You might also like
- The Four Common Types of Parenting StylesDocument11 pagesThe Four Common Types of Parenting StylesIka_Dyah_Purwa_1972100% (3)
- 2023 Calendar Printable For KidsDocument13 pages2023 Calendar Printable For KidsAMY LALRINGHLUANI M.Sc. Child Health (Paediatric ) NursingNo ratings yet
- Orthopedic Inpatient Protocols: A Guide to Orthopedic Inpatient RoundingFrom EverandOrthopedic Inpatient Protocols: A Guide to Orthopedic Inpatient RoundingNo ratings yet
- Blood Component TherapyDocument73 pagesBlood Component TherapySaikat Prasad DattaNo ratings yet
- BLOOD TRANSFUSION NotesDocument7 pagesBLOOD TRANSFUSION NotesErl D. MelitanteNo ratings yet
- Blood TransfusionDocument36 pagesBlood TransfusionRonan Reyno100% (1)
- BX10/BX10 MB: Weighing Terminals Technical ManualDocument60 pagesBX10/BX10 MB: Weighing Terminals Technical Manualfelipezambrano50% (2)
- Blood and Blood Components-LectureDocument12 pagesBlood and Blood Components-LectureSj EclipseNo ratings yet
- Blood and Blood Components-LectureDocument13 pagesBlood and Blood Components-LectureMelissa GinesNo ratings yet
- Blood Groups, Blood Components, Blood Transfusion PresentationDocument50 pagesBlood Groups, Blood Components, Blood Transfusion PresentationAashish Gautam100% (1)
- Jsa-0002 - CCTV Pipe Inspection RapidDocument8 pagesJsa-0002 - CCTV Pipe Inspection RapidMohamad AfifNo ratings yet
- Pediatric Hematology Oncology Ward Officer HandbookDocument40 pagesPediatric Hematology Oncology Ward Officer HandbookAnonymous FSUnLYr4yNo ratings yet
- Transfusion of Blood & Blood Components1Document45 pagesTransfusion of Blood & Blood Components1Chamika Huruggamuwa100% (1)
- Care For Hemodialysis Patients: Pre, During, Post Dialysis CareDocument18 pagesCare For Hemodialysis Patients: Pre, During, Post Dialysis CareHemanth PrakashNo ratings yet
- Blood & Blood Products GuideDocument52 pagesBlood & Blood Products Guidewellawalalasith100% (1)
- Community-Based Forest ManagementDocument7 pagesCommunity-Based Forest ManagementZiazel ThereseNo ratings yet
- IV-THERAPY-Blood TransfusionDocument40 pagesIV-THERAPY-Blood TransfusionShiena Mae PelagioNo ratings yet
- Guidance and CounselingDocument16 pagesGuidance and CounselingAMY LALRINGHLUANI M.Sc. Child Health (Paediatric ) NursingNo ratings yet
- BT New TemplateDocument65 pagesBT New TemplateNikky SilvestreNo ratings yet
- Blood TransfusionDocument29 pagesBlood TransfusionNonu Kims100% (1)
- Blood TransfusionDocument25 pagesBlood Transfusionpriya9balan-863873No ratings yet
- Blood TransfusionDocument55 pagesBlood Transfusionanand7504100% (2)
- Wardclass Powerpoint Blood TransfusionDocument27 pagesWardclass Powerpoint Blood TransfusionKatherine 'Chingboo' Leonico Laud60% (5)
- Neonatal Exchange Transfusion (Neonatal)Document8 pagesNeonatal Exchange Transfusion (Neonatal)Muhammad ShahbazNo ratings yet
- 12.intraoperative Fluid ManagmentDocument54 pages12.intraoperative Fluid ManagmentyeabsraNo ratings yet
- Blood TransfusionDocument52 pagesBlood TransfusionAnonymous GC8uMx367% (3)
- Exchange TransfusionDocument21 pagesExchange TransfusionJOSLIN100% (2)
- Neonatal Exchange TransfusionDocument33 pagesNeonatal Exchange TransfusionedrinsneNo ratings yet
- Exchange TransfusionDocument35 pagesExchange Transfusionsobinjohnpkl100% (2)
- Exhange TransfusionDocument50 pagesExhange Transfusionjulie kiskuNo ratings yet
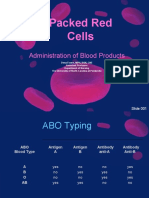
- Packed Red Cells: Administration of Blood ProductsDocument36 pagesPacked Red Cells: Administration of Blood ProductsRj SantosNo ratings yet
- BloodDocument49 pagesBloodvruttika parmar100% (3)
- Blood Components and Blood TransfusionDocument38 pagesBlood Components and Blood TransfusionjosephNo ratings yet
- Neonatal Exchange Transfusion GuideDocument9 pagesNeonatal Exchange Transfusion GuidedewpraNo ratings yet
- Blood TransfusionDocument39 pagesBlood Transfusiongoyabeb59No ratings yet
- Hematology Resident Guide to Blood Component TransfusionDocument49 pagesHematology Resident Guide to Blood Component TransfusionZel Azuro SolisNo ratings yet
- Transfusion Medicine OverviewDocument40 pagesTransfusion Medicine OverviewmonichaNo ratings yet
- Blood transfusionDocument20 pagesBlood transfusionGladys OdibuNo ratings yet
- Pediatric Hematology Oncology Ward Officer HandbookDocument40 pagesPediatric Hematology Oncology Ward Officer HandbookLetchumana KrishnanNo ratings yet
- IV Therapy SlidesDocument8 pagesIV Therapy SlidesRegean MercadoNo ratings yet
- Upper GI BleedDocument50 pagesUpper GI BleedNiladri BanerjeeNo ratings yet
- Blood Component Therapy F17Document33 pagesBlood Component Therapy F17Crystal LynaeNo ratings yet
- Principles of Blood Transfusion 2Document21 pagesPrinciples of Blood Transfusion 2dhivya singhNo ratings yet
- Blood Transfusion TherapyDocument38 pagesBlood Transfusion TherapyAnn Merlin JobinNo ratings yet
- Advanced Clinical Pharmacology Jan 2009Document51 pagesAdvanced Clinical Pharmacology Jan 2009kylietanglsNo ratings yet
- Blood Transfusion Therapy DefinitionDocument27 pagesBlood Transfusion Therapy DefinitionEvangelin MelvinNo ratings yet
- Blood Grouping and BankingDocument41 pagesBlood Grouping and BankingChipego NyirendaNo ratings yet
- Comprehensive Nursing Care in Hematopoietic Stem Cell TransplantationDocument47 pagesComprehensive Nursing Care in Hematopoietic Stem Cell TransplantationRajani Singh BaghelNo ratings yet
- Blood Transfusion Complications & Management (40Document30 pagesBlood Transfusion Complications & Management (40kushalNo ratings yet
- Preop Postop Paeds Surgical - Fluid MsnsgementDocument64 pagesPreop Postop Paeds Surgical - Fluid MsnsgementDiyana ZatyNo ratings yet
- Anaesthetic Management in Obstetric Haemorrhage: DR B.Srikanth Iindyrpg Dept. of AnaesthesiaDocument34 pagesAnaesthetic Management in Obstetric Haemorrhage: DR B.Srikanth Iindyrpg Dept. of AnaesthesiaEDI CNo ratings yet
- Blood TransfusionDocument65 pagesBlood TransfusionKate Lucernas MayugaNo ratings yet
- Rational Use of Blood ComponentsDocument43 pagesRational Use of Blood ComponentsMohandoss MurugesanNo ratings yet
- Blood TransfusionDocument18 pagesBlood TransfusionJeeduu frostNo ratings yet
- 11 Peri Operative CareDocument43 pages11 Peri Operative CareAdnan MaqboolNo ratings yet
- Blood Transfusion: Presented To: Sir Khurram AshfaqDocument33 pagesBlood Transfusion: Presented To: Sir Khurram AshfaqIJAZ HUSSAINNo ratings yet
- PPDS Rev 20 Jan 2019Document54 pagesPPDS Rev 20 Jan 2019Radinal MauludiNo ratings yet
- Blood Transfusion Guidelines for NICU BabiesDocument8 pagesBlood Transfusion Guidelines for NICU BabiesanuNo ratings yet
- Transfusion of Blood and Red CellsDocument34 pagesTransfusion of Blood and Red CellsAdams Westlifer SophianoNo ratings yet
- Peritoneal Dialysis (chronic) and Prescription in childrenDocument26 pagesPeritoneal Dialysis (chronic) and Prescription in childrenAnkit ManglaNo ratings yet
- BLOOD TRANSFUSION GUIDEDocument75 pagesBLOOD TRANSFUSION GUIDEKamal SaudNo ratings yet
- PolycythemiaDocument3 pagesPolycythemiaAdhil LuttooNo ratings yet
- 145 278 1 SMDocument28 pages145 278 1 SMAtika RosmiaNo ratings yet
- Blood TransfusionDocument27 pagesBlood TransfusionreynoldNo ratings yet
- Blood AdministrationDocument35 pagesBlood AdministrationnurminieNo ratings yet
- Surgical Practice For Infantile Hypertrophic PylorDocument5 pagesSurgical Practice For Infantile Hypertrophic PylorAMY LALRINGHLUANI M.Sc. Child Health (Paediatric ) NursingNo ratings yet
- Colostomy Care Tips for Pediatric PatientsDocument4 pagesColostomy Care Tips for Pediatric PatientsAMY LALRINGHLUANI M.Sc. Child Health (Paediatric ) NursingNo ratings yet
- Ospe & Osce-1Document9 pagesOspe & Osce-1AMY LALRINGHLUANI M.Sc. Child Health (Paediatric ) NursingNo ratings yet
- Evaluation of student performanceDocument11 pagesEvaluation of student performanceAMY LALRINGHLUANI M.Sc. Child Health (Paediatric ) NursingNo ratings yet
- Visit Report On ICUDocument8 pagesVisit Report On ICUAMY LALRINGHLUANI M.Sc. Child Health (Paediatric ) NursingNo ratings yet
- It Always Seems Impo!ible Un"l It's Done. Dream Big!: January 2022Document12 pagesIt Always Seems Impo!ible Un"l It's Done. Dream Big!: January 2022AMY LALRINGHLUANI M.Sc. Child Health (Paediatric ) NursingNo ratings yet
- Class TeachersDocument2 pagesClass TeachersAMY LALRINGHLUANI M.Sc. Child Health (Paediatric ) NursingNo ratings yet
- Models of PreventionDocument25 pagesModels of PreventionAMY LALRINGHLUANI M.Sc. Child Health (Paediatric ) NursingNo ratings yet
- Vancouver Citation Style Guide: Book-Single Author/EditorDocument3 pagesVancouver Citation Style Guide: Book-Single Author/EditorAMY LALRINGHLUANI M.Sc. Child Health (Paediatric ) NursingNo ratings yet
- Pictorial Guide On Biomedical Waste Management Rules 2016: (AMENDED IN 2018 & 2019)Document23 pagesPictorial Guide On Biomedical Waste Management Rules 2016: (AMENDED IN 2018 & 2019)Ravi BhatraNo ratings yet
- ANIMAL BEHAVIOR SCIENCEDocument37 pagesANIMAL BEHAVIOR SCIENCEZ AlbertNo ratings yet
- STD Comparison ChartDocument4 pagesSTD Comparison Chartabu ubaidahNo ratings yet
- 1619928348861forensic Science UNIT - VII 1 PDFDocument159 pages1619928348861forensic Science UNIT - VII 1 PDFVyshnav RNo ratings yet
- RR No. 6-2015 PDFDocument5 pagesRR No. 6-2015 PDFErlene CompraNo ratings yet
- The Suitcase ProjectDocument27 pagesThe Suitcase Projectshubhamkumar9211No ratings yet
- D1553.140U1 German Braun Speed - Braun Card-Xi'an Yuanhua Instrument Co., LTDDocument2 pagesD1553.140U1 German Braun Speed - Braun Card-Xi'an Yuanhua Instrument Co., LTDTrong Hung NguyenNo ratings yet
- HN E-Catalog CableDocument36 pagesHN E-Catalog CableMin Min AungNo ratings yet
- Flame Amplifier HoneywellDocument8 pagesFlame Amplifier Honeywellgavo vargoNo ratings yet
- BInggrisDocument19 pagesBInggrisanwar318No ratings yet
- Smart medical system monitors dementia patients' medicationDocument9 pagesSmart medical system monitors dementia patients' medicationKresnaNo ratings yet
- A Study On Satisfaction Level of Employees With Special Reference Textile IndustryDocument12 pagesA Study On Satisfaction Level of Employees With Special Reference Textile Industrysai kiran bade100% (1)
- Moisture Sorption Isotherms Characteristics of Food ProductsDocument10 pagesMoisture Sorption Isotherms Characteristics of Food ProductsMustapha Bello50% (2)
- Facilitating Civic Engagement Through Consultation: Learning From Local Communities Through The NHI-Accountability Project in South AfricaDocument64 pagesFacilitating Civic Engagement Through Consultation: Learning From Local Communities Through The NHI-Accountability Project in South AfricaOxfamNo ratings yet
- English Try Out UN 1 2008/2009Document4 pagesEnglish Try Out UN 1 2008/2009Cepiana Abas100% (10)
- India TodayDocument76 pagesIndia TodaySanket RaveendraNo ratings yet
- Shall We Date Obey Me! - Works Archive of Our OwnDocument1 pageShall We Date Obey Me! - Works Archive of Our OwnEdyn LaiNo ratings yet
- Kshitija's ResumeDocument1 pageKshitija's ResumeNavinNo ratings yet
- Ecl7000 enDocument2 pagesEcl7000 ensuchaya tupyangNo ratings yet
- Section - A: Holiday Homework For Grade XiDocument7 pagesSection - A: Holiday Homework For Grade XiGM Ali KawsarNo ratings yet
- Low Noise Pseudomorphic HEMT Technical DataDocument4 pagesLow Noise Pseudomorphic HEMT Technical Datahendpraz88No ratings yet
- Nikola Tesla Would Have Celebrated Christmas On January 7thDocument3 pagesNikola Tesla Would Have Celebrated Christmas On January 7thAnonymous DfeajF100% (1)
- Manual Book IOG ConventionDocument17 pagesManual Book IOG ConventionTaufiq MaulanaNo ratings yet
- Formula 1480 Rub Off Mask PDFDocument1 pageFormula 1480 Rub Off Mask PDFAbdul WasayNo ratings yet
- Honey & Bee Product Recipes: November 2007Document29 pagesHoney & Bee Product Recipes: November 2007Kyra ThomasNo ratings yet
- Veterinarian Careers Projected Strong GrowthDocument6 pagesVeterinarian Careers Projected Strong Growthnmann7100% (1)
- BC-5300 Preventive Maintenance Kit ManualDocument8 pagesBC-5300 Preventive Maintenance Kit ManualAbdel MUNDENNo ratings yet