You might also like
- Atls Important Notes Triage: Ali M. Ahmad Consultant Pediatric SurgeryDocument55 pagesAtls Important Notes Triage: Ali M. Ahmad Consultant Pediatric SurgeryAndris TapaNo ratings yet
- Cell SignalingDocument38 pagesCell SignalingShyrene Mamanao GumbanNo ratings yet
- Science 4 Module 1 Q2Document27 pagesScience 4 Module 1 Q2Lady Bielle Horcerada100% (3)
- Blood and Blood Components-LectureDocument12 pagesBlood and Blood Components-LectureSj EclipseNo ratings yet
- BLOOD TRANSFUSION NotesDocument7 pagesBLOOD TRANSFUSION NotesErl D. MelitanteNo ratings yet
- Blood Component TherapyDocument73 pagesBlood Component TherapySaikat Prasad DattaNo ratings yet
- Blood DonationsDocument6 pagesBlood DonationsCHIPapiNo ratings yet
- Tissue-Specific MetabolismDocument35 pagesTissue-Specific MetabolismLulu100% (2)
- Blood TransfusionDocument55 pagesBlood Transfusionanand7504100% (2)
- Wardclass Powerpoint Blood TransfusionDocument27 pagesWardclass Powerpoint Blood TransfusionKatherine 'Chingboo' Leonico Laud60% (5)
- Transfusion of Blood & Blood Components1Document45 pagesTransfusion of Blood & Blood Components1Chamika Huruggamuwa100% (1)
- Blood Banks and Blood GroupingDocument75 pagesBlood Banks and Blood GroupingAbhinav Bhattarai100% (1)
- Blood TransfusionDocument58 pagesBlood Transfusionmsat72100% (12)
- Blood Transfusion PocedureDocument9 pagesBlood Transfusion PocedureRaman Samrao100% (1)
- Blood & Blood ProductsDocument126 pagesBlood & Blood ProductsdrprasadingleyNo ratings yet
- 12.intraoperative Fluid ManagmentDocument54 pages12.intraoperative Fluid ManagmentyeabsraNo ratings yet
- IV-THERAPY-Blood TransfusionDocument40 pagesIV-THERAPY-Blood TransfusionShiena Mae PelagioNo ratings yet
- Blood TransfusionDocument52 pagesBlood TransfusionAnonymous GC8uMx367% (3)
- Blood TransfusionDocument36 pagesBlood TransfusionRonan Reyno100% (1)
- Blood and Blood Components-LectureDocument13 pagesBlood and Blood Components-LectureMelissa GinesNo ratings yet
- Blood TransfusionDocument29 pagesBlood TransfusionNonu Kims100% (1)
- Blood Basics1Document6 pagesBlood Basics1Celina PastorNo ratings yet
- Blood Groups, Blood Components, Blood Transfusion PresentationDocument50 pagesBlood Groups, Blood Components, Blood Transfusion PresentationAashish Gautam100% (1)
- Exchange TransfusionDocument21 pagesExchange TransfusionJOSLIN100% (3)
- BT New TemplateDocument65 pagesBT New TemplateNikky SilvestreNo ratings yet
- Blood Transfusion ClassDocument61 pagesBlood Transfusion ClassshikhaNo ratings yet
- Blood BankDocument43 pagesBlood BanksatnamNo ratings yet
- Blood TransfusionDocument47 pagesBlood TransfusionVaishnavi BingumallaNo ratings yet
- Blood Component Therapy F17Document33 pagesBlood Component Therapy F17Crystal LynaeNo ratings yet
- Exhange TransfusionDocument50 pagesExhange Transfusionjulie kiskuNo ratings yet
- Blood TransfusionDocument65 pagesBlood TransfusionKate Lucernas MayugaNo ratings yet
- BloodDocument49 pagesBloodvruttika parmar100% (3)
- Exchange TRX 2011-13Document3 pagesExchange TRX 2011-13AMY LALRINGHLUANI M.Sc. Child Health (Paediatric ) NursingNo ratings yet
- Principles of Blood Transfusion 2Document21 pagesPrinciples of Blood Transfusion 2dhivya singhNo ratings yet
- Blood TransfusionDocument20 pagesBlood TransfusionRaymund Christopher Dela PeñaNo ratings yet
- Blood TransfusionDocument32 pagesBlood TransfusionDrPreeti Thakur ChouhanNo ratings yet
- Blood TransfusionDocument48 pagesBlood TransfusionABARNA ABINo ratings yet
- Surgery of Kidney Ureter and VaricoseDocument55 pagesSurgery of Kidney Ureter and VaricoseSaurabh SharmaNo ratings yet
- Transfusi DarahDocument29 pagesTransfusi Darahanggie pratiwiNo ratings yet
- Blood Grouping and BankingDocument41 pagesBlood Grouping and BankingChipego NyirendaNo ratings yet
- Lecture 5 Blood Bank: Blood Donors, Blood Collection & StorageDocument19 pagesLecture 5 Blood Bank: Blood Donors, Blood Collection & StorageMarl EstradaNo ratings yet
- Blood DonationDocument76 pagesBlood Donationlanie_bluegirl100% (1)
- Blood TransfusionDocument20 pagesBlood TransfusionGladys OdibuNo ratings yet
- Blood Transfusion in ObstetricsDocument8 pagesBlood Transfusion in ObstetricsLubna TahaNo ratings yet
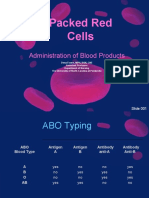
- Packed Red Cells: Administration of Blood ProductsDocument36 pagesPacked Red Cells: Administration of Blood ProductsRj SantosNo ratings yet
- PPDS Rev 20 Jan 2019Document54 pagesPPDS Rev 20 Jan 2019Radinal MauludiNo ratings yet
- Blood Transuation AssignmentDocument6 pagesBlood Transuation AssignmentvimajavNo ratings yet
- Blood Transfusion - Megha SoniDocument29 pagesBlood Transfusion - Megha SoniMegha VadanereNo ratings yet
- Transfusion2,0 PDFDocument13 pagesTransfusion2,0 PDFAngry FinnNo ratings yet
- Rationale: Most Patients Prescribed To Receive Platelet Transfusions Exhibit Moderate ToDocument2 pagesRationale: Most Patients Prescribed To Receive Platelet Transfusions Exhibit Moderate TojoanneNo ratings yet
- Blood TransfussionDocument51 pagesBlood TransfussionAllyssa Leila Estrebillo OrbeNo ratings yet
- Blood Component Transfusion: 1st Year Pediatric ResidentDocument49 pagesBlood Component Transfusion: 1st Year Pediatric ResidentZel Azuro SolisNo ratings yet
- Blood TransfusionDocument57 pagesBlood Transfusionibzshan_No ratings yet
- Blood Transfusion: Prepared By: Salar N. SulaimanDocument45 pagesBlood Transfusion: Prepared By: Salar N. SulaimanJoanne Bernadette AguilarNo ratings yet
- Hematologic DisorderDocument16 pagesHematologic DisorderZoe DorothyNo ratings yet
- Transfusion Medicine:: Types, Indications and ComplicationsDocument40 pagesTransfusion Medicine:: Types, Indications and ComplicationsmonichaNo ratings yet
- Types, Indications and Complications: TransfusionDocument26 pagesTypes, Indications and Complications: TransfusionVatha NaNo ratings yet
- Blood Transfusion TherapyDocument38 pagesBlood Transfusion TherapyAnn Merlin JobinNo ratings yet
- Blood Transfusion IIDocument20 pagesBlood Transfusion IIRaymund Christopher Dela PeñaNo ratings yet
- Blood Transfusion 1Document8 pagesBlood Transfusion 1KMNo ratings yet
- Blood TransfusionDocument31 pagesBlood TransfusionMilagros Florita100% (1)
- Blood Transfusion PDFDocument7 pagesBlood Transfusion PDFBaboolal100% (2)
- Blood TransfusionDocument18 pagesBlood TransfusionJeeduu frostNo ratings yet
- General and Specific Problems in Reproduction and SexualityDocument3 pagesGeneral and Specific Problems in Reproduction and Sexualitygoyabeb59No ratings yet
- Pediatric Patient ProblemsDocument85 pagesPediatric Patient Problemsgoyabeb59No ratings yet
- PROCEDURES IN VITAL SIGNS With RationaleDocument3 pagesPROCEDURES IN VITAL SIGNS With Rationalegoyabeb59No ratings yet
- Social Media in The Connected AgeDocument3 pagesSocial Media in The Connected Agegoyabeb59No ratings yet
- Sustainable Development Goals 2Document16 pagesSustainable Development Goals 2goyabeb59No ratings yet
- CatheterizationDocument42 pagesCatheterizationgoyabeb59No ratings yet
- Anti Hepatic FailureDocument4 pagesAnti Hepatic Failuregoyabeb59No ratings yet
- Brgy. Rapu Rapu Article ReviewDocument1 pageBrgy. Rapu Rapu Article Reviewgoyabeb59No ratings yet
- ALF (Acute Liver Failure) Concept MapDocument1 pageALF (Acute Liver Failure) Concept Mapgoyabeb59No ratings yet
- Altered Body TemperatureDocument10 pagesAltered Body TemperatureMelvin VrNo ratings yet
- Pages From 5090 - w11 - QP - 22Document1 pagePages From 5090 - w11 - QP - 22Abrar JawadNo ratings yet
- Exsc 223 CH 9 Practice ExamDocument8 pagesExsc 223 CH 9 Practice Examkimber brownNo ratings yet
- A KAP Study On The Quality of Sleep and Complications of Patients With Type 2 Diabetes MellitusDocument3 pagesA KAP Study On The Quality of Sleep and Complications of Patients With Type 2 Diabetes MellitusInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Apnea of Prematurity: UnderstandingDocument2 pagesApnea of Prematurity: UnderstandingEmil JaniakNo ratings yet
- Tutorial: MODULE: Cardiovascular System IIDocument3 pagesTutorial: MODULE: Cardiovascular System IIrishit100% (1)
- Jurnal AnestesiDocument5 pagesJurnal AnestesiridwanNo ratings yet
- Intro To Ana Physio RBLDocument69 pagesIntro To Ana Physio RBLHades HadesNo ratings yet
- US Military Study in HypothermiaDocument29 pagesUS Military Study in HypothermiaGeorgi GeorgievNo ratings yet
- Stroke Script - ABACDocument6 pagesStroke Script - ABACLee AndrewNo ratings yet
- Ion ChannelsDocument17 pagesIon ChannelsFrancia ToledanoNo ratings yet
- Crop Production MCQDocument31 pagesCrop Production MCQNsengimanaNo ratings yet
- PT Cakra Medika Utama: Price List Boditech Med Inc (I-Chroma)Document2 pagesPT Cakra Medika Utama: Price List Boditech Med Inc (I-Chroma)raditNo ratings yet
- Acharya Nagarjuna University:: Nagarjuna Nagar - 522 510, A.P., IndiaDocument9 pagesAcharya Nagarjuna University:: Nagarjuna Nagar - 522 510, A.P., IndiaShankar Reddy ChNo ratings yet
- G9 Science Q1 - Week 1-2 Respiratory-Circulatory-SystemDocument34 pagesG9 Science Q1 - Week 1-2 Respiratory-Circulatory-SystemSandra Lee LigsaNo ratings yet
- PHARMA 06. Introduction To Autonomic PharmacologyDocument6 pagesPHARMA 06. Introduction To Autonomic PharmacologyCindy Mae MacamayNo ratings yet
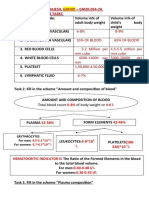
- Name - Soni Ritika Rajesh, Group - GM20-054-2A Physiology Week 03 TasksDocument10 pagesName - Soni Ritika Rajesh, Group - GM20-054-2A Physiology Week 03 TasksRitika SoniNo ratings yet
- Jurnal - Komponen DarahDocument6 pagesJurnal - Komponen Darahvivi maykasariNo ratings yet
- Aerobic Exercise On Increasing Endurance in Coronary Heart Disease Patients With 6MWT - Case StudyDocument6 pagesAerobic Exercise On Increasing Endurance in Coronary Heart Disease Patients With 6MWT - Case Studypriesha aprilia03No ratings yet
- Biology Unit 2 - Lesson 3 - Week 2Document3 pagesBiology Unit 2 - Lesson 3 - Week 2Daniel RoopchandNo ratings yet
- 4 - Acute Biologic CrisisDocument37 pages4 - Acute Biologic CrisisJek Dela CruzNo ratings yet
- Reviewer - Muscular SystemDocument11 pagesReviewer - Muscular SystemIvy Jan OcateNo ratings yet
- ETC Part Three Illustration AtfDocument1 pageETC Part Three Illustration Atfpnsscsny29No ratings yet
- Effect of Nadi Shuddhi Pranayama On Perceived Stress and Cardiovascular Autonomic Functions in 1st Year Undergraduate Medical StudentsDocument6 pagesEffect of Nadi Shuddhi Pranayama On Perceived Stress and Cardiovascular Autonomic Functions in 1st Year Undergraduate Medical StudentsBabuNo ratings yet
- Lab Manual - Human Heart - A+p - StudentDocument24 pagesLab Manual - Human Heart - A+p - Studentsyl0% (1)
- MCQDocument64 pagesMCQade winataNo ratings yet