You might also like
- Etp - 30 KLDDocument18 pagesEtp - 30 KLDsubramanyam kumarNo ratings yet
- Boq For Electrification Works: Project: Plot Development at Dodderi BOQ For External Electrical ServicesDocument17 pagesBoq For Electrification Works: Project: Plot Development at Dodderi BOQ For External Electrical ServicespavanNo ratings yet
- Rational Formula Q 10 C I A Area MM/HR Hectre Hectre Q 62.3732 Cum/hr Lps Pump HP Calculation PumpDocument4 pagesRational Formula Q 10 C I A Area MM/HR Hectre Hectre Q 62.3732 Cum/hr Lps Pump HP Calculation PumpBanerjee SuvranilNo ratings yet
- Pump Head CalculationDocument2 pagesPump Head Calculationkenoly123No ratings yet
- 02 Design Based Report - 20140130Document133 pages02 Design Based Report - 20140130vinaygvm0% (1)
- TS Nit N0 578Document328 pagesTS Nit N0 578naveen prasadNo ratings yet
- List of Electrical Standard Specifications: Power Control Centres, Motor Control Centres Document STD002.U07 1/33 Rev. ADocument33 pagesList of Electrical Standard Specifications: Power Control Centres, Motor Control Centres Document STD002.U07 1/33 Rev. Avaithy1990No ratings yet
- Water Treatment CatalogueDocument12 pagesWater Treatment CatalogueJim TsikasNo ratings yet
- Booster Brochure 4-12Document2 pagesBooster Brochure 4-12Sam Wing HongNo ratings yet
- DBRDocument13 pagesDBRpsjjoshiNo ratings yet
- VRV Electrical RequirementDocument6 pagesVRV Electrical RequirementShrenikShahNo ratings yet
- Water Distribution ManualDocument20 pagesWater Distribution ManualOxfamNo ratings yet
- 01-2021-02-15 - EL - RES - Ato Mamush Plumbing Services Design ReportDocument15 pages01-2021-02-15 - EL - RES - Ato Mamush Plumbing Services Design Reportdawitggg0% (1)
- Mechanical CommentsDocument6 pagesMechanical Commentspsn_kylmNo ratings yet
- DBR Imphal AirportDocument24 pagesDBR Imphal AirportCreative GroupNo ratings yet
- ENGGBOQEstimation ReportDocument266 pagesENGGBOQEstimation ReportUTTAL RAYNo ratings yet
- Sizing of Busbar Trunking Systems (Busways) - Electrical Installation GuideDocument2 pagesSizing of Busbar Trunking Systems (Busways) - Electrical Installation GuideENGMNo ratings yet
- TAC Vs NFPADocument4 pagesTAC Vs NFPAS.KAMBAN50% (2)
- IIT Works 02-09-2019 For Electrical ServicesDocument23 pagesIIT Works 02-09-2019 For Electrical ServicesYaduveerSinghNo ratings yet
- TSKII Series: In-Line Centrifugal Duct FanDocument4 pagesTSKII Series: In-Line Centrifugal Duct FanKarin Aca Ovi100% (1)
- LC1 - C2001-33BQ-0000 - Pump Room - Rev01Document111 pagesLC1 - C2001-33BQ-0000 - Pump Room - Rev01suheil samaraNo ratings yet
- Busbar RatingsDocument1 pageBusbar RatingsRa ArNo ratings yet
- 01 Appd SPSCLT Piller Drawings 28-04-2010Document41 pages01 Appd SPSCLT Piller Drawings 28-04-2010cayunk7145No ratings yet
- Gland SelectionDocument8 pagesGland SelectionJignesh ParmarNo ratings yet
- BOQ Gas PipingDocument2 pagesBOQ Gas PipingAbu ZakaNo ratings yet
- Engineering 2Document4 pagesEngineering 2Tori SmallNo ratings yet
- 1-Sanitary Drainage SystemsDocument20 pages1-Sanitary Drainage Systemsraja bharathiNo ratings yet
- Bill of Quantites: Development of The Beach From Nishan-E-Pakistan To Chunky Munkey Phase - V Ext. Dha KarachiDocument54 pagesBill of Quantites: Development of The Beach From Nishan-E-Pakistan To Chunky Munkey Phase - V Ext. Dha KarachiHaji ManshaNo ratings yet
- Design and Practice of District CoolingDocument2 pagesDesign and Practice of District CoolingPhi Mac100% (1)
- City Gas Distribution Project in East & West Godavari Districts of Andhra PradeshDocument11 pagesCity Gas Distribution Project in East & West Godavari Districts of Andhra PradeshAnil KumAr MoteNo ratings yet
- Cold Water Tank (Plumbing)Document3 pagesCold Water Tank (Plumbing)Jin FongNo ratings yet
- How To Calculate Water Pump Horsepower - 14 Steps (With Pictures)Document3 pagesHow To Calculate Water Pump Horsepower - 14 Steps (With Pictures)ren salazarNo ratings yet
- Abstract of CPWDDocument5 pagesAbstract of CPWDabhishek kumarNo ratings yet
- Grundfos CRE BrochureDocument2 pagesGrundfos CRE BrochureGrundfosEgyptNo ratings yet
- Is 13039 External Fire HydrantDocument10 pagesIs 13039 External Fire HydrantNanu PatelNo ratings yet
- Metric Handbook Planning AND Design Data: Edited by David AdlerDocument12 pagesMetric Handbook Planning AND Design Data: Edited by David AdlerBachir lejlifaNo ratings yet
- Switchgear Selection ChartsDocument6 pagesSwitchgear Selection Chartsirfanbaig36No ratings yet
- Yazd-System Description For Clean Drain System PDFDocument7 pagesYazd-System Description For Clean Drain System PDFace-winnieNo ratings yet
- Water DemandDocument9 pagesWater Demandraveena athiNo ratings yet
- Questions STPDocument22 pagesQuestions STPRabindra SinghNo ratings yet
- Star-Delta Starter: Electrical Notes & ArticlesDocument25 pagesStar-Delta Starter: Electrical Notes & Articlesprabhanshu241991100% (1)
- Schedule For Ordinary Hazard OccupanciesDocument1 pageSchedule For Ordinary Hazard OccupanciesMostafa El-BalashonyNo ratings yet
- Fire Fighting Pumps: FeaturesDocument3 pagesFire Fighting Pumps: FeaturesReyza Prasetyo100% (1)
- Air RecieverDocument9 pagesAir RecieverMichael Belmonte UrdanetaNo ratings yet
- Annex A Requirement Specs - HVLS Fan 20 Feb FinalDocument3 pagesAnnex A Requirement Specs - HVLS Fan 20 Feb FinalJia WenjieNo ratings yet
- Design Calculation Sheet: System Class Class A Class B Class C Class D Class E Class FDocument3 pagesDesign Calculation Sheet: System Class Class A Class B Class C Class D Class E Class FMohd Najeeb Ali FathaanNo ratings yet
- Calculate Size of Ventilation FanDocument3 pagesCalculate Size of Ventilation Fanhusnainyasir100% (2)
- Method of Statement - R1 PDFDocument49 pagesMethod of Statement - R1 PDFMohamed YoussifNo ratings yet
- Specifications For Motor Control CentersDocument5 pagesSpecifications For Motor Control CentersNATHANNo ratings yet
- Banglore STP Flow ChartDocument8 pagesBanglore STP Flow Chartrajesh kandimalla100% (1)
- Presentation PerlisDocument40 pagesPresentation PerlishermanNo ratings yet
- Design of PlumbingDocument2 pagesDesign of PlumbingMukesh KumarNo ratings yet
- Car Park Extract CalculationDocument5 pagesCar Park Extract CalculationShivraj SawantNo ratings yet
- Is 3076Document18 pagesIs 3076Sathish KumarNo ratings yet
- MEP Work PresentationDocument6 pagesMEP Work PresentationdavethiyaguNo ratings yet
- Room ACis.1391.2.1992Document36 pagesRoom ACis.1391.2.1992Ajay MenonNo ratings yet
- 800 KLD STPDocument8 pages800 KLD STPsubramanyam kumarNo ratings yet
- Design Report (Public Health)Document10 pagesDesign Report (Public Health)subramanyam kumarNo ratings yet
- Design Report (Public Health)Document10 pagesDesign Report (Public Health)subramanyam kumarNo ratings yet
- Bill of Quantities: Project: Sewage Treatment Plant (0.90 MLD) Location: Pochampally Consultant: Mep ConsultantDocument7 pagesBill of Quantities: Project: Sewage Treatment Plant (0.90 MLD) Location: Pochampally Consultant: Mep Consultantsubramanyam kumarNo ratings yet
- Soil ReportDocument10 pagesSoil Reportsubramanyam kumarNo ratings yet
- Filter Media Data 1 A-40 MM Gradation: Applicable Municipal Area AllowanceDocument2 pagesFilter Media Data 1 A-40 MM Gradation: Applicable Municipal Area Allowancesubramanyam kumarNo ratings yet
- WTP& Collection WellDocument431 pagesWTP& Collection Wellsubramanyam kumarNo ratings yet
- Terrace Main Dom Kadapa SSDocument5 pagesTerrace Main Dom Kadapa SSsubramanyam kumarNo ratings yet
- Sump .XLS (7.00 Lakhs)Document58 pagesSump .XLS (7.00 Lakhs)subramanyam kumarNo ratings yet
- S.S.Consultants: Advance Copy For Planning PurposeDocument1 pageS.S.Consultants: Advance Copy For Planning Purposesubramanyam kumarNo ratings yet
- Final Fire FightingDocument402 pagesFinal Fire Fightingsubramanyam kumarNo ratings yet
- Sump .Xls (7.00 Lakhs) - 1Document38 pagesSump .Xls (7.00 Lakhs) - 1subramanyam kumarNo ratings yet
- Crack - Water Tank - Wall (1.50 Lakhs)Document4 pagesCrack - Water Tank - Wall (1.50 Lakhs)subramanyam kumarNo ratings yet
- Sump .XLS (1.50 Lakhs)Document55 pagesSump .XLS (1.50 Lakhs)subramanyam kumarNo ratings yet
- Sump .XLS (2.00 Lakhs)Document35 pagesSump .XLS (2.00 Lakhs)subramanyam kumarNo ratings yet
- S.S.Consultants: Advance Copy For Planning PurposeDocument1 pageS.S.Consultants: Advance Copy For Planning Purposesubramanyam kumarNo ratings yet
- Sump .Xls (1.00 Lakhs) - 1Document35 pagesSump .Xls (1.00 Lakhs) - 1subramanyam kumarNo ratings yet
- Arch Ad 16Document1 pageArch Ad 16subramanyam kumarNo ratings yet
- Sump .XLS (2.00 Lakhs)Document35 pagesSump .XLS (2.00 Lakhs)subramanyam kumarNo ratings yet
- S.S.Consultants: Advance Copy For Planning PurposeDocument1 pageS.S.Consultants: Advance Copy For Planning Purposesubramanyam kumarNo ratings yet
- Arch Ad 19Document1 pageArch Ad 19subramanyam kumarNo ratings yet
- Arch Ad 17Document1 pageArch Ad 17subramanyam kumarNo ratings yet
- Super Speciality Hospital, Kadapa (10.08.2020)Document799 pagesSuper Speciality Hospital, Kadapa (10.08.2020)subramanyam kumarNo ratings yet
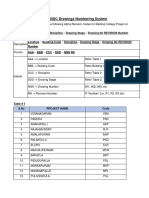
- Drawings Numbering SystemDocument2 pagesDrawings Numbering Systemsubramanyam kumarNo ratings yet
- List of Arch DrawingsDocument9 pagesList of Arch Drawingssubramanyam kumarNo ratings yet
- STP - 130 KLDDocument27 pagesSTP - 130 KLDsubramanyam kumarNo ratings yet