You might also like
- How To Diagnose Autism: Anissa Nur AzmiDocument5 pagesHow To Diagnose Autism: Anissa Nur AzmiYeni ZeonNo ratings yet
- Poon2010 DDDocument8 pagesPoon2010 DDPoonam joshiNo ratings yet
- Therapist's Guide to Pediatric Affect and Behavior RegulationFrom EverandTherapist's Guide to Pediatric Affect and Behavior RegulationNo ratings yet
- Parents' Experiences of The Service Pathway To An Autism DiagnosisDocument8 pagesParents' Experiences of The Service Pathway To An Autism DiagnosisKarel GuevaraNo ratings yet
- Povećana Prevalencija AutizmaDocument4 pagesPovećana Prevalencija AutizmaJohn SmithNo ratings yet
- Ozonoff, 2015Document3 pagesOzonoff, 2015Susi RutmalemNo ratings yet
- Research Article: Parental Perceptions of A Manchester Service For Autistic Spectrum DisordersDocument7 pagesResearch Article: Parental Perceptions of A Manchester Service For Autistic Spectrum DisordersElian Y. Sanchez-RiveraNo ratings yet
- Clinical Evaluation in Autism Spectrum Disorders-With-Cover-Page-V2Document28 pagesClinical Evaluation in Autism Spectrum Disorders-With-Cover-Page-V2Vini RarcariNo ratings yet
- Diagnosis and Treatment of Children With Autism Spectrum DisordersFrom EverandDiagnosis and Treatment of Children With Autism Spectrum DisordersRating: 5 out of 5 stars5/5 (1)
- Early Detection of Autism Spectrum Disorders: Screening Between 12 and 24 Months of AgeDocument10 pagesEarly Detection of Autism Spectrum Disorders: Screening Between 12 and 24 Months of AgeJose Alonso Aguilar ValeraNo ratings yet
- ASD Recovery 2019Document5 pagesASD Recovery 2019verdantlaw100% (1)
- O o o o O: Assessment For IdentificationDocument9 pagesO o o o O: Assessment For IdentificationJong Suk Joo (Shuru)No ratings yet
- Greenspan 2008Document5 pagesGreenspan 2008Jose Alonso Aguilar ValeraNo ratings yet
- AAP ASD Exec SummaryDocument7 pagesAAP ASD Exec SummaryCatherine AgustinNo ratings yet
- A Systematic Review of Predictors, Moderators, and Mediators of Augmentative and Alternative Communication (AAC) Outcomes For Children With Autism Spectrum DisorderDocument12 pagesA Systematic Review of Predictors, Moderators, and Mediators of Augmentative and Alternative Communication (AAC) Outcomes For Children With Autism Spectrum DisorderOrnella ThysNo ratings yet
- Early Detection of Developmental and Behavioral Problems: Pediatrics in Review September 2000Document10 pagesEarly Detection of Developmental and Behavioral Problems: Pediatrics in Review September 2000annaNo ratings yet
- Advances Autism PDFDocument892 pagesAdvances Autism PDFAndrea PuentesNo ratings yet
- Chen 2013Document8 pagesChen 2013RominaNo ratings yet
- American Academy of Pediatrics: Disorders, Fourth Edition Criteria 3) The Assessment ofDocument13 pagesAmerican Academy of Pediatrics: Disorders, Fourth Edition Criteria 3) The Assessment ofMatNo ratings yet
- Foreign RRSDocument2 pagesForeign RRSTheresa Mae PansaonNo ratings yet
- Parents of Children With ASD PDFDocument64 pagesParents of Children With ASD PDFmsyan1965No ratings yet
- Developmental ExaminationDocument15 pagesDevelopmental ExaminationDr. Nirbhay Mehta100% (1)
- 016 Developmental-Behavioral Screening and SurveillanceDocument13 pages016 Developmental-Behavioral Screening and SurveillanceMary KuklinaNo ratings yet
- 2019 - Changing Conceptualizations of Regression in Autism - OzonoffDocument9 pages2019 - Changing Conceptualizations of Regression in Autism - OzonoffJesus RiveraNo ratings yet
- Segundo 2019Document12 pagesSegundo 2019Thaís Spall ChaximNo ratings yet
- 2020 Delehanty Exploring Message Framing To Engage Parents in Early Screening For - CompressedDocument7 pages2020 Delehanty Exploring Message Framing To Engage Parents in Early Screening For - CompressedYolanda Gómez LópezNo ratings yet
- Robins M CHATDocument15 pagesRobins M CHATleonorcruz2314No ratings yet
- PMC7926898 AutismDocument13 pagesPMC7926898 AutismMageeNo ratings yet
- 2022 - Digital Medicine - Evaluation of An Artificial Intelligence-Based Medical Device For Diagnosis of Autism Spectrum DisorderDocument11 pages2022 - Digital Medicine - Evaluation of An Artificial Intelligence-Based Medical Device For Diagnosis of Autism Spectrum DisorderNeraLogoNo ratings yet
- Trayectorias de Desarrollo Lingüístico en Niños Con AutismoDocument9 pagesTrayectorias de Desarrollo Lingüístico en Niños Con AutismoNatalia Castro MartinezNo ratings yet
- Autism Risk in Very Preterm Infants-New Answers, More QuestionsDocument3 pagesAutism Risk in Very Preterm Infants-New Answers, More QuestionsPatricia BrucellariaNo ratings yet
- GRP7 Finalpaper FMDocument42 pagesGRP7 Finalpaper FMMorish Roi YacasNo ratings yet
- EvyDxen AutismoDocument9 pagesEvyDxen AutismocynthiaNo ratings yet
- Evaluation of The Child With Global Developmental DelayDocument14 pagesEvaluation of The Child With Global Developmental DelayplaincircleNo ratings yet
- Diagnosing Oppositional Defiant Disorder Using The AnxietyDocument9 pagesDiagnosing Oppositional Defiant Disorder Using The AnxietyCeeta QualityNo ratings yet
- Eye Tracking in Infants and Young Children PDFDocument22 pagesEye Tracking in Infants and Young Children PDFMH AmoueiNo ratings yet
- ADHD Guidance-September 2013Document6 pagesADHD Guidance-September 2013Claude JousselinNo ratings yet
- Autism As A Social Issue and Necessary Clinical Intervention ToolsDocument11 pagesAutism As A Social Issue and Necessary Clinical Intervention Toolstorontowriters7No ratings yet
- Barbaro & Dissanayake (2010) - SACS PDF FINAL PDFDocument10 pagesBarbaro & Dissanayake (2010) - SACS PDF FINAL PDFAnonymous 75M6uB3Ow100% (1)
- ESDMDocument9 pagesESDMVictória NamurNo ratings yet
- CitarDocument3 pagesCitarVictor NamurNo ratings yet
- Genetic Evaluation of Children With Global Developmental Delaydcurrent Status of Network Systems in TaiwanDocument7 pagesGenetic Evaluation of Children With Global Developmental Delaydcurrent Status of Network Systems in Taiwanfkia2013No ratings yet
- Intervención Familiar Profesional, Como Internvención en TEADocument16 pagesIntervención Familiar Profesional, Como Internvención en TEAfrancisca rojas rodriguezNo ratings yet
- Identification and Management of ASD Pediatrics.2019-3447.fullDocument66 pagesIdentification and Management of ASD Pediatrics.2019-3447.fullMaríaNo ratings yet
- AutismScreen AssessDocument42 pagesAutismScreen AssessMelindaDuciagNo ratings yet
- Early Behavioral Markers For Neurodevelopmental Disorders in The First 3 Years of Life An Overview of Systematic ReviewsDocument19 pagesEarly Behavioral Markers For Neurodevelopmental Disorders in The First 3 Years of Life An Overview of Systematic ReviewsMatheus PrenassiNo ratings yet
- Research Final Na ToooooDocument19 pagesResearch Final Na ToooooNaja ReyesNo ratings yet
- Autism Screen and AssessmentDocument51 pagesAutism Screen and Assessmentcynthia100% (3)
- Early InterventionDocument13 pagesEarly Interventionapi-290229666No ratings yet
- Recommended Autism ScreeningDocument21 pagesRecommended Autism ScreeningLiliana Torres EscalonaNo ratings yet
- Systematic Review of Tools To Measure Outcomes For Young Children With Autism Spectrum Disorder - PubMedDocument2 pagesSystematic Review of Tools To Measure Outcomes For Young Children With Autism Spectrum Disorder - PubMedDaniel NovakNo ratings yet
- Assessment of Attention in PreschoolersDocument23 pagesAssessment of Attention in PreschoolersMarilda GhellereNo ratings yet
- Attention Deficit Disorders and Gifted Students What Do We Really KnowDocument4 pagesAttention Deficit Disorders and Gifted Students What Do We Really KnowCyndi WhitmoreNo ratings yet
- Peds 20193447Document69 pagesPeds 20193447Mahi KouNo ratings yet
- Responding and Identifying To Developmental Delay in ChildrenDocument13 pagesResponding and Identifying To Developmental Delay in ChildrenInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Assessment of Co-Occurring Disabilities in Young Children Who AreDocument24 pagesAssessment of Co-Occurring Disabilities in Young Children Who AreMariana BucurNo ratings yet
- Research in Autism Spectrum Disorders: SciencedirectDocument5 pagesResearch in Autism Spectrum Disorders: SciencedirectdalimahNo ratings yet
- Ages Questionary Development ScreeningDocument7 pagesAges Questionary Development ScreeningPamela Chuquicondor CuevaNo ratings yet
- Identification, Evaluation, and Management of Children With ASDDocument69 pagesIdentification, Evaluation, and Management of Children With ASDWing Sze FUNGNo ratings yet
- European Journal of Pediatrics SciDocument7 pagesEuropean Journal of Pediatrics ScianimeshNo ratings yet
- M SC Audiology English VersionDocument2 pagesM SC Audiology English VersionMayankNo ratings yet
- Name - : Prakhar VermaDocument5 pagesName - : Prakhar VermaMayankNo ratings yet
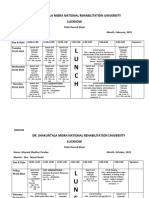
- L U N C H: Dr. Shakuntala Misra National Rehabilitation University LucknowDocument13 pagesL U N C H: Dr. Shakuntala Misra National Rehabilitation University LucknowMayankNo ratings yet
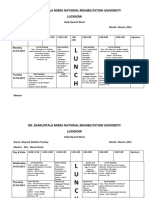
- L U N C H: Dr. Shakuntala Misra National Rehabilitation University LucknowDocument4 pagesL U N C H: Dr. Shakuntala Misra National Rehabilitation University LucknowMayankNo ratings yet
- MayankOCT 21-9 Jan Drs - DocxssDocument28 pagesMayankOCT 21-9 Jan Drs - DocxssMayankNo ratings yet
- L U N C H: Dr. Shakuntala Misra National Rehabilitation University LucknowDocument4 pagesL U N C H: Dr. Shakuntala Misra National Rehabilitation University LucknowMayankNo ratings yet
- Lecture 38Document10 pagesLecture 38Deepak GuptaNo ratings yet
- ST. LUKE'S MEDICAL CENTER EMPLOYEE'S FOUNDATION AFW v. NLRCDocument3 pagesST. LUKE'S MEDICAL CENTER EMPLOYEE'S FOUNDATION AFW v. NLRCjodelle11No ratings yet
- Exam1 Key JMB s06Document13 pagesExam1 Key JMB s06Steve DangNo ratings yet
- API 16C ErrataDocument1 pageAPI 16C ErrataDinesh KumarNo ratings yet
- Dance Lesson Plan Grade 12Document4 pagesDance Lesson Plan Grade 12api-24976678488% (34)
- PNOZ E1vp EN-23-27Document5 pagesPNOZ E1vp EN-23-27Rachid MoussaouiNo ratings yet
- 5 Natural Sore Throat RemediesDocument5 pages5 Natural Sore Throat Remedieslisa smithis100% (1)
- Heat Transfer Lab AssignmentDocument5 pagesHeat Transfer Lab AssignmentChristyNo ratings yet
- Eastman Methyl N-Amyl Ketone (MAK) and Eastman Methyl Isoamyl Ketone (MIAK)Document4 pagesEastman Methyl N-Amyl Ketone (MAK) and Eastman Methyl Isoamyl Ketone (MIAK)Chemtools Chemtools100% (1)
- Alcohol Consumption and Related Crime Incident in John Paul CollegeDocument17 pagesAlcohol Consumption and Related Crime Incident in John Paul Collegejoy mesanaNo ratings yet
- Punjab National BankDocument4 pagesPunjab National BankShubham RajNo ratings yet
- Glycerin As A Renewable Feedstock For EpichlorohydDocument6 pagesGlycerin As A Renewable Feedstock For EpichlorohydMuhammad RidhauddinNo ratings yet
- 432.01 Managing HSE in A Geophysical Nov 2017Document138 pages432.01 Managing HSE in A Geophysical Nov 2017Andrei Savu100% (1)
- Bycatch Reduction Devices - PresentationDocument92 pagesBycatch Reduction Devices - PresentationSujit Shandilya0% (1)
- 2013 Medigate Profile PDFDocument26 pages2013 Medigate Profile PDFGabriel Duran DiazNo ratings yet
- Leoline Installation and MaintenanceDocument8 pagesLeoline Installation and MaintenanceFloorkitNo ratings yet
- Scala: Service InstructionsDocument16 pagesScala: Service Instructionsmario_turbinadoNo ratings yet
- AT-502 - AT-504 - OM-0-Introduction-1 - 10-12-2019Document6 pagesAT-502 - AT-504 - OM-0-Introduction-1 - 10-12-2019Vinicius RodriguesNo ratings yet
- Reishi MushroomDocument5 pagesReishi Mushroomjunver100% (4)
- Afcat Question Paper 01-2014 PDFDocument10 pagesAfcat Question Paper 01-2014 PDFTuhin AzadNo ratings yet
- Grade Control For Australian Open Pit Gold MinesDocument14 pagesGrade Control For Australian Open Pit Gold Mineswaldo100% (1)
- Herbs and SpicesDocument77 pagesHerbs and SpicesNicole RicohermosoNo ratings yet
- Dialysis and ElectrodialysisDocument32 pagesDialysis and ElectrodialysisJuan CarvajalNo ratings yet
- La Paz National High SchoolDocument19 pagesLa Paz National High SchoolBon Ivan FirmezaNo ratings yet
- Manual Servicio Soxte 2050Document46 pagesManual Servicio Soxte 2050Quimica JordanlabNo ratings yet
- Leonard Peikoff-Introduction To LogicDocument20 pagesLeonard Peikoff-Introduction To Logicbursa07No ratings yet
- ACRE2a Non Elementary Reaction Kinetics RevDocument53 pagesACRE2a Non Elementary Reaction Kinetics RevRathish RagooNo ratings yet
- ISO 9001 Required DocumentationDocument3 pagesISO 9001 Required Documentationdnmule100% (1)
- TD-XT-D004-003 V2.00 20131204 XG1.UCD-135M185M300M Operation Manual PDFDocument47 pagesTD-XT-D004-003 V2.00 20131204 XG1.UCD-135M185M300M Operation Manual PDFStan TC100% (1)
- Megapower: Electrosurgical GeneratorDocument45 pagesMegapower: Electrosurgical GeneratorAnibal Alfaro VillatoroNo ratings yet