeraNo ratings yet
- Checklist On Vital Signs - Blood Oxygenation Using Pulse OxymeterDocument2 pagesChecklist On Vital Signs - Blood Oxygenation Using Pulse Oxymeteraliyah2 sanchezNo ratings yet
- Concept of isolation in microbiologyDocument9 pagesConcept of isolation in microbiologyUrdu Kahani100% (1)
- MCN Skills 2021 Procedure ChecklistDocument3 pagesMCN Skills 2021 Procedure ChecklistNashebah A. BatuganNo ratings yet
- NCM101 Health Assessment ExaminationDocument11 pagesNCM101 Health Assessment ExaminationJonah R. Merano100% (1)
- GI Drugs Classification GuideDocument29 pagesGI Drugs Classification GuideJeneyse Ajap BalcenaNo ratings yet
- 5 Nursing As A ScienceDocument31 pages5 Nursing As A ScienceeningNo ratings yet
- NCM 104 Home VisitDocument10 pagesNCM 104 Home VisitPinsoy, Bruce riano e.No ratings yet
- Beckman Coulter PK TP Feb2012Document16 pagesBeckman Coulter PK TP Feb2012Inês LoboNo ratings yet
- Amith V PresentationDocument22 pagesAmith V PresentationjacoblbawlteNo ratings yet
- Creating "Tangguh VillageDocument17 pagesCreating "Tangguh VillageArizal RivaldhyNo ratings yet
- CertificateDocument1 pageCertificateRanjana RanjanaNo ratings yet
- Gambaran Klinis Dan Laboratorium Pada Pasien Pneumonia Di Icu Rsud Raden Mattaher JambiDocument7 pagesGambaran Klinis Dan Laboratorium Pada Pasien Pneumonia Di Icu Rsud Raden Mattaher JambigusdeNo ratings yet
- Notification District Health Society Chittoor MO ANM Pharmacist PostsDocument8 pagesNotification District Health Society Chittoor MO ANM Pharmacist PostsRohitRajakNo ratings yet
- A Brief History of Acupuncture: Rheumatology June 2004Document3 pagesA Brief History of Acupuncture: Rheumatology June 2004Rudolph Antony Thomas100% (1)
- Department of Education: Region Vi-Western Visayas Schools Division of SipalayDocument3 pagesDepartment of Education: Region Vi-Western Visayas Schools Division of SipalayRoseo BatillerNo ratings yet
- CovidDocument110 pagesCovidHendhy WaluyoNo ratings yet
- Journal Reading: Pembimbing: Dr. Shandy Limansyahputra SP - OTDocument41 pagesJournal Reading: Pembimbing: Dr. Shandy Limansyahputra SP - OTsabariaNo ratings yet
- UAE Registration Requirements For General Sale List (GSL) ProductsDocument2 pagesUAE Registration Requirements For General Sale List (GSL) Productspandita bumikalimasadaNo ratings yet
- Konsep Dasar, Optimalisasi, Dan Teknik Pengurangan Dosis Pada Pesawat CT ScanDocument31 pagesKonsep Dasar, Optimalisasi, Dan Teknik Pengurangan Dosis Pada Pesawat CT Scanrifqi anisaNo ratings yet
- Influenza Della Condotta Anestesiologica Sullo Stato Mentale Di Soggetti AnzianiDocument7 pagesInfluenza Della Condotta Anestesiologica Sullo Stato Mentale Di Soggetti AnzianiMatteo BrambatiNo ratings yet
- MyCare UCLH - Appointments and VisitsDocument1 pageMyCare UCLH - Appointments and VisitsMing WuNo ratings yet
- MARIE CRISELLE CASIMJuly 26 2023-Letter of AuthorizationDocument1 pageMARIE CRISELLE CASIMJuly 26 2023-Letter of Authorizationjqm printingNo ratings yet
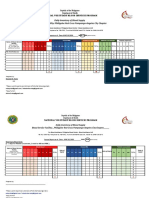
- Daily Inventory of Blood Supply Blood Service Facility: Philippine Red Cross Pampanga-Angeles City ChapterDocument2 pagesDaily Inventory of Blood Supply Blood Service Facility: Philippine Red Cross Pampanga-Angeles City ChapterFrances DeiNo ratings yet
- ASPAK KalibrasiDocument2 pagesASPAK KalibrasiLaboratorium PKM DarmarajaNo ratings yet
- BahasaDocument8 pagesBahasaLailatan Nisfi Sya'banNo ratings yet
- MCQ Pharmacognosy Iii Sem Vii Mock Test Nov 2020Document4 pagesMCQ Pharmacognosy Iii Sem Vii Mock Test Nov 2020Hira Enayatullah KhanNo ratings yet
- Surgical Scrubbing Procedure StudentsDocument4 pagesSurgical Scrubbing Procedure StudentsJulianne Kyla MercadoNo ratings yet
- Numerical Solution of SIRS Model for Dengue Fever TransmissionDocument12 pagesNumerical Solution of SIRS Model for Dengue Fever TransmissionRohan sharmaNo ratings yet
- Em American Journal of Infection Control em ObjDocument2 pagesEm American Journal of Infection Control em ObjKhadiga AhmadNo ratings yet
- Session PlanDocument9 pagesSession PlanKirsten Q. CaminongNo ratings yet
- Department of Education: Health Declaration FormDocument1 pageDepartment of Education: Health Declaration FormYanna AbarquezNo ratings yet
- Sasaran BIAN Ds. JuntiDocument45 pagesSasaran BIAN Ds. JuntifebriNo ratings yet
- 2.C. Laporan Penyimpanan ObatDocument9 pages2.C. Laporan Penyimpanan ObatNovi AstutiNo ratings yet
- ScriptDocument7 pagesScriptIvan Matthew SuperioNo ratings yet
- Aconite PoisoningDocument15 pagesAconite PoisoningShagun TyagiNo ratings yet
- DAR ChartingDocument2 pagesDAR ChartingJed Visaya83% (6)