You might also like
- Case PCAPDocument2 pagesCase PCAPNina Anne ParacadNo ratings yet
- IV Therapy - Asynchronous ActivityDocument2 pagesIV Therapy - Asynchronous ActivityNicole Chloe OcanaNo ratings yet
- Managing COPD: Nursing Care for Breathing Issues, Nutrition, Infection RiskDocument2 pagesManaging COPD: Nursing Care for Breathing Issues, Nutrition, Infection RiskAl RizkyNo ratings yet
- Foreign Body in The NoseDocument32 pagesForeign Body in The NoseLady350zNo ratings yet
- Nursing Assessment:: Intervention Rationale Independent InterventionsDocument2 pagesNursing Assessment:: Intervention Rationale Independent Interventionsnananana123No ratings yet
- A Simple Guide to Hypovolemia, Diagnosis, Treatment and Related ConditionsFrom EverandA Simple Guide to Hypovolemia, Diagnosis, Treatment and Related ConditionsNo ratings yet
- Case Presentation IM DDHDocument12 pagesCase Presentation IM DDHAishwarya BharathNo ratings yet
- Case Presentation On Supraventricular TachycardiaDocument64 pagesCase Presentation On Supraventricular TachycardiaHazel AsperaNo ratings yet
- Physician'S Order/Progress Notes: 23 S. Avila Male JhonDocument2 pagesPhysician'S Order/Progress Notes: 23 S. Avila Male JhonKrizha Angela Nicolas100% (1)
- Steps To Perform A Blood TransfusionDocument1 pageSteps To Perform A Blood Transfusionzepoli_zepoly6232No ratings yet
- Pediatric Bronchitis Case PresentationDocument28 pagesPediatric Bronchitis Case PresentationJoshua DulayNo ratings yet
- Case Presentation On Chronic Osteomyelitis: Prepared By: Sital Gautam MN1 Year, 2012Document55 pagesCase Presentation On Chronic Osteomyelitis: Prepared By: Sital Gautam MN1 Year, 2012Rabina RajbanshiNo ratings yet
- Sree Vasantham Hospital, Salem: 1. Er Protocol For Acute Intoxication (Poisoning)Document7 pagesSree Vasantham Hospital, Salem: 1. Er Protocol For Acute Intoxication (Poisoning)Elango MuthuNo ratings yet
- Community-Acquired Pneumonia GuideDocument37 pagesCommunity-Acquired Pneumonia GuideKristine-Joy Legaspi FrancoNo ratings yet
- Types of Insulin PDFDocument3 pagesTypes of Insulin PDFRetno WulanNo ratings yet
- Tuberculosis: Dr.V. Gangadharan Professor & Hod Department of Respiratory Medicine Saveetha Medical College HospitalDocument58 pagesTuberculosis: Dr.V. Gangadharan Professor & Hod Department of Respiratory Medicine Saveetha Medical College HospitalJoanna RachelNo ratings yet
- Problem-based Approach to Gastroenterology and HepatologyFrom EverandProblem-based Approach to Gastroenterology and HepatologyJohn N. PlevrisNo ratings yet
- Pat 2 Medsurg1Document20 pagesPat 2 Medsurg1api-300849832No ratings yet
- Bedside Nurse: Name of Student: Jela Mae V. Pates Score: - /25Document8 pagesBedside Nurse: Name of Student: Jela Mae V. Pates Score: - /25janna mae patriarcaNo ratings yet
- Management of Hypertensive CrisisDocument20 pagesManagement of Hypertensive CrisisKia AgusputraNo ratings yet
- Action Plan PICU FINALDocument2 pagesAction Plan PICU FINALMark MacasadduNo ratings yet
- Pedia HX Seizure 1Document25 pagesPedia HX Seizure 1Amer Hussein DomadoNo ratings yet
- Pet CTDocument4 pagesPet CTKanishk R.SinghNo ratings yet
- Post Op CareDocument7 pagesPost Op CareJeraldien Diente TagamolilaNo ratings yet
- Anthrax Clinical PathwayDocument4 pagesAnthrax Clinical PathwayNeurologianak HarkitNo ratings yet
- A Simple Guide to Circulatory Shock, Diagnosis, Treatment and Related ConditionsFrom EverandA Simple Guide to Circulatory Shock, Diagnosis, Treatment and Related ConditionsNo ratings yet
- Asthma Patient ProfileDocument8 pagesAsthma Patient ProfileGlenn Asuncion PagaduanNo ratings yet
- Nasogastric Tube (NGT) InsertionDocument19 pagesNasogastric Tube (NGT) InsertionNorman VerdeflorNo ratings yet
- Mechanical VentilationDocument9 pagesMechanical VentilationMario MagtakaNo ratings yet
- Pertussis Case Definition and Investigation PresentationDocument62 pagesPertussis Case Definition and Investigation PresentationMuhammad Jahari Supianto100% (1)
- PRE ANAESTHETIC ASSESSMENT New 1Document41 pagesPRE ANAESTHETIC ASSESSMENT New 1lokeswara reddyNo ratings yet
- Pneumonectomy 2Document7 pagesPneumonectomy 2jeanelineNo ratings yet
- Patient Information From Your Surgeon & Sages Laparoscopic Gallbladder RemovalDocument5 pagesPatient Information From Your Surgeon & Sages Laparoscopic Gallbladder RemovalolarrozaNo ratings yet
- ICU Case Study: 53-Year-Old Male with Organophosphate PoisoningDocument11 pagesICU Case Study: 53-Year-Old Male with Organophosphate PoisoningPrasyaanth RajanNo ratings yet
- Nurse'S Notes: Date-Shift Focus Data - Action - ResponseDocument5 pagesNurse'S Notes: Date-Shift Focus Data - Action - ResponseRenea Joy ArruejoNo ratings yet
- SuturesDocument62 pagesSuturesShanmuga PriyaNo ratings yet
- Nursing Care Plan for Client with Major BurnDocument2 pagesNursing Care Plan for Client with Major BurnMaricel R. ManabatNo ratings yet
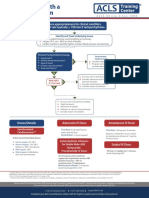
- Assess Appropriateness For Clinical Condition. Heart Rate Typically 150/min If TachyarrhythmiaDocument1 pageAssess Appropriateness For Clinical Condition. Heart Rate Typically 150/min If TachyarrhythmiaSiti Nur R Firda FauziyahNo ratings yet
- Capnography in ICUDocument49 pagesCapnography in ICUherbertglennyNo ratings yet
- Burns CH 25 n-7Document7 pagesBurns CH 25 n-7Jessica VargasNo ratings yet
- Capnometry: Dhanya VDocument49 pagesCapnometry: Dhanya VdaviddanamrajanNo ratings yet
- Congenital Diaphragmatic Hernia: Pediatric Surgery DepartmentDocument32 pagesCongenital Diaphragmatic Hernia: Pediatric Surgery DepartmentTuan Ahamed CassimNo ratings yet
- Nasogastric Intubation Medical NCO CourseDocument32 pagesNasogastric Intubation Medical NCO CourseBilly PeterNo ratings yet
- Airway ManagementDocument63 pagesAirway ManagementGilang GumilangNo ratings yet
- Tension Pneumothorax: Modifiable FactorsDocument3 pagesTension Pneumothorax: Modifiable FactorsJustin MaverickNo ratings yet
- Operating RoomDocument13 pagesOperating RoomrichardNo ratings yet
- Abbreviation NursingDocument16 pagesAbbreviation NursingPeter Lucky Turiano100% (1)
- HydronephrosisDocument6 pagesHydronephrosisJamaluddin Ahmad A.MNo ratings yet
- Cap MR DDHDocument32 pagesCap MR DDHLovelle LopezNo ratings yet
- TonsillectomyDocument27 pagesTonsillectomyRho Vince Caño MalagueñoNo ratings yet
- CAPNOGRAPHYDocument72 pagesCAPNOGRAPHYNikita JainNo ratings yet
- History and Physical Exam For COPDDocument10 pagesHistory and Physical Exam For COPDCathy GuerreroNo ratings yet
- Case Study Burn InjuryDocument9 pagesCase Study Burn InjuryAmber Dawn MonteroNo ratings yet
- Acute Glomerulonephritis Case StudyDocument6 pagesAcute Glomerulonephritis Case StudyjakerzNo ratings yet
- Case Presentation Meyke Liechandra C11109130 Fracture ClavicleDocument24 pagesCase Presentation Meyke Liechandra C11109130 Fracture ClavicleWahyunita IlhamNo ratings yet
- Orientation To Blood Bank 2Document24 pagesOrientation To Blood Bank 2Darshita SharmaNo ratings yet
- Cor Pulmonale Lesson PlanDocument49 pagesCor Pulmonale Lesson PlanRadha Sri50% (2)
- Tracheostomy Procedure GuideDocument18 pagesTracheostomy Procedure GuideSudhanshu ShekharNo ratings yet
- Acute Respiratory Distress SyndromDocument38 pagesAcute Respiratory Distress SyndrompatriaindraNo ratings yet
- RBC Indices & ESRDocument23 pagesRBC Indices & ESRPamela BesanaNo ratings yet
- Yusi - Anatomy of The Urinary Tract 2009 12-7Document129 pagesYusi - Anatomy of The Urinary Tract 2009 12-7abstabsNo ratings yet
- Drugs of Autonomic Nervous SystemDocument34 pagesDrugs of Autonomic Nervous SystemWyz Class100% (1)
- The gross structure of the human respiratory systemDocument14 pagesThe gross structure of the human respiratory systemSaraNo ratings yet
- Frecvența Și Predictorii Depresiei În Insuficiența Cardiacă CongestivaDocument5 pagesFrecvența Și Predictorii Depresiei În Insuficiența Cardiacă CongestivaAdina CipariuNo ratings yet
- 2.4.3 Child Health Nursing (Pediatric Nursing) Papers QPDocument17 pages2.4.3 Child Health Nursing (Pediatric Nursing) Papers QPTapobrata Sarkar100% (2)
- Congenital Diaphragmatic HerniaDocument48 pagesCongenital Diaphragmatic HerniaShahd IdaisNo ratings yet
- Arrhythmia Recognition Poster Part 2Document1 pageArrhythmia Recognition Poster Part 2Gwen LylesNo ratings yet
- Differential Diagnosis of TBC Pleurisy.Document13 pagesDifferential Diagnosis of TBC Pleurisy.Yvonne Nmeli MihesNo ratings yet
- Literature Review of Liver DiseaseDocument7 pagesLiterature Review of Liver Diseaseeeyjzkwgf100% (1)
- Drug Study: TramadolDocument5 pagesDrug Study: TramadolOmyl-Khayr M. SulogNo ratings yet
- QBase Anaesthesia 1Document209 pagesQBase Anaesthesia 1Sanj.etcNo ratings yet
- Atlas of Physical SignsDocument168 pagesAtlas of Physical SignsspankymaxNo ratings yet
- Thorax RadiologyDocument31 pagesThorax Radiologyshanti kiranaNo ratings yet
- Essential Revision Notes For MRCP PDFDocument1,002 pagesEssential Revision Notes For MRCP PDFMontasir Ahmed100% (23)
- Assignment Gaseous ExchangeDocument10 pagesAssignment Gaseous ExchangefetramyraNo ratings yet
- 2 - Regional Anatomy (MidTerm) MCQsDocument18 pages2 - Regional Anatomy (MidTerm) MCQsManju ShreeNo ratings yet
- Aiapget 2019 QPDocument10 pagesAiapget 2019 QPGanesh RadhakrishnanNo ratings yet
- GIT OverviewDocument108 pagesGIT OverviewNasser SalahNo ratings yet
- Application For Reinstatement of Plan Agreement (Revised As of July 21, 2021)Document3 pagesApplication For Reinstatement of Plan Agreement (Revised As of July 21, 2021)Cathylyn LacadinNo ratings yet
- Pharmacology Drug Study: Ivermectin and RemdesivirDocument4 pagesPharmacology Drug Study: Ivermectin and RemdesivirMa. Kaile Shyla Llacar100% (1)
- The Hemoglobin E Thalassemias: Correspondence: Grsfc@mahidol - Ac.thDocument15 pagesThe Hemoglobin E Thalassemias: Correspondence: Grsfc@mahidol - Ac.thDrAstha GuptaNo ratings yet
- Gesc 107Document12 pagesGesc 107Nippu SharmaNo ratings yet
- اسئلة تمريض شاملDocument116 pagesاسئلة تمريض شاملAmin TahaNo ratings yet
- Orbital Disease Diagnostic ImagingDocument11 pagesOrbital Disease Diagnostic ImagingFebeNo ratings yet
- Who Pen 2020Document85 pagesWho Pen 2020Faye PalmaresNo ratings yet
- Hemodynamics E-ConDocument1 pageHemodynamics E-ConpjebinkNo ratings yet
- 9700 s13 QP 11Document16 pages9700 s13 QP 11Joyce GohNo ratings yet
- Types of Auto ImmuneDocument3 pagesTypes of Auto ImmuneEdgar PunoNo ratings yet
- Pharma ExamDocument5 pagesPharma ExamMclavin LoveNo ratings yet