You might also like
- Critical Care Nurse Burnout, Moral Distress, and Mental Health During The COVID-19 Pandemic - A United States SurveyDocument8 pagesCritical Care Nurse Burnout, Moral Distress, and Mental Health During The COVID-19 Pandemic - A United States SurveyBiblioteca Médica CDS -HGZcMF-1No ratings yet
- 19 - Factor AssociadoDocument35 pages19 - Factor Associadohugo f.cNo ratings yet
- Psychological Challenges Encountered by HCPDocument7 pagesPsychological Challenges Encountered by HCPHarsha AgarwalNo ratings yet
- Sars Mental Health HCW2Document7 pagesSars Mental Health HCW2Abraham ChiuNo ratings yet
- Frontline ResilienceDocument24 pagesFrontline ResilienceEdiputriNo ratings yet
- Covid-19: Its Impact To The Healthcare Workers' Physical and Mental HealthDocument7 pagesCovid-19: Its Impact To The Healthcare Workers' Physical and Mental HealthJovilyn AjosteNo ratings yet
- The Spread of COVID19 in The Pakistan Anxiety, Depression and Post-Traumatic Stress DisorderDocument5 pagesThe Spread of COVID19 in The Pakistan Anxiety, Depression and Post-Traumatic Stress DisorderIJRASETPublicationsNo ratings yet
- COVID-19 Anxiety Among Front-Line Nurses: Predictive Role of Organisational Support, Personal Resilience and Social SupportDocument9 pagesCOVID-19 Anxiety Among Front-Line Nurses: Predictive Role of Organisational Support, Personal Resilience and Social SupportAnis MahmudahNo ratings yet
- 2021 - Issues Facing Post Pandemic Nuring Workforce in Oregon - Stress and Emotional HealthDocument3 pages2021 - Issues Facing Post Pandemic Nuring Workforce in Oregon - Stress and Emotional HealthnidikumbaraNo ratings yet
- Mental Health Among Healthcare Personnel During COVID-19 in Asia: A Systematic ReviewDocument9 pagesMental Health Among Healthcare Personnel During COVID-19 in Asia: A Systematic ReviewLaras KinasihNo ratings yet
- Resilience Strategies To Manage Psychological Distress Among Healthcare Workers During The COVID-19 Pandemic: A Narrative ReviewDocument8 pagesResilience Strategies To Manage Psychological Distress Among Healthcare Workers During The COVID-19 Pandemic: A Narrative ReviewdinarNo ratings yet
- NurseDocument4 pagesNurseTheresa Mae PansaonNo ratings yet
- Sustainability 12 09004 v2Document18 pagesSustainability 12 09004 v2Vlad CristinaNo ratings yet
- PortugueseDocument12 pagesPortugueseAna RibeiroNo ratings yet
- COVID-19 Pandemicandhealthworkerstress: Themediating Effect of Emotional RegulationDocument13 pagesCOVID-19 Pandemicandhealthworkerstress: Themediating Effect of Emotional RegulationShukri RahmanNo ratings yet
- 1 s2.0 S0967586820314399 MainDocument6 pages1 s2.0 S0967586820314399 MainKhofifah Erga SalsabilaNo ratings yet
- EpidDocument8 pagesEpidacoarif991No ratings yet
- Anxiety and Resilience of Healthcare Workers During COVID-19 Pandemic in IndonesiaDocument8 pagesAnxiety and Resilience of Healthcare Workers During COVID-19 Pandemic in IndonesiaYadira LagunesNo ratings yet
- Covid-19 Anxiety Among Frontline Nurses: Predictive Role of Organisational Support, Personal Resilience and Social SupportDocument25 pagesCovid-19 Anxiety Among Frontline Nurses: Predictive Role of Organisational Support, Personal Resilience and Social SupportAna May BanielNo ratings yet
- BARING & EZPELETA - Degree of Burnout and Its Association With Depression For SubmissionDocument73 pagesBARING & EZPELETA - Degree of Burnout and Its Association With Depression For SubmissionVirginia AbalosNo ratings yet
- Applying The Lessons of SARSDocument3 pagesApplying The Lessons of SARSZoran RadosevicNo ratings yet
- Brain, Behavior, and ImmunityDocument9 pagesBrain, Behavior, and ImmunityIndah NurlathifahNo ratings yet
- General Hospital Psychiatry: SciencedirectDocument14 pagesGeneral Hospital Psychiatry: Sciencedirectshinta aryNo ratings yet
- Caring For The Psychological Well-Being of Healthcare Professionals in The Covid-19 Pandemic CrisisDocument3 pagesCaring For The Psychological Well-Being of Healthcare Professionals in The Covid-19 Pandemic CrisisSanti Novita ArianiNo ratings yet
- Referensi 47Document7 pagesReferensi 47SaebaNo ratings yet
- Listening To Hospital Personnel's Narratives During The COVID-19 OutbreakDocument15 pagesListening To Hospital Personnel's Narratives During The COVID-19 OutbreakAshers NyawoNo ratings yet
- Mental Health of Nurses During The Fourth Wave of The COVID-19 Pandemic in PolandDocument12 pagesMental Health of Nurses During The Fourth Wave of The COVID-19 Pandemic in PolandLency CahyaningsihNo ratings yet
- Preti Et Al 2020Document22 pagesPreti Et Al 2020Carlos muñozNo ratings yet
- Brain, Behavior, and Immunity: SciencedirectDocument7 pagesBrain, Behavior, and Immunity: SciencedirectMarinela MeliszekNo ratings yet
- Sanliturk 2021Document6 pagesSanliturk 2021AamirNo ratings yet
- 14.+61860 115-120Document6 pages14.+61860 115-120Dwi NopriyantoNo ratings yet
- Depression in Healthcare WorkersDocument11 pagesDepression in Healthcare WorkersLouis VidalNo ratings yet
- 4883-PDF Galley-29565-1-10-20200730Document7 pages4883-PDF Galley-29565-1-10-20200730Irfan HussainNo ratings yet
- The Global Prevalence of Anxiety DepressDocument19 pagesThe Global Prevalence of Anxiety DepresswalkensiocsNo ratings yet
- Jurnal English Covid.7Document7 pagesJurnal English Covid.7Dina AryaniNo ratings yet
- Ijshr0038 PDFDocument9 pagesIjshr0038 PDFNilakshi Barik MandalNo ratings yet
- The Psychological Impact of COVID-19 On Front Line NursesDocument17 pagesThe Psychological Impact of COVID-19 On Front Line NursesPetar PanNo ratings yet
- 1 s2.0 S0165032723003397 MainDocument17 pages1 s2.0 S0165032723003397 MainNariman Abed Alganey AkariNo ratings yet
- 1 s2.0 S0165178122003341 Main 2Document7 pages1 s2.0 S0165178122003341 Main 2Roberto Alexis Molina CampuzanoNo ratings yet
- Mental Health Issues Among Health Care Workers During The COVID-19 Pandemic A Study From IndiaDocument6 pagesMental Health Issues Among Health Care Workers During The COVID-19 Pandemic A Study From IndiaYingying XuNo ratings yet
- Secondary Traumatic Stress and DissociativeDocument7 pagesSecondary Traumatic Stress and DissociativePriskila Nadya EngridaNo ratings yet
- Mitigating The Psychological Impact of COVID-19 On Healthcare Workers: A Digital Learning PackageDocument15 pagesMitigating The Psychological Impact of COVID-19 On Healthcare Workers: A Digital Learning PackagekodagaNo ratings yet
- Prevention of Occupational Stress in Health-Care Workers During COVID-19 PandemicDocument3 pagesPrevention of Occupational Stress in Health-Care Workers During COVID-19 PandemicLaras KinasihNo ratings yet
- Covi̇dde Tükenmi̇şli̇kDocument8 pagesCovi̇dde Tükenmi̇şli̇kTalipNo ratings yet
- Final Document White Paper 3Document19 pagesFinal Document White Paper 3api-672832076No ratings yet
- Burnout in Hospital Based Healthcare Workers During COVID 19 - Published - 20211007 1Document24 pagesBurnout in Hospital Based Healthcare Workers During COVID 19 - Published - 20211007 1Riwa DeghaimNo ratings yet
- EpuizareDocument4 pagesEpuizareMaria-Emanuela SultanaNo ratings yet
- 2021 Psychological Distress Among Healthcare Providers During COVID-19 in Asia - Systematic Review and Meta-AnalysisDocument24 pages2021 Psychological Distress Among Healthcare Providers During COVID-19 in Asia - Systematic Review and Meta-AnalysisMary MonikaNo ratings yet
- 01 DescriptivosDocument24 pages01 DescriptivosDuneska GomezNo ratings yet
- Ijerph 18 00861Document10 pagesIjerph 18 00861shameless.No ratings yet
- CHINADocument13 pagesCHINAGloria Estefany Chije AnayaNo ratings yet
- Psychiatry Research: Review ArticleDocument11 pagesPsychiatry Research: Review ArticledominiakzsoltNo ratings yet
- Student's First Name, Middle Initial(s), Last Name: Research OutlineDocument6 pagesStudent's First Name, Middle Initial(s), Last Name: Research OutlineNahshon UnsimilarNo ratings yet
- Chapter 1 FINALDocument5 pagesChapter 1 FINALYoonah FlaminiaNo ratings yet
- A Rapid Review of The Impact oDocument19 pagesA Rapid Review of The Impact oYosi Reskhiyani SimamoraNo ratings yet
- Orca Share Media1682588605040 7057288116474940411Document13 pagesOrca Share Media1682588605040 7057288116474940411Yuji itadoriNo ratings yet
- Psychiatry Research: A 1 B 1 C ADocument5 pagesPsychiatry Research: A 1 B 1 C AClaudya TamaNo ratings yet
- Healthcare 11 00976Document15 pagesHealthcare 11 00976Jose AndresNo ratings yet
- 1 s2.0 S0196655320306386 MainDocument7 pages1 s2.0 S0196655320306386 MainOktomi WijayaNo ratings yet
- The COVID-19 Response: The Vital Role of the Public Health ProfessionalFrom EverandThe COVID-19 Response: The Vital Role of the Public Health ProfessionalNo ratings yet
- Moderating Role of Resilience in The Relationship Between Grit and Psychological Well-BeingDocument15 pagesModerating Role of Resilience in The Relationship Between Grit and Psychological Well-BeingMáthé AdriennNo ratings yet
- 2020 - 7617 25335 2 PBDocument15 pages2020 - 7617 25335 2 PBMáthé AdriennNo ratings yet
- ContentServer 3Document30 pagesContentServer 3Máthé AdriennNo ratings yet
- Motor Development and Neuropsychological Patterns in Persons With Down SyndromeDocument10 pagesMotor Development and Neuropsychological Patterns in Persons With Down SyndromeMáthé AdriennNo ratings yet
- Ijerph 17 00807 v2Document10 pagesIjerph 17 00807 v2Máthé AdriennNo ratings yet
- j.1545 5300.2006.00193.x20211017 12256 B5i5nb With Cover Page v2Document15 pagesj.1545 5300.2006.00193.x20211017 12256 B5i5nb With Cover Page v2Máthé AdriennNo ratings yet
- 9989 Etarjome EnglishDocument8 pages9989 Etarjome EnglishMáthé AdriennNo ratings yet
- Violence, Displacement, Contact, and Attitudes Toward Hosting RefugeesDocument16 pagesViolence, Displacement, Contact, and Attitudes Toward Hosting RefugeesMáthé AdriennNo ratings yet
- Kaplan 1977Document9 pagesKaplan 1977Máthé AdriennNo ratings yet
- J Semperi 2006 01 001Document9 pagesJ Semperi 2006 01 001Máthé AdriennNo ratings yet
- Vangasse 2020Document13 pagesVangasse 2020Máthé AdriennNo ratings yet
- Symoens 2013Document21 pagesSymoens 2013Máthé AdriennNo ratings yet
- Advances in Prenatal Screening For Down Syndrome - General Principles and Second Trimester TestingDocument16 pagesAdvances in Prenatal Screening For Down Syndrome - General Principles and Second Trimester TestingMáthé AdriennNo ratings yet
- Slovic 538Document30 pagesSlovic 538Máthé AdriennNo ratings yet
- Steele 2018Document25 pagesSteele 2018Máthé AdriennNo ratings yet
- The Conditional Effects of The Refugee Crisis On Immigration Attitudes and NationalismDocument21 pagesThe Conditional Effects of The Refugee Crisis On Immigration Attitudes and NationalismMáthé AdriennNo ratings yet
- Political Psychology - 2020 - Knappert - Personal Contact With Refugees Is Key To Welcoming Them An Analysis ofDocument20 pagesPolitical Psychology - 2020 - Knappert - Personal Contact With Refugees Is Key To Welcoming Them An Analysis ofMáthé AdriennNo ratings yet
- International Migration ReviewDocument31 pagesInternational Migration ReviewMáthé AdriennNo ratings yet
- Verkuyten 2021Document2 pagesVerkuyten 2021Máthé AdriennNo ratings yet
- CDP 19 3 332Document10 pagesCDP 19 3 332Máthé AdriennNo ratings yet
- Subjects' Expectations, Individual Variability, and The Scanning of Mental ImagesDocument6 pagesSubjects' Expectations, Individual Variability, and The Scanning of Mental ImagesMáthé AdriennNo ratings yet
- 0013916500326005ebbe Is Van Jó Problámamegoldó FeladatDocument15 pages0013916500326005ebbe Is Van Jó Problámamegoldó FeladatMáthé AdriennNo ratings yet
- Pharmacological Interventions To Improve Cognition and Adaptive Functioning in Down Syndrome: Strides To DateDocument13 pagesPharmacological Interventions To Improve Cognition and Adaptive Functioning in Down Syndrome: Strides To DateMáthé AdriennNo ratings yet
- Emotion Cognition and Decision MakingDocument8 pagesEmotion Cognition and Decision MakingMáthé AdriennNo ratings yet
- Neurologic Complications of Down Syndrome: A Systematic ReviewDocument15 pagesNeurologic Complications of Down Syndrome: A Systematic ReviewMáthé AdriennNo ratings yet
- Dileo 2020Document22 pagesDileo 2020Máthé AdriennNo ratings yet
- Dixon Gordon2011Document18 pagesDixon Gordon2011Máthé AdriennNo ratings yet
- Psychiatry Research 273 (2019) 493-500Document8 pagesPsychiatry Research 273 (2019) 493-500Máthé AdriennNo ratings yet
- Adolescent Decision Making:: The Influence of Mood, Age, and Gender On The Consideration of InformationDocument30 pagesAdolescent Decision Making:: The Influence of Mood, Age, and Gender On The Consideration of InformationMáthé AdriennNo ratings yet
- Kee-Lee ChouDocument9 pagesKee-Lee ChouMáthé AdriennNo ratings yet
- Fundamental RightsDocument55 pagesFundamental RightsDivanshuSharmaNo ratings yet
- Final Project Report GMS BtechDocument68 pagesFinal Project Report GMS Btech02Musaib Ul FayazNo ratings yet
- VISCOROL Series - Magnetic Level Indicators: DescriptionDocument4 pagesVISCOROL Series - Magnetic Level Indicators: DescriptionRaduNo ratings yet
- UCAT SJT Cheat SheetDocument3 pagesUCAT SJT Cheat Sheetmatthewgao78No ratings yet
- Codex Standard EnglishDocument4 pagesCodex Standard EnglishTriyaniNo ratings yet
- Simavi - Project Officer PROPOPIDocument4 pagesSimavi - Project Officer PROPOPIAgus NugrahaNo ratings yet
- La Salle Lipa Integrated School Senior High School Community 1 Quarter Summative Assessment Earth Science AY 2021-2022 Household Conservation PlanDocument4 pagesLa Salle Lipa Integrated School Senior High School Community 1 Quarter Summative Assessment Earth Science AY 2021-2022 Household Conservation PlanKarlle ObviarNo ratings yet
- KrauseDocument3 pagesKrauseVasile CuprianNo ratings yet
- Sales Manager Latin AmericaDocument3 pagesSales Manager Latin Americaapi-76934736No ratings yet
- Introduction To Wireless and Mobile Systems 4th Edition Agrawal Solutions ManualDocument12 pagesIntroduction To Wireless and Mobile Systems 4th Edition Agrawal Solutions Manualethelbertsangffz100% (34)
- Question Paper: Hygiene, Health and SafetyDocument2 pagesQuestion Paper: Hygiene, Health and Safetywf4sr4rNo ratings yet
- Project Job Number EngineerDocument2 pagesProject Job Number Engineertekno plus banatNo ratings yet
- tdr100 - DeviceDocument4 pagestdr100 - DeviceSrđan PavićNo ratings yet
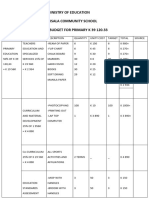
- Ministry of Education Musala SCHDocument5 pagesMinistry of Education Musala SCHlaonimosesNo ratings yet
- ATLAS HONDA Internship ReportDocument83 pagesATLAS HONDA Internship ReportAhmed Aitsam93% (14)
- Assessment 21GES1475Document4 pagesAssessment 21GES1475kavindupunsara02No ratings yet
- Legal Ethics HW 5Document7 pagesLegal Ethics HW 5Julius Robert JuicoNo ratings yet
- Data Book: Automotive TechnicalDocument1 pageData Book: Automotive TechnicalDima DovgheiNo ratings yet
- Journal of Economic LiteratureDocument28 pagesJournal of Economic LiteratureEkoKurniadiNo ratings yet
- Marley Product Catalogue Brochure Grease TrapsDocument1 pageMarley Product Catalogue Brochure Grease TrapsKushalKallychurnNo ratings yet
- Service Manual: Model: R410, RB410, RV410, RD410 SeriesDocument116 pagesService Manual: Model: R410, RB410, RV410, RD410 SeriesJorge Eustaquio da SilvaNo ratings yet
- Supreme Court of The United StatesDocument296 pagesSupreme Court of The United StatesABC News PoliticsNo ratings yet
- CT018 3 1itcpDocument31 pagesCT018 3 1itcpraghav rajNo ratings yet
- Awais Inspector-PaintingDocument6 pagesAwais Inspector-PaintingMohammed GaniNo ratings yet
- CSA Report Fahim Final-1Document10 pagesCSA Report Fahim Final-1Engr Fahimuddin QureshiNo ratings yet
- Amel Forms & Logging SheetsDocument4 pagesAmel Forms & Logging SheetsisaacNo ratings yet
- Te 1569 Web PDFDocument272 pagesTe 1569 Web PDFdavid19890109No ratings yet
- 1980WB58Document167 pages1980WB58AKSNo ratings yet
- Mpi Model QuestionsDocument4 pagesMpi Model QuestionshemanthnagNo ratings yet