Professional Documents
Culture Documents
Gastrointestinal Drugs: Alexander J. German, Jill E. Maddison and Grant Guilford
Gastrointestinal Drugs: Alexander J. German, Jill E. Maddison and Grant Guilford
Uploaded by
TORRES GUTIERREZ JOYNY RAQUEL catedraticoOriginal Title
Copyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
Gastrointestinal Drugs: Alexander J. German, Jill E. Maddison and Grant Guilford
Gastrointestinal Drugs: Alexander J. German, Jill E. Maddison and Grant Guilford
Uploaded by
TORRES GUTIERREZ JOYNY RAQUEL catedraticoCopyright:
Available Formats
19
Gastrointestinal drugs
Alexander J. German, Jill E. Maddison and Grant Guilford
Relevant pathophysiology
ANTIEMETIC DRUGS
Antiemetic drugs may have central or peripheral actions
Vomiting may occur as a sequel to primary or secondary (Fig. 19.1).
(nonenteric) gastrointestinal disease. Antiemetic therapy
should only be considered as symptomatic therapy. Initiation of vomiting
The clinician’s attention should primarily be directed Vomiting is initiated by either humoral or neural path-
at determining and resolving the underlying disease ways. The humoral pathway involves stimulation of the
process. A great variety of drugs have been found to be chemoreceptor trigger zone (CTZ) by blood-borne sub-
useful in treating vomiting due to different causes. stances, while the neural pathway is through activation
However, no single drug is effective for all types of of the vomiting center.
emesis.
Given that they are a symptomatic therapy, antiemet- Vomiting center
ics are often used in combination with other drugs and All animal species that vomit have a brainstem ‘vomit-
clinicians should be aware of potential drug interactions ing center’ – a group of several nuclei that act in concert
that may arise. For example, metoclopramide may affect to co-ordinate the somatomotor events involved in
the absorption of other drugs and have an impact on expelling gastric contents. Nonvomiting species (such as
efficacy (see below). Therefore, these drugs must be used rodents and rabbits) also have the brainstem nuclei and
with due care. motor systems necessary for emesis but lack the complex
synaptic interaction among nuclei and viscera required
for a co-ordinated reflex.
Clinical applications The concept of a discrete vomiting center within the
reticular formation of the medulla oblongata has been
Antiemetics are indicated to:
challenged. However, whether it is a discrete anatomical
● control vomiting, especially when profuse and pro-
center or represents sequential activation of a series of
tracted vomiting may lead to fluid, electrolyte or
effector nuclei, the important concept is that the medulla
acid–base disturbances or is causing distress to the
has a central co-ordinating role in emesis.
patient or owner
The vomiting center receives input from vagal and
● prevent vomiting predicted to occur with use of
sympathetic neurones, the CTZ in the area postrema,
emetic drugs, e.g. cisplatin, amphotericin.
the vestibular apparatus and the cerebral cortex. It may
Use of antiemetics is not necessary if vomiting is also be stimulated directly by blood-borne toxins that
intermittent, the patient is not distressed and correction can cross the blood–brain barrier.
of fluid and electrolyte imbalances can easily be The receptors that have been identified as important
achieved. in the vomiting center are 5-hydroxytryptamine (5-
HT)1A, α2-adrenergic receptors and neurokinin-1 (NK1)
receptors which are receptors for substance P. Drugs
Inappropriate use of antiemetics such as buspirone act as antiemetics by acting as antago-
Use of antiemetics in the following situations is nists at 5-HT1A receptors. Antiemetics such as prochlor-
inappropriate: perazine block α-adrenergic receptors. Maropitant
● gastrointestinal obstruction – antiemetics may delay (Cerenia®) acts at NK1 receptors.
diagnosis
● gastrointestinal toxicity – antiemetics may prevent Central stimulation
the patient from eliminating the toxin Central stimulation of the vomiting center occurs via
● systemic hypotension – the phenothiazines and higher centers in the central nervous system. Stimuli
α2-adrenergic antagonists, when used in high doses, include nervousness, unpleasant odors, pain and psy-
can intensify hypotension. chogenic factors. Opioids and benzodiazepine receptors
469
Ch019-S2858.indd 469 11/19/2007 2:28:56 PM
CHAPTER 19 GASTROINTESTINAL DRUGS
histaminergic and NK1 receptors must be involved in
Cerebral cortex Nucleus tractus solitarius the dog because antagonists at these receptors are very
Opioid H1, NK1, M1
effective antiemetic agents. D2-dopaminergic, α2-
adrenergic and 5-HT3 receptors are not involved.
Phenothiazines
Chemoreceptor trigger zone (CTZ)
The CTZ is located in the area postrema in the floor of
Vestibular the fourth ventricle. It has no blood–brain barrier, thus
Antihistamines H1, M1 allowing access to toxins and chemicals normally
excluded from the CNS by the blood–brain barrier. The
CTZ is stimulated by endogenous toxic substances pro-
Vomiting centre duced in acute infectious diseases or metabolic disorders
α2, 5HT1A, NK1 such as uremia and diabetic ketoacidosis and by drugs
and other exogenous toxins.
A variety of neurotransmitters and their receptors are
CRTZ important in the CTZ, including dopamine, adrenaline
D2, M1, H1 and H2 Anticholinergics
5HT3, NK1 Opioid
NK1 antagonists (epinephrine), 5-HT, acetylcholine, histamine, encepha-
lins and substance P. Species differ in the relative impor-
tance of some neurotransmitter–receptor systems. For
Peripheral receptors
5HT3 antagonists example, apomorphine, a D2-dopamine receptor agonist,
M2, 5HT3, 5HT4, Motilin,
NK1, D2 is a potent emetic in dogs and humans but not in the
Metoclopramide, cat, monkey, pig, horse or domestic fowl. This suggests
dromperidone that D2-dopamine receptor antagonists such as metoclo-
pramide might not be very useful as antiemetics in
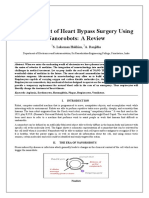
Fig. 19.1 Diagrammatic representation of receptors
the cat.
involved in emesis and sites of action of antiemetics.
In contrast, xylazine, an α2-adrenergic agonist, is a
more potent emetic in the cat than the dog. Cytotoxic
have been implicated in centrally initiated vomiting but drug-induced emesis has been shown to be mediated
have not been well characterized pharmacologically. directly by 5-HT3 receptors in the CTZ of the cat, in
The role of opioid receptors in emesis is confusing. contrast to the dog, in which peripheral visceral and
Various studies have demonstrated that opioids have an vagal afferent 5-HT3 receptors are activated.
emetic action in dogs and cats. However, opioids have Histamine receptors have not been demonstrated in
been used in humans and animals to reduce nausea and the CTZ of the cat. Studies based on eliminating the
vomiting associated with cancer chemotherapy. This emetic response to parenterally administered compounds
apparent paradox is caused by a differential effect of by lesioning the CTZ suggest that the CTZ may be less
opioids on the CTZ and the vomiting center. If an sensitive to emetic compounds in the cat than in the dog.
opioid penetrates the vomiting center it may strongly Alternatively, other sites for the origin of emesis may be
block the vomiting reflex. However, if an opioid pene- more important in the cat than the dog.
trates the CTZ first it will initially cause vomiting before
blocking the vomiting center. Morphine has been dem- Peripheral receptors
onstrated to have this dual effect (although it may also Peripheral receptors are located mainly in the gastroin-
cause vomiting because of histamine release). testinal tract, particularly the duodenum but also in the
Centrally induced vomiting may also occur as a result biliary tract, peritoneum and urinary organs. The recep-
of direct stimulation of the vomiting center by increased tors may be stimulated by distension, irritation, inflam-
cerebrospinal fluid pressure, encephalitis or CNS mation or changes in osmolarity.
neoplasia.
Afferent receptors
Vestibular apparatus Of the many afferent receptors found in the gut, 5-HT3
Labyrinthine impulses associated with motion sickness receptors play an important role in initiation of vomit-
and middle-ear infection also stimulate the vomiting ing by cytotoxic drugs. Cytotoxic drugs cause 5-HT
center via neural pathways arising from the vestibular release from enterochromaffin cells that activates 5-HT3
system. The CTZ is involved in this pathway in the dog receptors on vagal afferent fibers. 5-HT3 receptor antag-
but not in the cat. onists are very effective antiemetics for cytotoxic drug-
The neuronal pathways for motion sickness have not induced vomiting. However, the role of 5-HT3 receptors
been completely characterized. M1-cholinergic, H1- in other disorders of the gut has yet to be ascertained.
470
Ch019-S2858.indd 470 11/19/2007 2:28:56 PM
CLASSES OF ANTIEMETICS
Efferent receptors Pharmacokinetics
Vagal efferent receptors and myenteric neurones initiate Little information is available regarding the pharmaco-
the complex excitation and inhibition of visceral smooth kinetics of prochlorperazine in animals, although it is
muscle that culminates in emesis. Receptors involved believed to follow the general pattern of metabolism
include D2-dopaminergic, 5-HT4 serotonergic, M2- and elimination of other phenothiazine agents, i.e.
cholinergic, NK1 and motilin receptors. metabolism in the liver with both conjugated and
unconjugated metabolites eliminated in the urine.
Although chlorpromazine is absorbed well from the
CLASSES OF ANTIEMETICS gastrointestinal tract, it has a high first-pass metabo-
lism. In the circulation, chlorpromazine is highly bound
Phenothiazines
to plasma proteins – in humans the half-life is 36 h.
EXAMPLES Adverse effects
Prochlorperazine (e.g. Stemetil®, Compazine®, ● Phenothiazines may cause hypotension because of
Darbazine®), chlorpromazine (e.g. Thorazine®) central effects and an α-adrenergic receptor-blocking
action resulting in arteriolar vasodilation. Therefore,
they should not be included at high doses in a thera-
Clinical applications peutic regime until dehydration is corrected by intra-
Phenothiazines are broad-spectrum antiemetics that venous fluid therapy. They should not be given as an
have efficacy against vomiting initiated by central and undiluted intravenous bolus.
peripheral stimuli. ● Sedation may occur at high doses.
● Similarly to other phenothiazines, it is believed that
Mechanism of action prochlorperazine may lower the seizure threshold.
Phenothiazines antagonize α1- and α2-adrenergic There is anecdotal evidence in the literature that this
receptors, D2-dopaminergic receptors, H1- and H2- occasionally occurs.
histaminergic receptors and muscarinic cholinergic ● Extrapyramidal reactions such as rigidity, tremors,
receptors (weakly). They therefore have antiemetic weakness and restlessness may occur at high doses.
activity (see Fig. 19.1) at the CTZ (D2-receptors, H1-
and H2-receptors and muscarinic cholinergic receptors) Known drug interactions
and at high doses at the vomiting center (α2- ● It has been stated that phenothiazines should not be
receptors). given within 1 month of worming with an organo-
Prochlorperazine is a piperazine phenothiazine with phosphate agent as the effect of either drug may
less sedative action than other phenothiazines such be potentiated. Whether this is a realistic clinical
as acepromazine and chlorpromazine. In contrast to problem is debatable.
acepromazine, chlorpromazine has antiemetic efficacy ● Other CNS-active drugs such as barbiturates, narcot-
at doses low enough to avoid sedation. ics and anesthetic agents may cause additive CNS
depression.
Formulations and dose rates ● Quinidine given with phenothiazines may cause
additive cardiac depression.
In most countries, prochlorperazine is only available in human- ● Antidiarrheal mixtures containing kaolin and pectin
approved formulations (e.g. Stemetil®, Compazine®) such as pro- and antacids may cause reduced absorption of orally
chlorperazine edisylate (injectable or oral syrup), prochlorperazine administered phenothiazines.
maleate (tablets) or prochlorperazine base (rectal suppositories). ● Increased blood concentrations of both drugs
There are few, if any, countries where chlorpromazine is available as
may occur if propranolol is administered with
a veterinary-approved product.
phenothiazines.
DOGS AND CATS ● As phenothiazines block α-adrenergic receptors, if
adrenaline (epinephrine) is administered concur-
Prochlorperazine
• 0.1–0.5 mg/kg IV, IM, SC q.6-8 h
rently, unopposed β-adrenergic effects will occur,
• 0.5–1.0 mg/kg PO q.8-12 h causing vasodilation and tachycardia.
NB: Intramuscular injection may be painful but not to a degree that ● Phenytoin metabolism may be decreased if given con-
precludes administration by this route in most patients if necessary. currently with phenothiazines.
Chlorpromazine ● The following drugs that might conceivably be used
• 0.1–0.5 mg/kg IM, SC q.8 h concurrently with prochlorperazine or chlorproma-
zine (other drugs may also be incompatible) are
471
Ch019-S2858.indd 471 11/19/2007 2:28:56 PM
CHAPTER 19 GASTROINTESTINAL DRUGS
reported to be incompatible in solution: amphoteri- nism of peripheral D2-receptors, although enhanced
cin B, ampicillin sodium, chloramphenicol sodium cholinergic activity may also be involved. However,
succinate, dimenhydrinate, hydrocortisone sodium there is evidence from some animal studies that the
succinate, penicillin G sodium, phenobarbital gastrointestinal effects of metoclopramide may be disas-
sodium. Chlorothiazide sodium and methicillin are sociated from its dopamine receptor-blocking action.
also incompatible with chlorpromazine. In addition, Intact vagal innervation is not necessary for enhanced
do not mix with other drugs or diluents containing motility but anticholinergic drugs will negate its effects.
parabens as preservatives. Metoclopramide has also been demonstrated to have
anticholinesterase effects and there are suggestions that
Metoclopramide this drug sensitizes gastrointestinal smooth muscle to
the effects of acetylcholine.
Clinical applications
Gastrointestinal effects include increased tone and
Metoclopramide is indicated for control of vomiting
amplitude of gastric contractions, relaxation of the
associated with:
pyloric sphincter and increased duodenal and jejunal
● various emesis-inducing disorders involving either
peristalsis. Gastric emptying and intestinal transit times
stimulation of the CTZ or depressed
can be significantly reduced. There is little or no effect
gastrointestinal motility
on colonic motility.
● cancer chemotherapy
A beneficial effect of metoclopramide could not be
● gastroesophageal reflux
demonstrated in dogs with gastric dilation and volvulus
● decreased gastric emptying associated with:
and delayed gastric emptying treated with metoclo-
– inflammatory gastrointestinal disorders
pramide postsurgically. However, as the study involved
– gastric ulcers
use of liquids rather than solids, it might have been dif-
– gastric neoplasia
ficult to demonstrate an effect even if gastric motility
– autonomic neuropathy (diabetes mellitus)
was enhanced.
– postoperative gastric dilation and volvulus
Metoclopramide will also increase lower esophageal
surgery/intervention
pressure and reduce gastroesophageal reflux. This effect
– abnormal gastric motility.
is abolished by diphenhydramine. The increased lower
Although metoclopramide is sometimes recommended esophageal pressure induced by metoclopramide is not
for endoscopic procedures to facilitate passage of the sufficient to prevent gastric reflux in anesthetized dogs,
endoscope through the pylorus, this effect was not con- although it does lower the risk.
firmed in a well-controlled study of the effect of phar- Studies have indicated that metoclopramide has a
macological agents on the ease of endoscopic intubation biphasic effect on ureteral motility, increasing motility
in dogs. In fact, increased antral motility caused by at low doses and inhibiting it at high doses. Semen
metoclopramide makes endoscopic intubation more volume is reported to be reduced in dogs treated with
difficult. metoclopramide but sperm number was not significantly
affected.
Mechanism of action
Centrally, metoclopramide antagonizes D2-dopaminergic
receptors and 5-HT3 serotonergic receptors and has a
peripheral cholinergic effect. The antiemetic properties of Formulations and dose rates
metoclopramide may be related to 5-HT3 receptor antag-
Metoclopramide is available as a veterinary preparation in tablet and
onism rather than D2-receptor antagonism, even though injectable formulations in some countries (e.g. Australia) but only as
it has been classified for many years as an antidopaminer- a human preparation in others (e.g. USA, UK). Metoclopramide is
gic drug. The evidence supporting reassessment of its photosensitive and should be stored in light-resistant containers at
mode of action includes the observation that analogs of room temperature.
metoclopramide have been developed that are effective
antiemetics but show little or no dopamine antagonism. DOGS AND CATS
They are very specific 5-HT3 antagonists and it is there- • 0.2–0.5 mg/kg IM, SC, PO q.6–8 h
fore believed that the serotonin-antagonist effects of • 1–2 mg/kg IV infusion over 24 h
The efficacy of metoclopramide is believed to be enhanced by admin-
metoclopramide account for a large part of its antiemetic
istering 1–2 mg/kg/d by a constant-rate infusion instead of intermit-
effects. However, antidopaminergic mechanisms are
tent boluses.
still believed to play a role in the antiemetic action of When used to treat disorders of gastric motility and esophageal
metoclopramide. reflux, metoclopramide should be administered at a dose of 0.2–
Metoclopramide is commonly believed to cause 0.5 mg/kg PO 30 min before meals.
increased gastric emptying, primarily through antago-
472
Ch019-S2858.indd 472 11/19/2007 2:28:56 PM
CLASSES OF ANTIEMETICS
Pharmacokinetics intestine, e.g. cimetidine, aspirin, tetracyclines,
Metoclopramide is well absorbed from the gastrointes- diazepam.
tinal tract in humans and dogs. In humans, bio- ● Given that metoclopramide can accelerate the absorp-
availability can be reduced by up to 30% in some tion of nutrients, insulin requirements may be influ-
patients as a result of first-pass metabolism; this effect enced in diabetic animals.
is quite variable among individuals. One study sug- ● Metoclopramide antagonizes the antiprolactinemic
gested that similarly, in dogs, the liver plays an active effects of cabergoline.
role in reducing the systemic availability of metoclo-
pramide after oral administration. In a study of two Domperidone
greyhounds, bioavailability of metoclopramide after Clinical applications
oral administration was about 48%. Bioavailability Domperidone is a dopamine antagonist at D2-receptors
after intramuscular injection in humans is 74–96%. which has similar actions to metoclopramide. It does
The plasma half-life of metoclopramide in the dog is not appear to cross as readily into the CNS as metoclo-
approximately 90 min. In contrast to humans, in whom pramide and therefore is believed not to have the same
glucuronidation and sulfate conjugation are the major CNS effects as that drug. However, extrapyramidal
metabolic pathways, N-demethylation is more impor- adverse effects have been observed in some human
tant for metoclopramide metabolism in dogs. patients.
Adverse effects Mechanism of action
Side effects are uncommon but occur more often in cats Domperidone is a dopamine antagonist in the CTZ and
than in dogs. GI tract. It also is an α2- and β2-adrenergic antagonist
● Metoclopramide may cause (infrequently) mental in the stomach.
changes ranging from hyperactivity to depression.
● Cats will infrequently show disorientated or
frenzied behavior. Formulations and dose rates
● Metoclopramide should not be used when
gastrointestinal hemorrhage, obstruction or Domperidone is not available as a veterinary preparation in any
perforation is suspected. market but is available as a human preparation (Motilium®) and used
● This drug is relatively contraindicated in patients
quite extensively in some European countries. It is available as 10 mg
tablets and a 1 mg/mL suspension and in some markets as supposi-
with seizure disorders.
tories and an oral suspension.
● Use with caution in patients with renal
insufficiency because some reports suggest that DOGS AND CATS
metoclopramide reduces renal blood flow and may • 2–5 mg per animal q.8 h
exacerbate pre-existing disease.
Known drug interactions
● Excellent synergy (as a result of their different modes Pharmacokinetics
of action) can be obtained in the management of Domperidone is absorbed from the GI tract but has an
persistent vomition using metoclopramide and phe- oral bioavailability of only 20% in the dog. This is
nothiazines concurrently. However, because of the presumably due to a high first-pass effect. The drug is
potential for enhanced CNS effects, metoclopramide highly protein bound (93%). Peak levels occur about
should be used with care with phenothiazines, 2 h after dosing. Metabolites are excreted in urine and
butyrophenones and opioid analgesics. feces.
● Anticholinergic drugs (e.g. atropine) and narcotic
analgesics may negate the effects of metoclopramide Adverse effects
on gastrointestinal tract motility. ● There is little information on the use of domperidone
● The gastrointestinal stimulatory effects of metoclo- in veterinary medicine.
pramide may affect absorption of many drugs. Drug ● It may cause gastroparesis.
products that disintegrate, dissolve or are absorbed ● Because domperidone is a potential substrate of P-
in the stomach, such as digoxin, may be absorbed glycoprotein, it should be used with caution in
less, although the increased vigor of antral contrac- herding breeds such as collies which may have the
tions can also hasten disintegration. gene mutation that causes a nonfunctional protein.
● Metoclopramide may enhance the absorption of ● The drug is teratogenic at high doses in mice, rats
drugs that are absorbed primarily in the small and rabbits.
473
Ch019-S2858.indd 473 11/19/2007 2:28:56 PM
CHAPTER 19 GASTROINTESTINAL DRUGS
● Because dopamine is involved in prolactin produc- ent input to the vomiting center (vestibular system),
tion, domperidone may increase prolactin levels compared with the neural and humoral inputs associ-
resulting in galactorrhea or gynecomastia. ated with general emesis.
● There may be an impact on fertility as a result of
domperidone’s effect on prolactin levels. Mechanism of action
● Injectable formulations have been associated with Maropitant is a selective antagonist of substance P at
cardiac arrhythmias in human patients with cardiac the NK1 receptor. Some studies would suggest the antag-
disease or hypokalemia. onism is competitive. However, other studies suggest
● Rarely, somnolence or dystonic reactions have the inhibition is nonsurmountable. It inhibits the final
occurred in people. common pathway involved in activating the vomiting
reflex in the CNS and is effective against emesis induced
Known drug interactions by both peripheral and central stimuli.
Domperidone should not be used with dopaminergic
drugs such as dopamine or dobutamine.
Formulations and dose rates
NK1 receptor antagonists
DOGS
EXAMPLE Prevention or treatment of emesis due to central or
peripheral stimuli
Maropitant (Cerenia®) • 2 mg/kg PO, once daily for up to 5 d
• 1 mg/kg SC, once daily for up to 5 d
Prevention of motion sickness
• 8 mg/kg PO, once daily for a maximum of two consecutive days
Clinical applications
Maropitant is the first drug of its class registered (in
some markets) for veterinary use. It is indicated for the Pharmacokinetics
prevention and treatment of general emesis in the dog Oral bioavailability is 23.7% at a 2 mg/kg dose rate and
and the prevention of motion sickness in the dog. 37% at 8 mg/kg. The difference suggests that first-pass
In laboratory studies, the drug was highly effective in metabolism is proportionally greater at the 8 mg/kg
preventing and treating vomiting induced by apomor- dose, possibly due to saturation of a high-affinity, low-
phine (centrally acting purely at the CTZ), cisplatin capacity enzyme system (or efflux pump system) limiting
(central and peripheral emetic stimulus) and ipecac access of the drug to the systemic circulation at the
(peripheral emetic stimulus) at a dose of 1 mg/kg SC or 2 mg/kg dose. Feeding does not affect oral bio-
2 mg/kg PO. availability at the 2 mg/kg dose rate. Bioavailability
Efficacy has also been demonstrated in field studies. when given subcutaneously is 90.7%.
Maropitant was significantly more effective in reducing Maropitant is metabolized by first-order kinetics in
emetic events in dogs treated for acute vomiting than the liver by two enzyme systems: CYP2D15 (high affin-
metoclopramide; the proportion of dogs not vomiting ity, responsible for >90% of clearance) and CYP3A12
within 24 h was 92% for maropitant and 50% for (low affinity, high capacity). Hepatic clearance is the
metoclopramide, a difference that was statistically sig- major route of excretion; there is no evidence of excre-
nificant. In relation to prevention of cisplatin-induced tion of active drug or its major metabolite.
emesis, only two of 39 dogs treated with maropitant 1 h
prior to cisplatin treatment vomited compared with 39 Adverse effects
of 41 dogs who vomited when treated with saline alone Post-dosing emesis occurs in approximately 8% of dogs
prior to cisplatin treatment. Maropitant was also suc- treated at the 8 mg/kg dose rate for the prevention of
cessful in treating cisplatin-induced vomiting, i.e. when motion sickness. This is believed to be due to a local
the drug was given after cisplatin-induced vomiting effect of the drug on the GI tract and can be reduced by
commenced. dosing after consumption of a small amount of food.
Maropitant also has efficacy in preventing motion
sickness but a higher dose is required. In a small field Known drug interactions
study, motion sickness was prevented in the majority of ● In laboratory and field studies significant drug inter-
(but not all) dogs with recurrent and persistent motion actions are unlikely to occur due to its margin of
sickness only at a dose of 8 mg/kg PO. The higher dose safety and well-characterized pharmacokinetics.
of maropitant required to prevent emesis associated ● Significant hepatic dysfunction could interfere with
with motion sickness is likely to be related to the differ- metabolism and elimination of maropitant but the
474
Ch019-S2858.indd 474 11/19/2007 2:28:57 PM
CLASSES OF ANTIEMETICS
wide margin of safety for the drug suggests that this For intractable vomiting, when first-line drugs are ineffective
may not have clinically relevant adverse effects. • 0.1–0.176 mg/kg q.6–12 h as a slow intravenous push
• 0.5–1.0 mg/kg PO once or twice daily
5-HT3 antagonists
CATS
EXAMPLES The use of ondansetron in cats is controversial and many pharmacolo-
gists do not recommend its use in this species.
Ondansetron (Zofran®), granisetron (Kytril®), dolasetron
(Carpuject®, Anzemet®, Anemet®, Zamanon®) and OTHER 5-HT3 ANTAGONISTS
tropisetron Dolasetron is also available as both injectable (0.625 mL ampoules)
and tablet (50 mg and 100 mg strength) formulations. The size of
tablets is inconvenient for most cats and dogs, such that oral ondan-
setron preparations are preferred.
• 0.5–0.6 mg/kg IV, SC or PO q.24 h
Clinical applications
The 5-HT3 receptor antagonists are extremely potent
(and expensive) antiemetics used in the management of Adverse effects
cancer therapy-induced emesis in humans. Their clinical ● Experimental studies suggest that 5-HT3 antagonists
efficacy is orders of magnitude better than metoclo- are very safe in animals, showing minimal toxicity at
pramide (e.g. 100 times better in the ferret) and they are doses up to 30 times greater than those needed to
often used in cases when ‘first-line’ antiemetics (e.g. abolish vomiting.
metoclopramide or chlorpromazine) are ineffective. In ● Given that ondansetron, and related products, are
this regard, these drugs can often control vomiting in potent antiemetics, their use may mask signs of ileus
puppies with parvoviral gastroenteritis. They have been or gastrointestinal distension. These drugs should be
used occasionally in dogs to control cisplatin-induced used with caution in cases where gastrointestinal
emesis but cost is prohibitive for most veterinary clinical obstruction cannot be excluded because appropriate
situations. therapy may be delayed.
● In humans, constipation, headaches, occasional
Mechanism of action alterations in liver enzymes and rarely hypersensitiv-
5-HT3 receptors are located in the CTZ and, peripher- ity reactions have been reported.
ally, on vagal nerve terminals and on enteric neurones ● Dolasetron has also been associated with ECG inter-
in the gastrointestinal tract. Although initially 5-HT3 val prolongation (of the P-R, Q-T and J-T segments),
antagonists were thought to have a central action on the whilst arrhythmias and hypotension have also been
CTZ, recent work suggests that their main effect is reported for ondansetron.
through antagonism of peripheral 5-HT3 receptors in ● Safety of this drug group during gestation has not
the gut. This is supported by work demonstrating that been clearly established, so the drug should be used
chemotherapy-induced vomiting is caused by serotonin with caution in pregnant animals.
release from small intestinal enterochromaffin cells. ● Ondansetron is a potential substrate of P-glycopro-
tein. Given that some rough collies have a mutation
causing a nonfunctional protein, these dogs and
Formulations and dose rates associated breeds may be more sensitive to the effects
of 5-HT3 antagonists.
Most veterinary experience has been with ondansetron; most of the
other drugs have not had extensive use at the current time. No
veterinary formulations of any of these drugs are available. Anticholinergics
ONDANSETRON EXAMPLES
Ondansetron is available both as injectable and as tablet
formulations. Atropine, butylscopolamine (hyoscine), propantheline,
isopropamide
DOGS
Prevention of cisplatin-induced vomiting
• 0.5 mg/kg IV as a loading dose and then 0.5 mg/kg/h as an
infusion for 6 h Clinical applications
• 0.1 mg/kg PO q.12–24 h or at 30 min prior to and 90 min after Anticholinergics are mainly used for their antispasmodic
cisplatin infusion and antisecretory actions for some types of diarrhea.
Given that their use is contradicted in many
475
Ch019-S2858.indd 475 11/19/2007 2:28:57 PM
CHAPTER 19 GASTROINTESTINAL DRUGS
circumstances, they should be used with caution. These drugs should also be avoided in cases suspected to
drugs have also been used frequently in the past as have gastrointestinal obstruction.
antiemetics but usually inappropriately. They are usually ● Overuse can result in gastric atony and intestinal
not effective unless vomiting is initiated by smooth ileus, which may predispose to absorption of endo-
muscle spasm (an extremely uncommon occurrence). toxins through damaged mucosa.
They do not stop vomiting caused by stimulation of ● Antimuscarinic agents should be used with caution
peripheral receptors by other means such as inflamma- in cases with known or suspected enteric infections,
tion. Those anticholinergic drugs that can cross the because the reduction in motility may prolong the
blood–brain barrier (e.g. hyoscine) are effective for retention of the causative agent.
motion sickness through antagonism of M1-receptors in ● Antimuscarinic agents should also be used with
the vestibular apparatus. caution in animals with hepatic or renal disease,
Anticholinergics have been used in the management hyperthyroidism, congestive heart failure, hyperten-
of pancreatitis on the basis that they may reduce pan- sion, concurrent myasthenia gravis, prostatic hyper-
creatic secretion. However, no appreciable benefit has trophy and in geriatric or pediatric patients.
been demonstrated experimentally or clinically from ● Side effects are those expected for antimuscarinics,
this treatment. In fact, some clinicians consider that e.g. xerostomia, dry eyes, hesitant urination, tachy-
their use is contraindicated in pancreatitis because they cardia and constipation. CNS side effects include
cause thickening of pancreatic secretions. stimulation, drowsiness, ataxia, seizures and respira-
tory depression; however, these effects are unlikely
Mechanism of action with the quaternary ammonium antimuscarinics.
Anticholinergics act as antagonists at central and periph- Ocular side effects of this group include mydriasis,
eral muscarinic receptors (M1 and M2). Quaternary cycloplegia and photophobia; again, these side
ammonium antimuscarinics, such as butylscopolamine effects are less likely with quaternary ammonium
and propantheline, do not cross the blood–brain barrier, antimuscarinics.
so have a predominantly peripheral action, and CNS
side effects are minimal. Known drug interactions
● Antimuscarinics can enhance the actions of thiazide
diuretics and sympathomimetics and antagonize the
Formulations and dose rates effects of metoclopramide.
● Antihistamines, procainamide, quinidine, meperi-
Atropine sulfate is available as an injectable preparation. No veteri- dine, benzodiazepines and phenothiazines can all
nary-approved preparations of propantheline are available, but generic potentiate the effects of anticholinergics.
human tablet formulations can be used (7.5 mg, 15 mg). In some ● Adverse effects can be exacerbated by corticoste-
countries, butylscopalamine is available, as both injectable and oral
roids, primidone, nitrates and disopyramide.
preparations (Buscopan®) and also in an injectable formulation in
combination with metamizole (dipyrone) (Buscopan Compositum®;
4 mg/mL butylscopalamine, 500 mg/mL metamizole); the latter is a Antihistamines
pyrazoline drug with anti-inflammatory, analgesic and antipyretic
properties. EXAMPLES
Atropine Diphenhydramine (Benadryl®), dimenhydrinate
• The standard dose rate is 0.02–0.04 mg/kg, IM or SC (Dramamine®)
Propantheline
• The dose for both dogs and cats is 0.25 mg/kg PO q.8 h
Butylscopalamine
• In dogs, the primary indication is as a long-acting antispas-
modic at a dose of 0.5 mg/kg IM or PO q.12 h (sole prepara- Clinical applications
tions) or 0.1 mg/kg IV or IM (in combination with metamizole) Antihistamines are primarily indicated for treatment
and prevention of motion sickness in the dog.
Mechanism of action
Adverse effects Antihistamines block histamine receptors in the CTZ
● The major problem with anticholinergics is that they and vestibular pathways. Histamine receptors in CTZ
also affect M2-receptors, potentially causing delayed are involved in motion sickness in the dog but not in
gastric emptying and ileus. This may potentiate vom- the cat.
iting and exacerbate gastric hypomotility, which In addition to its antihistaminergic effects, diphen-
occurs in many disorders causing vomiting. These hydramine has substantial sedative, anticholinergic,
476
Ch019-S2858.indd 476 11/19/2007 2:28:57 PM
ANTIULCER DRUGS
antitussive effects and local anesthetic effects. The anti- Relevant pathophysiology
cholinergic action may in fact be the main mechanism
by which it is effective in motion sickness, as there are The protective barrier that prevents gastric mucosa from
muscarinic receptors in the vestibular system. being damaged by gastric acid includes the following
factors.
● Mucus, with bicarbonate incorporated into the
Formulations and dose rates mucosal gel layer.
● High epithelial turnover (thus a high metabolic rate
DOGS AND CATS and oxygen requirement).
Diphenhydramine ● Tight junctions and lipoprotein layer of epithelial
• 2–4 mg/kg PO, IM q.8-12 h cells.
Dimenhydrinate ● A rich vascular supply.
• 4–8 mg/kg PO, IM q.8 h ● Prostaglandins – PGE series and PGI2 are
protective:
– inhibit gastric acid secretion
– maintain mucosal blood flow
Pharmacokinetics – involved in secretion and composition of healthy
The pharmacokinetics of these drugs have not been mucus
studied in domestic species. In humans diphenhydr- – may be intercellular messengers for stimulus of
amine is well absorbed after oral administration but mucosal cell turnover and migration.
systemic bioavailability is only 40–60% because of first-
pass metabolism. Diphenhydramine and dimenhydri- Gastrointestinal ulceration may be associated with a
nate are metabolized in the liver and largely excreted as number of events.
metabolites in urine. ● Drugs (aspirin, phenylbutazone, corticosteroids)
● Uremia (toxins, increased gastrin)
Adverse effects ● Liver disease (cause not known)
● CNS depression (e.g. lethargy, somnolence, ● Stress
paradoxical excitement – cats). The sedative effects ● Increased production of HCl (mast cell tumor at
may diminish with time. any site, gastrin-producing tumor of the pancreas
● Anticholinergic effects (e.g. dry mouth, urinary (Zollinger–Ellison syndrome))
retention). ● Hypotension, e.g. during surgery,
● Gastrointestinal side effects (e.g. vomiting and hypoadrenocorticism
diarrhea) are uncommon, but have been reported. ● Spinal cord disease
● These drugs should be used with caution if pyloric
Interruption of the gastric mucosal barrier allows back-
or proximal intestinal obstruction is suspected.
diffusion of gastric acid into the submucosa, which
● Use with caution in patients with hyperthyroidism,
causes mast cell degranulation, resulting in histamine
seizure disorders, cardiovascular disease,
release and subsequent further stimulation of acid
hypertension and closed-angle glaucoma; signs of
production by gastric parietal cells, which enhances
ototoxicity may also be masked by these drugs.
inflammation and edema in the submucosa. The aim of
antiulcer therapy is to repair the mucosal barrier directly,
Known drug interactions
reduce the amount of gastric acid produced or neutral-
Increased sedation can occur if antihistamines are com-
ize its effect and hence stop the vicious cycle of gut
bined with other CNS-depressant drugs. Antihistamines
damage.
may counteract the anticoagulatory effects of heparin
A number of classes of antiulcer drugs are available
or warfarin. Diphenhydramine may exacerbate the
and numerous agents are available within each class.
effects of adrenaline (epinephrine).
There are differences in mechanism of action amongst
groups and in potency amongst individual agents.
However, there is little information as to whether the
ANTIULCER DRUGS reported differences in potency relate to real differences
in clinical efficacy. An example is a recent study in
Clinical applications healthy laboratory dogs, which examined changes in
Antiulcer drugs are useful in the specific management of luminal pH after administration of four acid-blocking
gastrointestinal ulceration and reflux esophagitis. They drugs: ranitidine, famotidine, omeprazole and panto-
are not usually needed for treatment of simple acute prazole. Famotidine, pantoprazole and omeprazole sig-
gastritis. nificantly suppressed gastric acid secretion, compared
477
Ch019-S2858.indd 477 11/19/2007 2:28:57 PM
CHAPTER 19 GASTROINTESTINAL DRUGS
with saline solution, as determined by median 24-h pH, acetylcholine supplied to muscarinic receptors). Nizati-
and percentages of time pH was ≥3 or ≥4. However, dine may also have direct agonist effects on M3-
ranitidine did not. Of the four agents examined, twice- muscarinic receptors. In fact, nizatidine is more
daily omeprazole was most effective in suppressing commonly used primarily for its prokinetic activity than
gastric acid secretion. Although this suggests that proton as an acid-blocking drug.
pump inhibitors are the agents of choice, the study Cimetidine has an apparent immunomodulatory
involved healthy laboratory animals and it is not clear effect as it has been demonstrated to reverse suppressor
whether the criteria used in the study (luminal pH) were T cell-mediated immune suppression by blocking H2-
those which were most important in determining clini- receptors on suppressor T lymphocytes. It also increases
cal efficacy. lymphocyte response to mitogen stimulation. This effect
has been used clinically in the treatment of malignant
melanomas in people and gray horses. Cimetidine also
CLASSES OF ANTIULCER DRUGS possesses weak antiandrogenic activity.
Histamine-receptor antagonists
Formulations and dose rates
EXAMPLES
Cimetidine (Zitac®, Tagamet®), ranitidine (Zantac®), DOGS AND CATS
famotidine (Pepcid®), nizatidine (Axid®) Cimetidine
• 5–10 mg/kg PO, IV q.6–8 h
Ranitidine
• 1–2 mg/kg PO, SC, IV q.8-12 h
Famotidine
Clinical applications • 0.5–1.0 mg/kg PO, IV q.12–24 h
The histamine-receptor antagonists have efficacy in Nizatidine
treating gastric ulceration caused by a variety of disor- • 2.5–5.0 mg/kg PO, IV q.12–24 h
ders, including nonsteroidal anti-inflammatory drugs
(NSAIDs) and uremia. However, they do not appear to
be effective in preventing NSAID-induced ulcers. Raniti-
dine and nizatidine are also used as prokinetic agents Pharmacokinetics
(see below). Cimetidine
Oral bioavailability of cimetidine is reported to be
Mechanism of action 95% and serum half-life 1.3 h. Inhibition of gastric acid
These drugs act as competitive inhibitors at the hista- secretion peaks at 75% within 1.5 h and 50% inhibition
mine (H2) receptors on gastric parietal cells. H2- lasts about 2 h after an oral dose. The effects of the drug
receptors, when occupied by histamine and in the are gone after 5 h. Concurrent administration with food
presence of acetylcholine and gastrin, stimulate maximal delays drug absorption.
acid secretion. The H2-receptor is the dominant receptor Cimetidine decreases hepatic blood flow and inhibits
for stimulation of acid secretion. H2-receptor antago- hepatic microsomal enzymes. This can affect the metab-
nists cause a 70–90% decrease in gastric acid produc- olism of other drugs, although the clinical significance
tion. Ranitidine is reported to suppress gastric acid of this is uncertain. In humans, cimetidine is both
production to a greater extent than cimetidine (90% excreted unchanged by the kidneys and metabolized in
versus 75%); similarly, famotidine is more effective at the liver. More drug is excreted by the kidneys when
suppressing acid secretion than is ranitidine. However, administered parenterally than when given orally.
this does not appear to result in improved clinical effi-
cacy in dogs. By decreasing the amount of gastric acid Ranitidine
produced, H2-antagonists also proportionally decrease In dogs, the oral bioavailability of ranitidine is approxi-
pepsin secretion. mately 80% and serum half-life is 2.2 h. Food does not
Cimetidine and famotidine have no effect on lower affect absorption. Inhibition of gastric acid production
esophageal pressure or gastric emptying time and none peaks at 90% and 50% inhibition lasts about 4 h.
of these agents affects pancreatic secretion or biliary Ranitidine does not inhibit hepatic microsomal
secretion. However, ranitidine and nizatidine increase enzymes to the same extent as cimetidine. In humans,
lower esophageal sphincter pressure and have anti- ranitidine is both excreted in the urine via glomerular
cholinesterase activity which significantly enhances filtration and tubular secretion and metabolized in the
gastrointestinal motility (by increasing the amount of liver to inactive metabolites.
478
Ch019-S2858.indd 478 11/19/2007 2:28:57 PM
CLASSES OF ANTIULCER DRUGS
Famotidine ● Famotidine may exacerbate leukopenias if given
Famotidine is not completely absorbed after oral admin- concurrently with other bone marrow-suppressing
istration but hepatic first-pass metabolism is minimal. agents.
In humans, the oral bioavailability is approximately ● Nizatidine may increase salicylate levels in patients
40–50%. taking high doses of aspirin.
● Anticholinergic agents (e.g. atropine and propanthe-
line) may negate the prokinetic effects of ranitidine
Nizatidine and nizatidine.
In dogs, oral absorption is rapid and almost complete ● The increased intragastric pH associated with H2-
and there is minimal hepatic first-pass metabolism. antagonist administration may reduce the absorption
Although food improves oral bioavailability, the differ- of drugs that require an acid medium for dissolution
ence is not thought to be clinically relevant. Nizatidine and absorption, such as ketoconazole.
is metabolized in the liver to a number of metabolites ● It is recommended that at least 2 h elapses between
and at least one of these may have activity. dosing with cimetidine and giving antacids, metoclo-
pramide, digoxin or ketoconazole.
Adverse effects
● In animals, adverse effects appear rare at the doses Sucralfate
commonly used. Clinical applications
● In humans, side effects of cimetidine such as gyneco- Sucralfate is indicated for the symptomatic treatment
mastia and antiandrogenic activity and CNS signs of gastric ulceration from various causes. In humans,
(mental confusion, lethargy and seizures) have been sucralfate is as effective as antacids or H2-receptor
reported. antagonists in healing ulcers. It does not appear to be
● Occasionally, agranulocytosis may occur. successful, however, in preventing corticosteroid-induced
● Transient cardiac arrhythmias may occur if cimeti- ulceration in dogs subjected to spinal surgery. Its effi-
dine, ranitidine or famotidine are given cacy in preventing NSAID-induced ulcers is unproven
intravenously. in the dog. Sucralfate has also been used to treat oral
● Long-term used of H2-antagonists could cause hypo- and esophageal ulcers and esophagitis.
acidity and bacterial overgrowth in the stomach but
there is no clinical evidence that this is a serious
concern. There is no evidence that rebound hyperse- Mechanism of action
cretion occurs after stopping therapy with cimetidine Sucralfate is composed of sucrose octasulfate and alu-
or ranitidine. minum hydroxide, which dissociate in the acid environ-
● Cimetidine has been reported to cause a cutaneous ment of the stomach. Minimal systemic absorption
drug eruption in a cat. of either compound occurs. Sucralfate is structurally
● The dose of the H2-antagonists should be reduced by related to heparin but does not possess any appreciable
50% in patients with impaired renal function. anticoagulant activity. It is also structurally related to
sucrose but is not used as a sugar by the body.
When given orally, sucrose octasulfate reacts with
Known drug interactions hydrochloric acid and is polymerized to a viscous sticky
● Cimetidine can decrease hepatic microsomal enzyme substance that binds to the proteinaceous exudate
systems and thus theoretically can decrease hepatic usually found at ulcer sites. Because of electrostatic
metabolism of various drugs, including benzodiaze- charges, sucralfate preferentially adheres to ulcerated
pines, barbiturates, propranolol, calcium channel tissues. It protects the ulcer against hydrogen ion back-
blockers, metronidazole, phenytoin, quinidine, the- diffusion, pepsin and bile and therefore promotes ulcer
ophylline and warfarin. This has been demonstrated healing. The aluminum hydroxide theoretically neutral-
in the dog in a study of the pharmacokinetics of izes gastric acid but this antacid activity is not believed
verapamil when cimetidine was administered concur- to be clinically important.
rently. The clinical significance of this effect has It was believed that the formation of a physical pro-
not been established, although there are anecdotal tective barrier was the major mechanism by which
reports of cimetidine therapy adversely affecting sucralfate assisted ulcer healing. However, it is now
dogs receiving phenobarbital. Ranitidine inhibits micro- believed that the major drug actions of sucralfate are
somal enzyme systems to a much lesser (5–10-fold) related to stimulation of mucosal defense and reparative
degree. mechanisms, possibly related to stimulation of local
● Cimetidine and ranitidine may decrease the renal PGE2 and PGI2 production. Sucralfate also inactivates
excretion of procainamide. pepsin, adsorbs bile acids and is believed to be
479
Ch019-S2858.indd 479 11/19/2007 2:28:57 PM
CHAPTER 19 GASTROINTESTINAL DRUGS
cytoprotective by stimulating prostaglandin synthesis. It Misoprostol
does not significantly affect gastric acid output but may
slow gastric emptying appreciably. Clinical applications
Misoprostol (Cytotec®) is a synthetic prostaglandin
(PGE1). In human medicine, there are conflicting data
about whether misoprostol is as effective as H2-
Formulations and dose rates antagonists in healing ulcers. It is, however, most useful
for prevention of NSAID-induced ulceration and its effi-
LARGE DOGS cacy in this regard has been demonstrated in dogs. This
• 1 g PO q.8 h contrasts with the lack of prophylactic efficacy of other
antiulcer drugs. However, some studies suggest that it
SMALL DOGS may not be effective in preventing gastric ulceration
• 0.5 g PO q.8 h caused by high-dose glucocorticoid therapy (e.g.
methylprednisolone).
CATS Other less common uses include intravaginal admin-
• 0.25–0.5 g PO q.8–12 h
istration in conjunction with PGF2 for pregnancy termi-
It is preferable to administer sucralfate at least 60 min prior to
feeding.
nation in dogs (mid to late gestation). It has also been
reported to be effective in reducing ciclosporin-induced
toxicity and one study suggested some efficacy in treat-
ment of atopic dermatitis in dogs.
Pharmacokinetics Mechanism of action
Only 3–5% of an oral dose of sucralfate is absorbed Misoprostol has gastric antisecretory and mucosal pro-
and this is excreted unchanged in urine within 48 h. The tective effects as it acts as a synthetic replacement for
remainder of the drug is excreted in feces within 48 h. PGE1. PGE1 inhibits hydrochloric acid through a direct
Sucralfate binds to the ulcer site for up to 6 h after oral action on gastric parietal cells, by suppressing the acti-
dosing. vation of histamine-sensitive adenylate cyclase. It also
inhibits gastrin secretion and increases gastric mucus
Adverse effects formation. It increases blood flow to the mucosa, which
● Because very little drug is absorbed systemically, no increases the oxygen and nutrient supply to the healing
systemic toxicities have been reported. mucosa, ultimately enhancing epithelialization.
● The only reported side effect in humans is
constipation. Formulations and dose rates
Known drug interactions Misoprostol is not currently approved for veterinary use in any country.
● Recommendations vary concerning whether con- Although the most common recommendation is for q.8 h dosing, a
current administration of H2-antagonists decreases recent study examining effects on aspirin-induced gastric ulceration
sucralfate dissolution. Although it was believed that suggested that q.12 h dosing was as effective.
sucralfate required an acid environment for dissolu-
tion, a study in rats indicated that sucralfate pre- DOGS
• 2–5 µg/kg PO q.8–12 h
vented mucosal injury in both acidic and neutral
environments. However, as there are no definitive
studies in dogs and cats, it is probably prudent where
practical to administer sucralfate 30 min before an Pharmacokinetics
H2-antagonist if both drugs are used. Misoprostol pharmacokinetics are similar in dogs and
● Sucralfate may have the ability to bind other drugs humans. It is absorbed extensively after oral admin-
but no clinically important drug interactions have istration in dogs, although there is significant first-pass
been reported. However, it is recommended that metabolism. It undergoes rapid esterification to its free
drugs such as tetracyclines, digoxin, fluoroquino- acid, which is the active form. It is further metabolized
lones and aminophylline should not be given within in several tissues (biotransformed via oxidation to inac-
2 h of administering sucralfate. tive metabolites) and is excreted mainly in urine. Both
● Sucralfate can bind to and interfere with the absorp- misoprostol and its acid are relatively highly protein
tion of fat-soluble vitamins (e.g. A, D, E and K). bound. In humans the serum half-life of misoprostol is
Therefore, avoid giving this medication concurrently about 30 min and its duration of pharmacological effect
with enteral feeding preparations. 3–6 h.
480
Ch019-S2858.indd 480 11/19/2007 2:28:57 PM
CLASSES OF ANTIULCER DRUGS
Adverse effects prazole were more effective than either famotidine or
● Misoprostol can induce parturition or abortion as a ranitidine. Nevertheless, given that the study was in
result of luteolysis and myometrial contractions and healthy dogs, it is not clear whether the differences
is therefore contraindicated in pregnant animals noted relate to clinical efficacy.
unless intended as an abortifacient. Excellent long-term clinical outcomes have been
● Diarrhea, abdominal pain, flatulence and vomiting reported in humans and dogs with nonresectable gastri-
are relatively frequent side effects, although they are nomas treated with omeprazole. Omeprazole has been
often transient and resolve over several days. They reported to be useful in dogs in management of severe
can be minimized by dosage adjustment and giving erosive esophagitis, gastritis or gastric ulcer disease
the dose with food. refractory to therapy with H2-receptor antagonists and
● Life-threatening diarrhea has been reported in sucralfate. It has been used successfully to treat severe
humans with inflammatory bowel disease, so it erosive esophagitis in one cat but had no effect in two
would be prudent to avoid or use the drug with similarly affected cats.
caution in dogs with this disorder. One recent study demonstrated that omeprazole has
● Misoprostol should not be used in patients with some efficacy in preventing exercise-induced gastritis in
known hypersensitivity to prostaglandins or prosta- racing Alaskan sled dogs. In another study, omeprazole
glandin analogs. did not reduce mechanically induced gastric ulceration
● Some prostaglandins and prostaglandin analogs or prevent aspirin-induced gastritis in dogs, although
(although not misoprostol to date) have precipitated there was a trend that suggested that omeprazole was
seizures in epileptic humans. more effective than cimetidine in this regard. However,
a further study demonstrated limited efficacy, in both
Known drug interactions treating and preventing gastric mucosal lesions, in dogs
● The presence of food decreases the rate but not with acute degenerative disc disease treated with
extent of drug absorption. corticosteroids.
● Bioavailability is reduced by concomitant use of
antacids but this may not be clinically significant.
● Magnesium-containing antacids may exacerbate Mechanism of action
diarrhea induced by misoprostol. Omeprazole, a substituted benzimidazole, is a proton
pump inhibitor that binds to and irreversibly blocks
Special considerations H+/K+-ATPase, thereby blocking gastric acid secretion.
Pregnant women should handle the drug with caution Omeprazole inhibits gastric acid secretion stimulated by
(check label warning). any secretagogue, in contrast to H2-receptor antago-
nists, which only suppress gastric acid production
Proton pump inhibitors stimulated by histamine. Because it is a weak base,
omeprazole accumulates in the acid compartment of the
parietal cell; therefore its effect persists after the drug is
EXAMPLES
no longer detectable in blood. Omeprazole is inactive at
The main agent used in veterinary medicine is omeprazole physiological pH and so does not affect ATPase else-
(Prilosec®, Losec®). Other drugs in this group are now where in the body.
used in humans (e.g. lansoprazole, pantoprazole) but there Omeprazole has a longer duration of action than the
is limited information about their use in companion animals. H2-antagonists and most recommendations are for
once-daily dosing. However, a recent study reported
that twice-daily omeprazole maintained gastric lumen
pH > 3 throughout a 24-h period, whereas q.24 h dosing
Clinical applications did not. Whether it is necessary to maintain pH > 3 to
Omeprazole has slightly greater efficacy in promoting achieve effective ulcer healing is not clear. Given the cost
ulcer healing in humans than H2-antagonists but is and convenience of once-daily dosing, this protocol is
more expensive. Its use in veterinary medicine is usually likely to remain the most common approach, with more
restricted to refractory ulcers or ulcers associated with frequent dosing used for refractory cases only.
gastrinomas or mastocytosis. However, some veterinary The antisecretory effects increase with each dose
gastroenterologists use omeprazole as their first-choice until the drug attains a steady-state inhibition. In
antiulcer drug. Such an approach is supported by the dogs, gastric acid output is reduced by about 30% in
study previously referred to assessing efficacy and dura- the first 24 h after an oral dose of 0.7 mg/kg and after
tion of gastric acid suppression, by measuring luminal five doses gastric acid production is almost completely
pH, in healthy research dogs; omeprazole and panto- inhibited.
481
Ch019-S2858.indd 481 11/19/2007 2:28:57 PM
CHAPTER 19 GASTROINTESTINAL DRUGS
Formulations and dose rates Known drug interactions
● Inhibition of P450 hepatic enzymes may decrease
Omeprazole is labeled for equine use in some countries but not, to hepatic clearance of some drugs such as diazepam,
the authors’ knowledge, for small animal use. The drug is rapidly phenytoin and warfarin.
degraded by acid, so is formulated as 20 mg enteric-coated granules ● Drugs that require a low pH for optimal absorption
in a gelatin capsule. For dogs less than 20 kg, the enteric-coated (e.g. ketoconazole, ampicillin) may have reduced
granules must be repackaged in a gelatin capsule. absorption, as omeprazole increases gastric pH.
● In humans, omeprazole can occasionally cause bone
DOGS marrow suppression, which may be exacerbated if
• 0.5–1.0 mg/kg PO q.24 h (for ulcer management). Consider
used with other drugs that also suppress
q.12 h dosing in refractory cases. A pragmatic dosing schedule
hematopoiesis.
has been recommended as follows:
one 20 mg capsule daily for dogs weighing more than 20 kg
0.5 × 20 mg capsule daily for dogs weighing less than 20 kg Nonsystemic antacids
0.25 × 20 mg capsule daily for dogs weighing less than 5 kg
• 0.7–2.0 mg/kg PO q.12–24 h (for esophagitis) EXAMPLES
CATS Nonsystemic antacids include a variety of oral preparations
• 0.7 mg/kg PO q.24 h (for ulcer management). that contain aluminum hydroxide, calcium carbonate and
magnesium compounds.
Pharmacokinetics
Omeprazole is rapidly absorbed from the gut and dis-
Clinical applications
Nonsystemic antacids are probably most frequently
tributed widely but primarily in gastric parietal cells. It
used in the management of uremia, as aluminum
is metabolized extensively in the liver to at least six dif-
hydroxide binds phosphate, thus reducing hyperphos-
ferent metabolites, which are excreted principally in the
phatemia as well as having an antacid effect.
urine and also via bile into feces. Significant hepatic
dysfunction can reduce the first-pass effect of the drug,
increasing the systemically available drug and prolong-
Mechanism of action
Nonsystemic antacids act to neutralize hydrochloric
ing its duration of action. Omeprazole inhibits hepatic
acid, bind bile acids, decrease pepsin activity and pos-
microsomal enzymes to a similar degree to cimetidine.
sibly stimulate local prostaglandin (PGE1) production.
Preparations are usually a combination of aluminum
Adverse effects
hydroxide and magnesium hydroxide to maximize the
● There is limited information on veterinary use of
buffering capabilities of each compound. Magnesium
omeprazole but anecdotal reports suggest that it is
causes increased bowel motility and aluminum causes
well tolerated in dogs and cats.
decreased motility, which is another reason why the two
● The main potential side effects include gastrointesti-
are usually combined. Both magnesium hydroxide and
nal signs (anorexia, nausea, vomiting, flatulence,
calcium carbonate have a short, rapid effect; aluminum
diarrhea), hematological abnormalities, urinary tract
hydroxide has a slow, persistent effect.
infections, proteinuria and CNS disturbances.
Administration of antacid medications poses difficul-
● Long-term therapy has been reported to cause revers-
ties in veterinary patients because of the high volume
ible gastric hypertrophy in dogs because of the
and frequency of treatment required to prevent rebound
trophic effect of gastrin. Gastric hypertrophy has not
acid secretion. Nevertheless, the clinical efficacy of
been detected in dogs treated for 20 d.
antacid tablets was recently shown to be similar to
● In rats, long-term therapy is reported to cause gastric
higher doses of antacid liquids or cimetidine in
hypertrophy and carcinoids. Similar changes have
humans.
been found with long-term ranitidine therapy. There
is a concern that similar changes may develop after
long-term therapy in other species. However, given
that similar changes have not been detected in
Formulations and dose rates
humans, the relevance of this side effect is not clear. Although inexpensive, nonsystemic antacids must be administered
Nevertheless, as in humans, most clinicians do not orally (which may be difficult in a vomiting patient) and frequently,
recommend extending therapy beyond 8 weeks, which results in poor owner compliance.
unless the benefits outweigh potential risks.
482
Ch019-S2858.indd 482 11/19/2007 2:28:57 PM
PROKINETIC DRUGS
• Dosages are empirical as no specific dosages have been
ous combinations have been suggested, but those which
defined for animals have been critically evaluated include the following.
Tablets (e.g. aluminum hydroxide 500 mg) can be administered at ● Amoxicillin (20 mg/kg PO q.12 h for 14 d), metro-
10–30 mg/kg PO q.8 h nidazole (20 mg/kg PO q.12 h for 14 d) and famoti-
For liquid preparations (e.g. aluminum hydroxide gel 4% w/v), usual dine (0.5 mg/kg PO q.12 h for 14 d) in dogs.
doses are generally in the order of 5–10 mL PO q.8 h ● Clarithromycin (30 mg PO q.12 h for 4 d), metroni-
To be effective, antacids must be administered at least every 4 h dazole (30 mg PO q.12 h for 4 d), ranitidine (10 mg
PO q.12 h for 4 d) and bismuth subsalicylate (40 mg
PO q.24 h for 4 d) in H. heilmanii-infected cats.
● Azithromycin (30 mg PO q.24 h for 4 d), tinidazole
Adverse effects (100 mg PO q.24 h for 4 d), ranitidine (20 mg PO
● Calcium-containing antacids tend to promote consti- q.24 h for 4 d) and bismuth subsalicylate (20 mg PO
pation; magnesium promotes looser feces and alumi- q.12 h for 4 d) in H. heilmanii-infected cats.
num reduces gastric motility and delays gastric ● Amoxicillin (20 mg/kg PO q.8 h for 21 d), metroni-
emptying. dazole (20 mg/kg PO q.8 h for 21 d) and omeprazole
● If antacids are administered infrequently they may (0.7 mg PO q.24 h for 21 d) in H. pylori-infected
actually result in increased gastric acid production. cats.
● Administration of excessive calcium-containing ant- ● Amoxicillin (20 mg/kg PO q.12 h for 14 d), clar-
acids may predispose to renal calculi. ithromycin (7.5 mg/kg PO q.12 h for 14 d) and
● Hypophosphatemia and accumulation of aluminum metronidazole (10 mg/kg PO q.12 h for 14 d) in H.
are potential sequelae with long-term use of alumi- pylori-infected cats.
num-containing antacids.
Thus if a decision is made to eradicate Helicobacter
species, use of one of the above protocols is
Known drug interactions
recommended.
Antacids will interfere with gastric absorption of con-
currently administered drugs such as digoxin, tetracy-
clines and fluoroquinolones.
DRUG COMBINATIONS
THERAPY FOR ERADICATION OF
HELICOBACTER SPP Hyoscine and dipyrone
Spasmogesic®, Buscopan® and other trade names
Helicobacter pylori is the major cause of pyloric ulcer describe drug combinations containing the anticholiner-
disease in humans. A number of Helicobacter species gic hyoscine and the NSAID dipyrone. Although this
have been shown to colonize the gastric mucosa of cats combination is relatively commonly used in small
and dogs, including H. felis and H. heilmanii, and animals, its value in the management of gastrointestinal
gastric spiral organisms are often identified during his- disease is questionable.
topathological inspection of gastric mucosal biopsy The potential concerns with anticholinergic usage in
specimens procured from both symptomatic and asymp- the management of vomiting or diarrhea are discussed
tomatic companion animals. Therefore, it remains con- elsewhere in this chapter. The potential adverse effects
troversial as to whether or not Helicobacter species are from dipyrone are discussed in Chapter 13 on
a significant cause of disease in small animals. Certainly, NSAIDs.
disease is not the result of simple infection and disease
pathogenesis is likely more complicated. Instead, it is
thought that these organisms are normal commensal
bacteria and that most dogs and cats can tolerate their PROKINETIC DRUGS
presence. Current theories on the pathogenesis of
Helicobacter-associated gastritis center on the hypothe- Treatment of certain conditions such as delayed gastric
sis that disease manifests after a breakdown in mucosal emptying and suboptimal colonic motility is facilitated
tolerance to Helicobacter species. As a consequence, by the use of prokinetic drugs. These include meto-
many clinicians choose to eradicate Helicobacter species clopramide (discussed previously), ranitidine (again
in patients with chronic vomiting and biopsy-proven described previously), erythromycin and cisapride.
gastric inflammation. Cisapride was previously the prokinetic of choice in
Treatment usually involves administering a combina- small animals. However, this drug was recently impli-
tion of antibacterial and acid-blocking drugs. Numer- cated in causing adverse cardiac events in people. This
483
Ch019-S2858.indd 483 11/19/2007 2:28:57 PM
CHAPTER 19 GASTROINTESTINAL DRUGS
is unfortunate given that, in most cases, the patients
had pre-existing risk factors and/or were receiving other
Formulations and dose rates
medications known to inhibit the hepatic CYP3A4 Erythromycin is available in numerous preparations as different
enzyme system and metabolism of cisapride. However, esters, including erythromycin estolate, erythromycin ethylsuccinate,
despite this, cisapride has recently been withdrawn from erythromycin lactobionate and erythromycin gluceptate. Erythromycin
the market in many countries, including the USA and is also available as the base form. Oral preparations (tablets, capsule
UK. Given that the drug is no longer widely available, and suspension) are used most commonly for the prokinetic effects.
its use can no longer be considered. Further, related Tablets and capsules usually contain erythromycin as base, stearate
novel compounds developed as alternatives to cisapride ester or ethylsuccinate ester; the suspension usually contains eryth-
(e.g. prucalopride) have failed to gain approval for romycin ethylsuccinate. It is likely that pharmokinetics and toxicity
vary depending upon the exact ester used.
similar reasons.
Tegaserod (Zelmac®) is an aminoguanidine indole
DOGS AND CATS
derivative of serotonin, which has recently become • 0.5–1.0 mg/kg PO q.8 h
available in North America. It acts as a selective partial
agonist highly selective for 5-HT4 receptors; various
studies have demonstrated prokinetic effects including
stimulation of peristaltic activity in vitro, increased Pharmacokinetics
canine intestinal and colonic motility and transit, Erythromycin is absorbed after oral administration in
reduced visceral afferent firing or sensation in response the upper small intestine and a number of factors may
to distension in animals, accelerated gastric, small influence bioavailability. These include the form of the
bowel and colonic transit in healthy patients and drug, acidity of the gastrointestinal tract, presence of
increased small bowel transit in human patients with food and gastric emptying time. Given that the base is
constipation-predominant irritable bowel syndrome. acid labile, it should be administered on an empty
Thus, in time it may prove to be a suitable alternative stomach. Erythromycin is partly metabolized in the liver
to cisapride. However, the authors are not aware of any to inactive metabolites, although most is excreted
clinical trials of this drug in companion animals and unchanged through the biliary route. Some active
more work is required before its use can be recom- erythromycin is reabsorbed after biliary excretion,
mended in veterinary patients. potentially prolonging the activity of each dose. The
elimination half-life in cats and dogs is estimated to be
60–90 min.
Erythromycin
Adverse effects
Clinical applications ● The main side effect of erythromycin is vomiting,
Erythromycin has antibacterial activities (not discussed although this is less common when administered at
further here) but at subantimicrobial doses can also be the doses used for prokinetic effect, and enteric-
used as a prokinetic. It is used most commonly to coated products may further reduce the frequency of
improve the rate of gastric emptying, but may also be vomiting. Other gastrointestinal signs can also be
beneficial in the treatment of esophageal reflux. seen, including anorexia and diarrhea.
● When used for its prokinetic effects, clinical signs
may deteriorate rather than improve because the
Mechanism of action drug can stimulate the emptying of larger than
Erythromycin is a macrolide antibiotic which, at doses normal food particles from the stomach.
below the level required for antimicrobial activity, has ● In humans, erythromycin estolate is occasionally
prokinetic activities. In many species (e.g. cats, rabbits associated with cholestatic hepatitis, although such
and humans), the effect is due to the drug acting on an adverse effect has not been reported in a veteri-
motilin and 5-hydroxytryptophan (5-HT3) receptors, nary species. Nevertheless, as a precaution, this drug
thus stimulating migrating motility complexes and ante- should not be given to patients with pre-existing
grade peristalsis. However, the mechanism of action in hepatic dysfunction.
dogs is less well understood, but it is most likely via ● Erythromycin should not be used in patients who are
action on 5-HT3 receptors. Gastric emptying is enhanced hypersensitive to it.
by stimulating antral contractions, whilst lower esopha-
geal pressure is also increased. However, given that Known drug interactions
erythromycin has most effect in stimulating interdiges- ● Erythromycin may increase gastrointestinal absorp-
tive activity, beneficial effects on gastric emptying during tion of digoxin, potentially leading to digoxin
the digestive phase are less clear. toxicity.
484
Ch019-S2858.indd 484 11/19/2007 2:28:58 PM
LAXATIVE THERAPY
● Erythromycin may increase serum concentrations of Psyllium
theophylline and terfenadine. In humans, this effect • DOGS: 5 mL (1 teaspoonful) to 30 mL (2 tablespoonfuls) PO
is particularly important because this combination q.12–24 h
has been associated with the development of fatal • CATS: 5–20 mL (1–4 teaspoonfuls) PO with each meal
arrhythmias. Sterculia
● The metabolism of methylprednisolone may be DOGS and CATS
inhibited and the clearance of theophylline may be • <5 kg: 1.5 g PO q.24 h
increased by concurrent erythromycin administra- • 5–15 kg: 3 g PO q.12–24 h
tion. The significance of the former interaction is not • >15 kg: 4 g PO q.12–24 h
clear, whilst the interaction with theophylline may
lead to theophylline toxicity and close pharmacologi-
cal monitoring is recommended.
● Erythromycin may prolong prothrombin times and Emollient laxatives
lead to bleeding when given to a patient previously Emollient laxatives are anionic detergents that reduce
stabilized on warfarin. surface tension, thus increasing the miscibility of water
● Other reported human drug interactions of erythro- and lipid digesta. This thereby increases lipid absorption
mycin include ciclosporin, carbemazepine and tri- and impairs the absorption of water. There is some evi-
azolam. However, the significance of such interactions dence that docusate sodium (dioctyl sodium sulfosucci-
for veterinary species is less well established. nate), the main agent used in this group, also increases
● Administration of erythromycin may falsely elevate colonic mucosal cell cAMP concentration and thus
serum concentrations of ALT and AST if colorimetric increases both ion secretion and fluid permeability.
assays are used and urinary catecholamine measure- Most of the effect of this drug is local, although some
ments may be altered in a similar manner. drug is absorbed from the small intestine and then
excreted into bile.
Docusate is present as the sole agent in enemas (e.g.
Fletcher’s enemette, Dioctynate®, Enema-DSS®, Docu-
LAXATIVES, ENEMAS AND soft®, Ther-evac®) and some oral preparations (tablets,
BOWEL CLEANSERS capsules and syrups of various strengths) or in combina-
tion products with dantron, a fecal softener (e.g. ‘con-
These drugs are commonly used to evacuate the large
danthrusate’, Docusol®; 50 mg dantron and 60 mg
bowel and the main pathological indications are consti-
docusate/5 mL). The enema preparations are all veteri-
pation and obstipation.
nary-licensed products, but the oral preparations are
not.
Clinical efficacy has not been established definitively.
Nevertheless, they are safe agents when used in healthy
LAXATIVE THERAPY
well-hydrated individuals. However, these preparations
should be avoided in patients with pre-existing electro-
A number of groups of laxative drugs exist, including
lyte or fluid deficits. These drugs have few reported side
bulk-forming laxatives, emollient laxatives, lubricant
effects when used at recommended doses; cramping,
laxatives, hyperosmotic laxatives and stimulant
diarrhea and intestinal mucosal damage have been
laxatives.
reported, whilst liquid oral preparations can sometimes
cause pharyngeal irritation. Concurrent administration
Bulk-forming laxatives of mineral oil is not recommended, because enhanced
absorption of the oil may occur. If overdose occurs, it
Most of the available agents in this group are dietary is advisable to monitor hydration and systemic electro-
fiber supplements which contain poorly digestible poly- lyte status. If concurrent administration is essential, it
saccharides and celluloses. These are mainly derived is advisable to stagger dosing by at least 2 h.
from cereal grains, wheat bran and psyllium. This group
of agents can either be given in a purpose-formulated
‘prescription’ diet or as a preparation added to the exist-
Docusate sodium (dioctyl sodium sulfosuccinate)
ing diet. Examples include psyllium (Vetasyl®, Metamu-
• DOGS: 50–300 mg PO q.12–24 h; 10–15 mL of a 5% solution
cil®, Genifiber®, etc.) and sterculia (Peridale®). Dietary mixed with 100 mL of water and instilled per rectum
fiber supplements are usually well tolerated, more effec- • CATS: 50 mg PO q.12–24 h; 2 mL of a 5% solution mixed with
tive and more physiological than the other groups of 50 mL of water and instilled per rectum
laxatives.
485
Ch019-S2858.indd 485 11/19/2007 2:28:58 PM
CHAPTER 19 GASTROINTESTINAL DRUGS
Lubricant laxatives should not be administered to animals with gastric
retention, suspected gastrointestinal obstruction, bowel
As their name suggests, these agents have lubricating perforation, megacolon or in patients with reduced
properties. They impede colonic water absorption and swallowing function (which may predispose to inhala-
make it easier for feces to be passed. Some reports have tion pneumonia). Occasional vomiting may be seen,
suggested that up to 60% of these preparations may be especially if the maximal dose has been administered.
absorbed, although most reports dispute these findings. Otherwise, this drug preparation is very well tolerated.
Examples include paraffin (mineral oil) and white soft Given that gastrointestinal motility is affected, the
paraffin (white petrolatum). These agents have only absorption of other drugs may be affected by adminis-
moderate effects and are only likely to be of use in mild tration of bowel cleansers.
cases of constipation. Preparations of paraffin include
generic preparations (e.g. liquid paraffin) and white soft
paraffin (Katalax®). DOGS
In humans, use of these drugs is contraindicated in • Withhold food for 18–24 h prior to colonoscopy. Give 2–3 doses
young or old patients, debilitated patients and pregnant of 20–30 mL/kg, 4–6 h apart, by orogastric intubation. Prior to
patients. In addition, these agents should be avoided in the procedure, a warm water enema should be administered
patients with pre-existing dysphagia, regurgitation or
CATS
vomiting. The main side effect is lipoid pneumonia sec-
• Withhold food for 18–24 h prior to colonoscopy. Give 2 doses of
ondary to inhalation (paraffin is tasteless and may not 30 mL/kg, 4–6 h apart, by orogastric intubation. Prior to the
elicit normal swallowing when syringed). When signifi- procedure, a warm water enema should be administered
cant quantities of mineral oil are absorbed, granuloma-
tous reactions may develop in the liver, spleen and
mesenteric lymph nodes. Long-term use is not recom-
mended since it may predispose to malabsorption of Stimulant laxatives
fat-soluble vitamins (vitamins A, D, E and K), although This group stimulates propulsive motility and the
the significance of this has not been determined main agent used in companion animals is bisacodyl
clinically. Docusate sodium should not be administered (Ducolax®). The exact mechanism of action is unclear;
concurrently with mineral oil, because it may enhance the two putative mechanisms are promoting peristalsis
absorption. through direct stimulation of intramural neural plexuses
and increasing fluid and ion accumulation in the large
DOGS intestine and thus increasing catharsis. This drug can
• Use liquid paraffin (mineral oil) 15–30 mL (1–2 tablespoonfuls) be given as sole therapy, or in combination with other
PO per meal, as required laxative preparations such as fiber supplements. The
drug is reported to be minimally absorbed after oral
CATS administration and onset of action is 6–10 h. Relatively
• Adult cats: 1 inch of white soft paraffin paste PO q.12–24 h few side effects have been reported but include cramp-
• Kittens: 0.5 inch of white soft paraffin paste PO q.12–24 h ing, nausea and diarrhea. Stimulant laxatives are con-
traindicated in cases of intestinal obstruction not caused
by constipation, when rectal bleeding is present or if
Hyperosmotic laxatives intestinal perforation is suspected. Bisacodyl should not
Hyperosmotic laxatives consist of agents which are be given concurrently with milk or antacids as both can
poorly absorbed in the gastrointestinal tract but osmoti- cause premature disintegration of the enteric coating.
cally active. Lactulose is a nondigestible carbohydrate Further, this drug should not be administered concur-
used for both treatment of constipation and manage- rently with other oral medications (e.g. not ≤2 h),
ment of hepatic encephalopathy (see below). Polyethyl- because its effect on gastrointestinal motility may affect
ene glycol 3350 (PEG) also acts as an osmotic agent and absorption. Daily administration is inadvisable because
is commonly included in bowel-cleansing solutions used of potential injury to myenteric neurones when used
prior to lower bowel colonoscopy. Most preparations chronically.
used for this purpose also contain sodium sulfate, which
minimizes sodium absorption and other electrolytes
DOGS
(e.g. bicarbonate, potassium and chloride) to maintain
• 5–20 mg PO q.24 h
isotonicity and prevent any net gain or loss in the secre-
tion of water or electrolytes in the intestine. CATS
A variety of preparations of PEG are available, e.g. • 2–5 mg PO q.24 h
Golytely®, Klean Prep®, Colyte® and Nulytely®. PEG
486
Ch019-S2858.indd 486 11/19/2007 2:28:58 PM
MOTILITY-MODIFYING DRUGS
slowing transit may be counterproductive. Reduced
ANTIDIARRHEAL DRUGS motility may allow enterotoxin-producing organisms to
remain in the small intestine, resulting in increased fluid
For most cases of acute diarrhea, the mainstay of therapy loss. In addition, in cases of diarrhea caused by invasive
is to replace fluid losses, modify the diet and treat the bacteria, diarrhea probably has a protective function in
specific cause (infectious, immune-mediated, etc.) where hastening elimination of organisms. Slowing transit
possible. Treatment of diarrhea does not often require time may prolong the time bacteria are resident in the
use of drugs but they may be considered when relief of bowel, resulting in a greater opportunity for prolifera-
discomfort will benefit the patient, provided that their tion, invasion of the mucosa and absorption of toxic
use does not risk exacerbating the diarrhea or causing products. However, loperamide appears to be antisecre-
systemic effects. tory and therefore may have value in treating animals
with secretory diarrhea due to Escherichia coli. Anec-
MOTILITY-MODIFYING DRUGS dotally, opioids appear to be useful in the management
of fecal incontinence in some patients.
Intestinal transit time is predominantly determined by
the balance between peristalsis, which moves ingesta in Mechanism of action
an aboral direction, and segmental contractions, which Opioids increase the amplitude of rhythmic contraction
narrow the bowel lumen and increase the resistance to and decrease propulsive contractions. They directly affect
flow. Peristalsis is influenced by the cholinergic system intestinal smooth muscle, producing both tonic and
and gut hormones such as motilin. Segmental contrac- phasic contractions of the circular muscle. They also act
tions are cholinergic dependent. centrally and on synapses to augment segmentation.
Although it is theoretically possible to reduce diar- They either have no effect on longitudinal muscle or they
rhea by either decreasing peristalsis or increasing relax it. The net effect of these actions is to inhibit flow
segmental contractions, reducing peristalsis is of little of intestinal contents, delay gastric emptying and increase
clinical benefit and is generally contraindicated. This is the tone of the ileocolic valve and anal sphincter.
because, in most cases of diarrhea, the gut is hypomo- Some opioids, such as loperamide and to a lesser
tile, not hypermotile, and peristalsis and segmental con- extent diphenoxylate, also increase fluid and water
tractions are already reduced. absorption, possibly by a calcium-blocking effect or by
Gastrointestinal motility may be modified by two inhibition of calmodulin, the intrinsic calcium-binding
groups of agents: opioids, which increase segmental protein. Loperamide and diphenoxylate also inhibit the
contractions, and anticholinergic drugs, which decrease activity of secretagogues such as E. coli enterotoxin,
both segmental contractions and peristalsis. vasoactive intestinal peptide, bile acids and PGE2.
Finally, opiates may also enhance mucosal absorption
Opioids in the gastrointestinal tract.
Lomotil® contains atropine as well as diphenoxylate.
EXAMPLES This is to discourage abuse of the drug by people. At
Diphenoxylate (Lomotil®), loperamide (Imodium®), therapeutic doses of Lomotil® the atropine has no clini-
paregoric cal effect.
Formulations and dose rates
Clinical applications
There are no currently approved veterinary formulations of these
These drugs may be effective for the symptomatic treat-
drugs. Human formulations are available; paregoric is available as a
ment of diarrhea as they increase segmental contrac- liquid. Diphenoxylate and loperamide are available in tablet and liquid
tions, thus delaying gut transit time. They may relieve forms. Use of diphenoxylate in cats is not recommended.
abdominal pain and tenesmus and reduce the frequency
of defecation, although convincing clinical efficacy has DOGS AND CATS
not been observed in many veterinary patients. Paregoric
They are rarely required, however, in management • 0.05–0.06 mg/kg PO q.8 h
of diarrhea in small animals. Acute diarrhea is usually Loperamide
self-limiting with appropriate treatment and chronic • 0.1–0.2 mg/kg PO q.8 h
diarrhea does not usually respond to such therapy and
requires a definitive diagnosis to be established to allow DOGS ONLY
specific treatment to be instituted. Diphenoxylate
The use of motility modifiers is not without risk as • 0.1 mg/kg PO q.8 h
the diarrhea may be beneficial in removing toxins and
487
Ch019-S2858.indd 487 11/19/2007 2:28:58 PM
CHAPTER 19 GASTROINTESTINAL DRUGS
Pharmacokinetics Anticholinergic drugs
There are few data on the pharmacokinetics of the
Anticholinergics have little use in the management of
opioid agents in small animals. The morphine in parego-
diarrhea in small animals, although they are frequently
ric is absorbed in a variable fashion from the gastro-
prescribed, usually in combination products. As dis-
intestinal tract and rapidly metabolized in the liver,
cussed previously, most diarrheal disorders in small
resulting in serum concentrations that are much lower
animals are associated with a hypomotile rather than a
than those produced by morphine administered
hypermotile gut and the risk with anticholinergics is
parenterally.
that they will produce a dynamic ileus, especially if
In humans diphenoxylate is rapidly absorbed. Onset
electrolyte imbalances such as hypokalemia are also
of action occurs about 45 min after dosing and lasts for
present. Anticholinergics reduce but do not abolish peri-
3–4 h. In dogs, it has been stated that loperamide has a
stalsis and substantially decrease segmental contrac-
faster onset and longer duration of action than diphenox-
tions. As long as some peristaltic activity is present, no
ylate, although published clinical studies confirming this
matter how weak, it can propel liquid ingesta along the
appear to be lacking.
flaccid intestine and diarrhea will occur.
Although anticholinergics reduce gastric secretions,
including protein exudation induced by histamine, they
have little effect on intestinal secretions.
Adverse effects They may be justified in the short term for relief of
● In dogs, the most common side effects of opiates pain and tenesmus associated with large bowel inflam-
are constipation, sedation and bloating. Overdosage matory disease. They also may be indicated in stress-
with these medications can lead to significantly induced colitis where cholinergic mechanisms might be
reduced gastrointestinal motility (i.e. ileus) and involved.
delayed absorption.
● Signs of systemic opioid intoxication may occur Adsorbents and protectants
with use of the opioid antidiarrheals, particularly in
Kaolin and pectin
cats.
Kaolin and pectin are in many preparations that are
● Neurological disturbances such as ataxia, hyperex-
widely used for the management of diarrhea in small
citability, circling, head pressing, vocalization and
and large animals. They are purported to soothe irri-
prostration may occur with overdosage. In dogs
tated gastrointestinal mucosa and bind toxins and
there has been a suggestion that collies may be more
pathogenic bacteria. However, their clinical efficacy is
sensitive to the toxic effects of loperamide.
unproven. There is no evidence that kaolin and pectin
● Treatment of side effects or overdosage involves use
reduce gastrointestinal fluid or electrolyte loss and
of the opioid antagonist naloxone and recovery is
kaolin may in fact increase fecal sodium loss.
usually uneventful.
Many preparations contain combinations of kaolin
● Massive overdoses with the diphenoxylate/atropine
and pectin and/or antibacterials and/or anticholinergics.
preparations may also lead to atropine toxicity.
As discussed previously, the value of the latter two types
of compound in the treatment of diarrhea is limited in
small animals and may be detrimental.
Known drug interactions Montmorillonite
● Other CNS depressants such as anesthetic agents, Montmorillonite (Diarsanyl®) is an intestinal adsor-
antihistamines, phenothiazines, barbiturates and bent/protectant, which is used in the symptomatic
tranquilizers may cause increased CNS or respiratory treatment of companion animals with diarrhea. It is a
depression when used with opiate antidiarrheal trilamellar smectite clay, with a similar mechanism of
agents. action to that of kaolin. However, it is reported to have
● Opiate antidiarrheal agents are contraindicated in superior adsorbent properties. Most preparations of
patients receiving monoamine oxidase inhibitors, montmorillonite also contain simple sugars and electro-
e.g. l-deprenyl (selegiline), within at least 14 d. lytes. No adverse affects are known, but are likely to
However, the significance of this interaction in vet- be similar to that of kaolin preparations. Overdosage
erinary species is not clear given that this drug group would be expected to cause constipation. The main
is rarely used. formulation (Diarsanyl®) is a paste in 10 mL, 24 mL
● Plasma amylase and lipase concentrations may be and 60 mL multidose syringes. Each 10 mL of paste
increased for up to 24 h after the administration of contains 4.5 g of montmorillonite and the recommended
opiates. dose rate is as follows.
488
Ch019-S2858.indd 488 11/19/2007 2:28:58 PM
MOTILITY-MODIFYING DRUGS
DOGS
ucts is not recommended as the drug can be neurotoxic
• <7 kg: 1 mL PO q.12 h and is contraindicated in patients with renal impair-
• 7–17 kg: 2 mL PO q.12 h ment. Further, given that bismuth is radio-opaque, it
• 18–30 kg: 4 mL PO q.12 h may interfere with radiographic studies of the gastroin-
• 31–60 kg: 10 mL PO q.12 h testinal tract. Overdosage can result in salicylate toxic-
ity, especially in cats. A safe dose in dogs and cats is
CATS 0.25 mL/kg q.4–6 h. Dosages greater than 0.7 mL/kg
• 1 mL PO q.12 h could result in toxicity. Aside from this, changes in fecal
characteristics can be seen, i.e. color change to black or
green-black.
Activated charcoal Sulfasalazine
Activated charcoal has been used for many years in the Clinical applications
treatment of toxicosis. The drug is not absorbed from Sulfasalazine is indicated in the treatment of chronic
the gastrointestinal tract and is thought to have a local colitides (e.g. inflammatory bowel disease) in dogs and
effect, by adsorbing toxic substances and binding bacte- (less commonly) cats. Although well-controlled studies
rial toxins. However, it is not reported to be effective have not been performed in small animals, uncontrolled
for mineral acids or alkalis and, in fact, there is limited studies and widespread clinical use indicate that the
work supporting its efficacy. Recommended dosages are drug has convincing clinical benefit in patients with
in the range of 2–8 g/kg as an aqueous suspension per chronic colitis. It is not a panacea, however, and a
os. For example, administering 10 mL/kg of a 20% number of animals do not respond or relapse during or
slurry provides a dose equivalent to 2 g/kg. Given the after therapy.
volumes involved, this drug is usually given by oro- or Preparations containing only 5-aminosalicylic acid
nasogastric intubation. (5-ASA) (mesalazine, mesalamine) are now used in
Very rapid administration may induce emesis and human and veterinary medicine in the treatment of
charcoal can cause effects on fecal characteristics (e.g. ulcerative colitis. 5-ASA appears to retain the effective-
diarrhea, constipation, black feces). Aside from these, ness of sulfasalazine but reduces (but does not eliminate
there are no reported systemic adverse effects. Finally, altogether) the incidence of side effects by dispensing
activated charcoal can permanently stain objects with with the sulfonamide entity. The drug is administered
which it comes into contact and the powder has a ten- as a suppository or as an enteric-coated tablet to ensure
dency to float over wide areas. Therefore, care is advised that the majority of drug reaches the colon. Other drugs
during preparation. used in human colitis include olsalazine, which is two
molecules of 5-ASA linked by an azo bond. The clinical
value of this drug in veterinary medicine has yet to be
Bismuth subsalicylate established.
Bismuth subsalicylate is reported to be an effective agent
for treatment and prevention of enterotoxigenic diar-
rhea. Nausea, abdominal pain and diarrhea are reduced Mechanism of action
in humans with infective diarrhea treated with bismuth- Sulfasalazine is a combination of sulfapyridine and 5-
containing products. Bismuth subsalicylate has modest ASA, which is cleaved by colonic bacteria, resulting in
antibacterial effects against enteropathogens such as E. sulfapyridine being absorbed and ASA excreted in feces.
coli, Salmonella spp and Campylobacter jejuni. However, Given that the colonic concentrations of both sulfapyri-
it is sometimes used in combination protocols for dine and 5-ASA are higher than when given orally as
the eradication of Helicobacter species. The salicylate individual agents, it is not entirely established which is
moiety is believed to decrease intestinal secretion by responsible for the clinical effects. However, 5-ASA is
inhibiting prostaglandin production and inhibiting gen- probably the active ingredient, as a result of antiprosta-
eration of cAMP by the enterotoxin. glandin and antileukotriene activity. In addition, this
Preparations which contain bismuth subsalicylate agent is thought to have oxygen free radical-scavenging
(Pepto-Bismol®, Peptosyl®) can be clinically useful in actions, to interfere with phagocytic chemotaxis and
the management of acute diarrhea. However, such function and to inhibit cytokine and immunoglobulin
conditions usually resolve with appropriate nondrug production. NSAIDs such as aspirin that inhibit prosta-
therapy. glandin but not leukotriene synthesis are ineffective in
Reported side effects in humans include nausea and treating colonic inflammation and may actually worsen
vomiting. Long-term use of bismuth-containing prod- inflammatory bowel disease.
489
Ch019-S2858.indd 489 11/19/2007 2:28:58 PM
CHAPTER 19 GASTROINTESTINAL DRUGS
phenylbutazone, thiazide diuretics, salicylates and
Formulations and dose rates phenytoin. The clinical significance of these interac-
Sulfasalazine is available as tablets or liquid. Various dosage regimens
tions has not been established.
have been successfully used. ● Sulfasalazine may decrease the bioavailability of
folic acid or digoxin. Antacids may decrease the
DOGS oral bioavailability of sulfasalzine if administered
• Some clinicians recommend a dose of 10–15 mg/kg PO q.8– concurrently.
12 h for 2 weeks, then tapered to the lowest effective dose ● Antacids may decrease the oral bioavailability of
• Other reports suggest that higher doses are required, e.g. 20– sulfasalazine if administered concurrently.
50 mg/kg (up to a maximum of 1 g) PO q.8 h; from 2–4 weeks, ● As with other sulfonamides, sulfasalazine may affect
attempts can be made to taper the dose gradually (e.g. by blood thyroid concentrations, e.g. decreased total
reducing 25–50% of the dose every 2–4 weeks) to the lowest
and free T4, increased cTSH.
effective dose
• Therefore, it is usually recommended to start at a low dose
● Olsalazine may causes increases in plasma concentra-
(e.g. 12.5 mg/kg PO q.8 h) and increase this after 4 weeks if it tions of ALT and AST.
has been ineffective
• Olsalazine is used in dogs that cannot tolerate sulfasalazine.
The recommended dose is 10–20 mg/kg PO q.8 h APPETITE STIMULANTS
CATS The main appetite stimulants used in companion animals
• 10–20 mg/kg PO q.24 h. The reduced dosing interval is used in are the H1-receptor antagonists cyproheptadine and
light of increased sensitivity to salicylates in this species diazepam. In both drugs, the appetite stimulation is
effectively a ‘side effect’ of the indication for which they
were predominantly designed.
Pharmacokinetics Cyproheptadine also has serotonin antagonist and
After oral administration approximately 20–30% of the calcium channel-blocking properties. It is indicated for
drug is absorbed in the small intestine. Some of this short-term use as an appetite stimulant in cats; pro-
absorbed drug is believed to be excreted unchanged into found anorexia or chronic nutritional disorders are
the bile. Unabsorbed and biliary excreted drug is cleaved better managed with more intensive nutritional support,
in the colon by bacterial flora. Because the colonic i.e. tube feeding. The drug is well absorbed, almost
microflora is required to cleave the drug, sulfasalazine completely metabolized in the liver and metabolites are
is not effective against small bowel inflammation. The excreted in the urine. The main side effects are sedation
sulfapyridine component is rapidly absorbed but only a and anticholinergic effects (dry mucous membranes,
small percentage of the 5-ASA is absorbed; both are mydriasis); occasional reports of hemolytic anemia have
metabolized in the liver and excreted in the urine. been described.
Olsalazine is poorly absorbed and that which is absorbed Diazepam is used mainly for its anticonvulsant, anx-
is rapidly eliminated. Approximately 98% of an oral iolytic and skeletal muscle relaxant properties. However,
dose is thought to reach the colon. when used IV, it can be an effective appetite stimulant
in cats. Again, only short-term (and preferably single)
Adverse effects use is recommended. The IV preparation should be
● The major adverse effect, although uncommon, is injected slowly, since rapid administration may cause
keratoconjunctivitis sicca. Should decreased tear marked excitation. Thrombophlebitis has also been
production be recorded, this can be resolved by reported. The drug should be used with caution in
reducing the dose or discontinuing the drug patients with pre-existing or suspected renal or hepatic
altogether. insufficiency. The main side effects include muscle fas-
● Other occasional adverse effects include vomiting, ciculations, weakness, ataxia, behavior changes and
allergic dermatitis, cholestatic jaundice, hemolytic excessive sedation. Fulminant hepatic necrosis has also
anemia and leukopenia. been described in cats after oral administration (usually
● Drug hypersensitivity manifested as lethargy, pyrexia, for >5 d). Given that the IV preparation is used for
arthralgia and cutaneous drug eruption can occur appetite stimulation, the significance of this finding is
with sulfonamide drugs and has been reported with unclear. Nevertheless, cautious use is recommended.
the use of sulfasalazine.
CATS
Known drug interactions Cyproheptadine
● Sulfasalazine may displace other highly protein- • 1–4 mg per cat PO q.12–24 h
bound drugs such as methotrexate, warfarin,
490
Ch019-S2858.indd 490 11/19/2007 2:28:58 PM
URSODEOXYCHOLIC ACID (URSODIOL)
Diazepam
ing effects of hydrophobic bile acids, which are retained
• 0.05–0.4 mg/kg IV. Eating may begin shortly after administra- in cholestatic disorders. Hydrophobic bile acids can be
tion so have a food supply ready cytotoxic through detergent-like and nondetergent-like
Oxazepam
actions. The mechanisms responsible for this hepato-
• 2 mg per cat PO q.12 h protective effect in humans have not been fully eluci-
dated and are controversial but they are believed to
involve replacement of the more hydrophobic bile acids,
increased bile flow (choleresis) and immunomodulation.
Ursodeoxycholic acid may also inhibit ileal uptake of
DRUGS USED FOR MANAGEMENT OF toxic secondary bile acids formed by bacterial modifica-
HEPATIC DISEASE tion of primary bile acids in the gut lumen. The hepa-
toprotective effect may, however, be less in cats and dogs
URSODEOXYCHOLIC ACID (URSODIOL) than in humans as the major circulating bile acid in dogs
Clinical applications and cats is taurocholate. This is more hydrophilic and
Ursodeoxycholic acid (ursodiol) is a naturally occurring less hepatotoxic than the major circulating bile acids in
bile acid found in the bile of the Chinese black bear. humans.
Black bear bile has been used for many years by practi- Choleresis results from protonation of unconjugated
tioners of Eastern medicine and has been commercially ursodeoxycholic acid when it is secreted into bile, result-
synthesized and available for use as a hepatoprotective ing in the generation of a bicarbonate ion. Protonated
agent in Japan since the 1930s. Since the 1970s ursode- ursodeoxycholic acid is passively absorbed by biliary
oxycholic acid has been used in Western human medi- epithelial cells, resulting in the net secretion of one
cine for dissolution of gallstones. More recently, it has bicarbonate ion, which then serves as an osmotic draw
been used in the management of chronic hepatic diseases for biliary water secretion. Induced choleresis may
in humans such as primary biliary cirrhosis, biliary protect the hepatocytes from potentially toxic sub-
disease secondary to cystic fibrosis, nonalcoholic steato- stances normally secreted into bile such as copper,
hepatitis, idiopathic chronic hepatitis, autoimmune leukotrienes, cholesterol and bilirubin.
hepatitis, primary sclerosing cholangitis and alcoholic The immunomodulatory effects of ursodeoxycholic
hepatitis. However, its therapeutic efficacy in some of acid are believed to involve decreased immunoglobulin
these disorders has not been firmly established. production by B lymphocytes, decreased interleukin-1
In veterinary medicine, ursodeoxycholic acid has been and -2 production by T lymphocytes, decreased expres-
used in the management of dogs with chronic hepatitis sion of hepatocyte cell surface membrane HLA class I
and cats with lymphocytic plasmacytic cholangitis. It is molecules and possibly stimulation of the hepatocyte
believed to be most beneficial in disorders where bile glucocorticoid receptor.
toxicity plays an important role in the ongoing pathol-
ogy. The efficacy of ursodeoxycholic acid in veterinary Formulations and dose rates
patients has not been definitely established, although
anecdotal reports suggest it may have some benefit in Currently, no veterinary preparations are available but a variety of
patients with chronic inflammatory hepatobiliary human products exist, including both tablet (250 mg; e.g. Destolit®,
disease. It may be of some benefit in slowing disease Urso®) and capsule formulations (300 mg; e.g. Ursofalk®, Acti-
progression, especially if used at an early stage of the gall®). The exact choice of product depends upon the size of patient
disease. Some authors recommend ursodeoxycholic acid and ease of dosing with a particular type of preparation.
treatment for all cats with cholangiohepatitis where
DOGS AND CATS
extrahepatic biliary obstruction has been eliminated.
• 10–15 mg/kg q.24 h or divided and given q.12 h
It is recommended that ursodeoxycholic acid be administered for 3–4
Mechanism of action months, after which the patient should be reassessed for improve-
Ursodeoxycholic acid decreases intestinal absorption ment in biochemical markers of hepatocellular pathology. If there has
and suppresses hepatic synthesis and storage of choles- been improvement treatment is continued but if there has been no
terol. This is believed to reduce cholesterol saturation improvement or progression, either treatment should be terminated
of bile, thereby allowing solubilization of cholesterol- or additional therapies such as glucocorticoids or colchicine added.
containing gallstones. It has little effect on calcified
gallstones or on radiolucent bile pigment stones and
therapy is only successful in patients with a functioning Pharmacokinetics
gallbladder. Ursodeoxycholic acid is well absorbed from the small
Ursodeoxycholic acid, a relatively hydrophilic bile intestine in humans, with over 90% of the administered
acid, is also believed to protect the liver from the damag- dose being absorbed. It is extracted from the portal
491
Ch019-S2858.indd 491 11/19/2007 2:28:58 PM
CHAPTER 19 GASTROINTESTINAL DRUGS
circulation and conjugated with either taurine or glycine interfering with the transcellular movement of collagen.
and excreted into bile. Only very small amounts enter The drug increases collagenase activity and may there-
the systemic circulation and minimal amounts are fore promote degradation of existing collagen, although
detected in urine. It undergoes enterohepatic circula- collagen already cross-linked cannot usually be degraded.
tion; at each cycle some of the free and conjugated drug It has anti-inflammatory effects by inhibiting leukocyte
is degraded by gut bacteria, oxidized or reduced to less migration, which may suppress fibrogenesis. It may also
soluble compounds and eliminated in the feces. have a direct hepatoprotective effect by stabilizing hepa-
tocyte membranes. Colchicine is also reported to block
Adverse effects synthesis of serum amyloid A by hepatocytes, thus
● Ursodeoxycholic acid appears to be well tolerated by preventing amyloid formation. The mechanism of its
dogs and cats; vomiting and diarrhea are reported apparent efficacy in gout is poorly understood.
rarely.
● There is some concern in human patients that taurine
depletion may be potentiated by chronic treatment Formulations and dose rates
with ursodeoxycholic acid. This may be important
in cats, who are obligate taurine conjugators. This Various colchicine preparations are available in tablet form, usually in
potential for taurine depletion may be exacerbated either 0.5 mg or 0.6 mg sizes (dependent upon manufacturer). Inject-
in some cats with hepatobiliary disease, who have able formulations may be available, but most experience in veterinary
increased urinary excretion of taurine-conjugated species is with oral dosing. Doses in dogs have been extrapolated
bile acids. Dogs are less likely to become taurine from the human literature. Its use in the cat has not been reported.
depleted by this mechanism as they can shift to Colchicine is marketed in combination with probenecid in some
countries – this combination should be avoided as probenecid can
glycine conjugation.
cause nausea, vomiting and lethargy.
● Ursodeoxycholic acid should not be used in patients
with extrahepatic biliary obstruction, biliary fistulas, DOGS
cholecystitis or pancreatitis. • 0.025–0.03 mg/kg/d
Known drug interactions
Aluminum-containing antacids or colestyramine resin
may bind to ursodeoxycholic acid, thus reducing its Pharmacokinetics
efficacy. Ursodeoxycholic acid dissolves more rapidly in No information is available on the pharmacokinetics of
bile and pancreatic juice; therefore, administration with colchicine in dogs and cats. Data derived from humans
food may improve absorption and is recommended. and laboratory animals indicate that the drug undergoes
first-pass metabolism after absorption from the gut, the
Colchicine metabolites, as well as unchanged drug, being resecreted
Clinical applications into the gut in bile and then reabsorbed. Colchicine is
Colchicine is used in the management of gout in humans, concentrated in leukocytes. Its plasma half-life is about
providing acute relief of symptoms as well as prophy- 20 min; leukocyte half-life is 60 h.
laxis. It has also been used for the treatment of fibrosing Colchicine is deacetylated in the liver as well as being
liver diseases such as primary biliary cirrhosis, alcoholic metabolized in other tissues. Most of the dose is excreted
liver disease, cryptogenic liver fibrosis and liver cirrho- in the feces, with a small amount excreted in urine,
sis. However, two recent meta-analyses have demon- particularly in patients with hepatic disease.
strated limited efficacy of this drug, but more adverse
events. Thus, this drug is likely to fall from favor in Adverse effects
human hepatology. In veterinary medicine it has been ● Because of the limited veterinary experience with
used in the management of amyloidosis and chronic colchicine, little is known about its potential toxicity
hepatic fibrosis. There is anecdotal evidence from a few in dogs and cats.
case studies that colchicine may improve liver function ● In humans, the therapeutic window for colchicine is
and slow the progression of hepatic fibrosis. However, quite narrow, with toxic effects occurring after only
controlled clinical trials are lacking and, given recent small overdoses.
findings in human studies, it should therefore be used ● Nausea, vomiting and diarrhea have been reported
cautiously or avoided altogether. in dogs.
● Bone marrow suppression has occurred in humans
Mechanism of action after prolonged use.
Collagen secretion from lipocytes requires microtubules, ● Myopathy and peripheral neuropathy have been
the assembly of which is inhibited by colchicine, thereby reported rarely in humans.
492
Ch019-S2858.indd 492 11/19/2007 2:28:58 PM
URSODEOXYCHOLIC ACID (URSODIOL)
● Severe local irritation occurs if the drug is inadver- metallothionein, which may bind and sequester copper
tently administered perivascularly. Thrombophlebitis in a nontoxic form. It may also have antifibrotic effects
has also been reported. as it inhibits lysyl oxidase, an enzyme necessary for col-
● Colchicine is contraindicated in patients with serious lagen synthesis, and directly binds to collagen fibrils,
renal, gastrointestinal or cardiac disease and should preventing cross-linking into stable collagen fibers.
be used with caution in patients with less severe However, its efficacy as an antifibrotic agent in humans
disease of these organs. is doubtful and it has not been evaluated in veterinary
● Colchicine is teratogenic in mice and hamsters; there- medicine.
fore it should not be used in pregnant patients unless Penicillamine may have immunomodulatory effects
the benefits outweigh the risks. and has been demonstrated to reduce IgM rheumatoid
● Colchicine may decrease spermatogenesis. factor in humans with rheumatoid arthritis. However,
● Safety for nursing neonates is unknown as it is not its mechanism of action in this disease remains
known whether it is excreted in milk. uncertain.
Known drug interactions Formulations and dose rates
● NSAIDs, especially phenylbutazone, increase the risk
of thrombocytopenia, leukopenia or bone marrow Penicillamine is available as tablets and capsules.
suppression when used concurrently with
colchicine. DOGS AND CATS
● Many antineoplastic and other potentially marrow- Copper-associated hepatopathy
suppressing drugs may cause additive myelosuppres- • 10–15 mg/kg PO q.12 h on an empty stomach. However, if
sion when used concurrently with colchicine. gastrointestinal adverse effects are experienced, these may be
reduced if it is given with food, although absorption may be
● Colchicine may enhance the activity of sympathomi-
reduced. Alternatively, reduce dose and gradually build up to
metic drugs and CNS depressants, although the clini-
full dose
cal significance of this interaction is not known
Cystine urolithiasis
● Colchicine may cause false-positive results for eryth-
• 15 mg/kg PO q.12 h (same comments as above if toxicity
rocytes on urine dipsticks and may elevate serum
experienced)
ALP concentrations.
Lead toxicity
• 110 mg/kg/day divided q.6–8 h. Reduce dose to 33 mg/kg/d if
Penicillamine gastrointestinal adverse effects occur
Penicillamine is a degradation product of penicillin but
has no antimicrobial activity. It was first isolated in
1953 from the urine of a patient with liver disease who Adverse effects
was receiving penicillin. ● Gastrointestinal tract adverse effects are common,
resulting in nausea and vomiting. Smaller doses on
a more frequent basis may alleviate adverse effects.
Clinical applications Alternatively, the drug can be given with food,
Penicillamine is a monothiol chelating agent which is although this will reduce absorption.
used in veterinary medicine in the treatment of copper ● Other adverse effects observed infrequently or
storage hepatopathy (e.g. Bedlington terriers), lead tox- rarely include:
icity and cystine urolithiasis. It has also been used in the – fever
management of rheumatoid arthritis in humans. – lymphadenopathy
– skin hypersensitivity reactions
Mechanism of action – immune-complex glomerulonephropathy.
Penicillamine chelates several metals, including copper, ● Leukopenia, aplastic anemia and agranulocytosis
lead, iron and mercury, forming stable water-soluble have been reported in humans.
complexes that are excreted by the renal route. It also
combines chemically with cystine to form a stable, Known drug interactions
soluble, readily excreted complex. Administration of penicillamine with gold compounds,
Although it usually takes months to years for hepatic cytotoxic or immunosuppressant drugs or phenylbuta-
copper levels to decrease, clinical improvement is often zone may increase the risk of hematological and/or
seen in Bedlington terriers after only a few weeks, renal adverse effects. Zinc (or other cationic minerals)
suggesting that the drug has beneficial effects other may decrease the efficacy of penicillamine when given
than copper depletion. Penicillamine induces hepatic concurrently.
493
Ch019-S2858.indd 493 11/19/2007 2:28:59 PM
CHAPTER 19 GASTROINTESTINAL DRUGS
Zinc with hepatic disease or if toxic substances are present,
conversion to GSH may be reduced. Administration of
Zinc is a nutritional metal agent that is used to reduce exogenous SAMe increases hepatic and red blood cell
copper toxicity in breeds with copper-associated hepa- GSH concentrations, whilst this compound also inhibits
topathies, e.g. Bedlington terrier. It is also reported to apoptosis secondary to the presence of alcohol or bile
have antifibrotic functions. The effect of copper toxicosis acids in hepatocytes. Other effects include anti-
relates to the ability of zinc to inhibit the absorption of depressant activity, possibly due to increased serotonin
copper in the gastrointestinal tract. For liver disease, zinc turnover, and increased dopamine or noradrenaline
supplementation is often provided as part of a purpose- (norepinephrine) release.
formulated prescription diet. However, oral and inject- Oral bioavailability is reported to be 1% and the
able forms are also available and usually include either amount absorbed can be reduced further in the presence
zinc acetate or zinc sulfate. Zinc acetate is the prepara- of food. Once absorbed, SAMe enters the portal circula-
tion most commonly used for hepatic disorders. tion and is metabolized in the liver.
Large doses of zinc can cause gastrointestinal signs,
including vomiting, whilst hemolysis can occur after Clinical applications
administration of large doses or if serum concentrations SAMe is most frequently used as adjunctive therapy for
exceed 1000 µg/dL. Penicillamine and ursodeoxycholic a variety of hepatic disorders (canine chronic hepatitis,
acid can decrease zinc absorption, whilst zinc salts can hepatic lipidosis, cholangiohepatitis, etc.). It may also
reduce the absorption of tetracycline and fluoroquino- be beneficial in the treatment of certain hepatotoxic
lones (e.g. enrofloxacin). It is recommended to stagger disorders, most notably paracetamol (acetaminophen).
dosing by at least 2 h.
Formulations and dose rates
Formulations and dose rates
No pharmaceutical preparations exist; SAMe is considered to be a
DOGS nutritional supplement. Therefore, potency, purity, safety and efficacy
Copper-associated hepatopathy may vary across the various preparations. Specific animal products
• 5–10 mg/kg (of elemental zinc) PO q.12 h. Start at the higher exist, e.g. Denosyl®, Zentonil® and Hepatosyl®.
end of the dose range for the first 3 months, then reduce dose
to 50 mg PO q.12 h for maintenance. Separate the dose from DOGS AND CATS
feeding by 1–2 h. Monitor plasma zinc concentrations every • Calculate daily dose based upon 17–20 mg/kg PO q.24 h (or
2–3 months and aim for plasma zinc concentrations of divided twice daily), rounded to the closest tablet size. The
200–400 µg/dL product should be administered on an empty stomach, ≥1 h
before feeding
Hepatic fibrosis
• Or, dose according to the following regimen: 5.5 kg, 90 mg PO
• 10 mg/kg (of elemental zinc) q.24 h PO, aiming for plasma zinc
q.24 h; 5.5–11 kg, 180 mg PO q.24 h; 11–16 kg, 225 mg PO
concentrations between 200–300 µg/dL
q.24 h; 16–29.5 kg, 450 mg PO q.24 h; 29.5–41 kg, 675 mg
PO q.24 h; 41 kg+, 900 mg PO q.24 h
S-adenosyl methionine (SAMe)
Adverse effects
S-adenosyl methionine (SAMe) is an endogenous mole-
SAMe appears relatively safe for use in small animals
cule which is synthesized, from methionine, by many
and adverse effects are minimal. In humans, oral dosing
cells in the body. However, the enzyme SAMe synthetase
may cause anorexia, nausea, vomiting, diarrhea, flatu-
is found in the liver and is the rate-limiting step for
lence, constipation, dry mouth, insomnia, headache,
SAMe synthesis in the face of hepatic compromise.
sweating and dizziness.
SAMe is an essential factor in three major biochemical
pathways (most important in the liver), namely trans-
Known drug interactions
methylation, transsulfuration and aminopropylation.
Concurrent use of pethidine (meperidine), monoamine
SAMe functions as a donor of methyl groups and is thus
oxidase inhibitors (e.g. selegiline), serotonin reuptake
essential for the activation or elimination of many
inhibitors (e.g. fluoxetine) and other antidepressants
substances. For transsulfuration, SAMe generates
(e.g. amitryptiline, clomipramine) could cause additive
sulfur-containing compounds, which are important for
serotonergic effects.
conjugation reactions and for synthesis of glutathione
(GSH). The latter is also essential for numerous meta-
bolic processes and detoxification reactions; conversion
Silymarin
of SAMe to GSH requires folate, cyanocobalamin and Milk thistle, Silybum marianum, is a flower used for
pyroxidine. Ample SAMe is usually synthesized but, thousands of years for medical purposes. Three bio-
494
Ch019-S2858.indd 494 11/19/2007 2:28:59 PM
URSODEOXYCHOLIC ACID (URSODIOL)
chemicals of interest have been isolated from the milk ● Finally, silymarin may increase the clearance of drugs
thistle: silychristine, silydianin and silybin. The mixture which undergo hepatic glucuronidation, e.g.
of these three substances is called ‘silymarin’. Silymarin paracetamol (acetaminophen), diazepam and
has been traditionally used in the treatment of liver morphine.
disease but while it has recently been advocated for use
in pets, all scientific information available concerns Lactulose
human use. The biological mechanism of action is yet
Lactulose is a synthetic derivative of lactose, consisting
unknown but several theories exist. Silymarin may:
of one molecule of galactose and one molecule of fruc-
● control hepatic cell membrane permeability and
tose. This disaccharide cannot be digested by enzymes
thus prevent toxin penetration
of the mammalian digestive tract, allowing the colonic
● inhibit the cytotoxic, inflammatory and apoptotic
microflora to convert it to low molecular weight acids
effects of tumor necrosis factor
(lactic, formic and acetic acid). These acids both increase
● inhibit lipid peroxidase and β-glucoronidase and
osmotic pressure (thus drawing water into the intestine
act as a free radical scavenger and antioxidant
and having a laxative effect) and cause an acidifying
● reduce hepatic collagen formation
effect. By acidifying the colonic contents, ammonia
● increase hepatic glutathione content.
(NH3) is trapped as ammonium (NH4+) and, in this
form, cannot be absorbed across the intestinal wall. Less
Clinical applications
than 3% of this drug is absorbed, the drug is not metab-
Controlled studies demonstrating the efficacy of silyma-
olized and is excreted unchanged in the urine within
rin are lacking and formulations are not standardized.
24 h.
However, it is used commonly in the treatment of human
and companion animal hepatic disorders. It is most
Clinical applications
commonly utilized in the treatment of chronic hepa-
The main use of lactulose is to reduce blood ammonia
topathies, although it may also be suitable for acute
concentrations in the treatment of hepatic encephalopa-
hepatic disease and as a hepatoprotective agent against
thy. It can also be used as an osmotic laxative for the
a variety of hepatotoxic substances (such as Amanita
treatment of constipation.
phalloides).
Formulations and dose rates Formulations and dose rates
No pharmaceutical preparations exist and, as with SAMe, silymarin is The commercially available preparations are viscous sweet liquids
considered to be a nutritional supplement. Therefore, potency, purity, and have an adjusted pH of 3–7.
safety and efficacy may vary across the various preparations. A variety
of preparations exist, including tablets and capsules in various DOGS
strengths, e.g. from 150 mg to 1000 mg. • 5–30 mL PO q.6–8 h initially, then adjust the dose to achieve
2–3 soft stools per day
DOGS AND CATS • For encephalopathic coma, first empty and clean the lower
• 20–50 mg/kg PO q.24 h bowel with repeated warm water enemas, then use 18–20 mL/
kg of a solution containing 3 parts lactulose and 7 parts warm
water, as a retention enema. Replace every 4–8 h
Adverse effects
● There are no reported absolute contraindications for CATS
silymarin and this drug is well tolerated by the oral • For hepatic encephalopathy: 0.25–5mL PO q.8–12 h. Again,
route. modify the dose to achieve soft stools
● Overdoses rarely cause significant morbidity. The • For encephalopathic coma, first empty and clean the lower
bowel with repeated warm water enemas, then use 18–20 mL/
main signs seen in these situations are
kg of a solution containing 3 parts lactulose and 7 parts warm
gastrointestinal. water, as a retention enema. Replace every 4–8 h
• For constipation, 0.5 mL/kg q.8–12h PO
Known drug interactions
● Silymarin may inhibit the cytochrome P450 enzyme
2C9, such that drugs with narrow therapeutic ranges Adverse effects
should be used with caution, e.g. warfarin, amitrip- ● The main adverse effects are gastrointestinal, e.g.
tyline and verapamil. flatulence, gastric distension and cramping.
● Silymarin may also inhibit cytochrome P3A4, but ● The main side effect of overdose is diarrhea.
this interaction has not yet been found to be ● Use cautiously in patients with pre-existing fluid
significant. and electrolyte imbalances.
495
Ch019-S2858.indd 495 11/19/2007 2:28:59 PM
CHAPTER 19 GASTROINTESTINAL DRUGS
● Cats do not like the taste of lactulose and it can be
difficult to administer this drug to some patients.
Formulations and dose rates
There are no veterinary-approved formulations, but a variety of human
Known drug interactions preparations are available (e.g. Ipeca®, Ipecacuanha tincture®,
● Do not use lactulose and other laxatives Ipecavom®, Ipetitrin®, etc.) containing various concentrations, e.g.
concurrently. 1.5%, 1.75% and 2%.
● In theory, the use of some antibacterials (e.g. neomy-
DOGS
cin) could eliminate the bacteria that convert lactu-
• 1.0–2.5 mL/kg PO (to a maximum of 15 mL) as a single dose.
lose to low molecular weight acids that exert an Repeat after 20 min if no response. If the stomach is empty,
osmotic effect. However, this has not appeared give 5 mL/kg of water immediately afterwards. If vomiting does
to be a clinical concern since synergy has been not occur after the second dose, subsequently perform gastric
reported when lactulose and antibiotics are used lavage to retrieve the ipecac
concurrently.
● Nonabsorbable oral antacids may reduce colonic CATS
acidification and might reduce the efficacy of • 1.0–3.3 mL/kg PO as an initial dose. It may be prudent to dilute
lactulose. the dose 50:50 with water, to minimize the adverse effect of
the taste. Repeat with a second dose 20 min after the first if
vomiting does not occur; subsequently perform gastric lavage to
retrieve the ipecac
EMETIC AGENTS
In some circumstances, most notably after recent inges- Pharmacokinetics
tion of toxic compounds, drugs are required to induce There are few data available on the pharmacokinetics
vomiting. A number of household products have been of ipecac syrup. Apparently, there is great interindivid-
used for the purpose, most notably strong salt (sodium ual variability in the proportion absorbed amongst
chloride) solutions, hydrogen peroxide and washing patients.
soda crystals. In addition, the sedative drug xylazine
may be effective for this purpose in cats. However, the Adverse effects
most commonly used pharmaceutical agents are syrup ● Emetics are contraindicated in patients that are
of ipecacuanha (ipecac) and apomorphine. hypoxic, dyspneic, unable to swallow, hypovolemic
Emetic agents rarely eliminate more than 80% of the or comatose.
ingested material and more commonly only 40–60%. ● Emetics should not be given to animals which have
Therefore, it is advisable to use other symptomatic ingested strong acids or alkalis because the contents
therapies in conjunction with emetic agents. of the vomitus may cause further damage to esopha-
geal, pharyngeal or oral tissues.
Ipecac syrup ● Given the risk of aspiration, emetics should not be
given after ingestion of petrolatum or related com-
Clinical applications pounds because the risk of subsequent aspiration
Ipecac syrup is derived from the roots and rhizomes of outweighs the potential toxicity.
certain plants; it contains two active alkaloid agents: ● The syrup is clear, with a mild odor. It has an unpleas-
emetine and cephaeline. The main indication of this ant taste and, as a consequence, may be difficult to
agent is to induce vomiting, after the ingestion of toxic administer successfully to cats.
compounds or after a drugs overdose. ● Although side effects are uncommon, occasional side
effects include salivation, lacrimation, protracted
Mechanism of action vomiting, diarrhea and lethargy.
The major alkaloids of ipecac (emetine and cephaeline) ● Overdosage of ipecac has been known to lead to
are thought to be the pharmacologically active agents cardiotoxicity (e.g. arrhythmias, hypotension and
and have both local and central activity. Locally, they fatal myocarditis).
produce an irritant effect on the gastric mucosa, whilst
centrally they stimulate the chemoreceptor trigger zone. Known drug interactions
The medullary regions must be responsive for vomiting ● Use of emetics in the face of strychnine intoxication,
to be elicited. When vomiting occurs, contents from or with other CNS stimulants, may precipitate
both the stomach and small intestine are evacuated. seizures.
Vomiting usually occurs with 10–30 min of administra- ● Activated charcoal may adsorb ipecac syrup and, as
tion in both dogs and cats. a result, these drugs should not be administered con-
496
Ch019-S2858.indd 496 11/19/2007 2:28:59 PM
FURTHER READING
currently. Instead, ipecac syrup should be given first result, parenteral (or subconjunctival) administration is
and activated charcoal only administered once vom- preferred. Emesis usually occurs rapidly after intrave-
iting has occurred. nous administration, whilst therefore may be a delay of
● The efficacy of ipecac may be decreased by dairy 5 min after intramuscular injection. Although conjunc-
products and carbonated beverages. tival administration is effective, response is less predict-
able and injected routes are preferred.
Apomorphine
Adverse effects
Clinical applications
● Emetics are contraindicated in patients that are
Apomorphine is used as an emetic agent in dogs, where
hypoxic, dyspneic, unable to swallow, hypovolemic
it is considered to be the drug of choice for this purpose.
or comatose.
Its use is controversial in cats.
● Emetics should not be given to animals which have
ingested strong acids or alkalis because the contents
Mechanism of action
of the vomitus may cause further damage to esopha-
Apomorphine stimulates dopamine receptors in the che-
geal, pharyngeal or oral tissues.
moreceptor trigger zone and thereby induces vomiting.
● Given the risk of aspiration, emetics should not be
Although it may have both stimulatory and inhibitory
given after ingestion of petrolatum or related com-
effects within the CNS, stimulatory effects predominate.
pounds because the risk of subsequent aspiration
However, depression of medullary centers may lead to
outweighs the potential toxicity.
respiratory depression.
● The principal adverse effect is protracted vomiting.
Excitement, restlessness, CNS excitement/depression
Formulations and dose rates and cardiorespiratory depression may occur if an
No veterinary licensed products are available, but there are a number overdose is administered. The CNS adverse effects
of human preparations. can be reversed by naloxone, although this drug
cannot usually block the vomiting.
DOGS ● Apomorphine should not be used in cases of oral
• 0.03–4 mg/kg IV or 0.04–0.08 mg/kg IM or SC, as a single opiate or other CNS depressant (e.g. barbiturate)
dose toxicity.
● Apomorphine is contraindicated in patients hyper-
CATS sensitive to morphine.
• 0.04 mg/kg IV, or 0.08 mg/kg IM or SC as a single dose.
● The use of this drug is controversial in cats and many
However, use in this species is controversial and many do not
clinicians believe that xylazine and ipecac syrup are
recommend it
• If vomiting does not occur after administration, it is inadvisable both more effective.
to administer repeated doses as they are unlikely to be effective
and signs of toxicity may occur Known drug interactions
● Drugs with antidopaminergic effects may antagonize
the effect of apomorphine, e.g. phenothiazines.
Pharmacokinetics ● Additive CNS, cardiac and respiratory adverse
Apomorphine is slowly absorbed after oral administra- effects may develop if apomorphine is administered
tion and efficacy is unpredictable by this route. As a concurrently with opiates.
FURTHER READING
Hall JA, Washabau RJ 2000 Gastric prokinetic agents. In: Bonagura J Plumb DA 2005 Plumb’s veterinary drug handbook, 5th edn. Blackwell
(ed.) Current veterinary therapy XIII. WB Saunders, Philadelphia, PA, Publishing, Ames, IA
pp 614-617 Washabau RJ, Elie MS 1995 Antemetic therapy. In: Bonagura J (ed.)
Leveille-Webster C 2000 Ursodeoxycholic acid therapy. In: Bonagura J Current veterinary therapy XIII. WB Saunders, Philadelphia, PA,
(ed.) Current veterinary therapy XIII. WB Saunders, Philadelphia, PA, pp 679-684
pp 691-693
497
Ch019-S2858.indd 497 11/19/2007 2:28:59 PM
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5807)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (842)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Human Anatomy and Physiology Syllabus. Allan RevisedDocument7 pagesHuman Anatomy and Physiology Syllabus. Allan RevisedAllan IgbuhayNo ratings yet
- FCM Lec 18 Family Life CycleDocument4 pagesFCM Lec 18 Family Life Cycleabstabs100% (2)
- Vampires, Werewolves, and ZombiesDocument2 pagesVampires, Werewolves, and Zombieshru217No ratings yet
- Neutron 2.0 NEET Minor Test - 02 Without Answer KeyDocument22 pagesNeutron 2.0 NEET Minor Test - 02 Without Answer KeyshamamatulkubraNo ratings yet
- Treatment of Antibiotics in Dogs and Cats During PregnancyDocument9 pagesTreatment of Antibiotics in Dogs and Cats During PregnancyNoe Moreno GumetaNo ratings yet
- الكيمياء الحياتية الجزء الأولDocument396 pagesالكيمياء الحياتية الجزء الأولمحمد الجبوريNo ratings yet
- Lecture-1, Introductio To MicrobiologyDocument35 pagesLecture-1, Introductio To MicrobiologyWaleed 1100% (1)
- Plants Used To Treat Various Mental Illnesses in Ethiopia A Systematic ReviewDocument26 pagesPlants Used To Treat Various Mental Illnesses in Ethiopia A Systematic ReviewSIYUM ABAYINEHNo ratings yet
- Biocatalysis and Agricultural BiotechnologyDocument13 pagesBiocatalysis and Agricultural BiotechnologyDANIELA GELVEZNo ratings yet
- Severe MalnutritionDocument92 pagesSevere MalnutritionLa Ode RinaldiNo ratings yet
- SPM Biology Form 4 NotesDocument3 pagesSPM Biology Form 4 NotesSmiley555No ratings yet
- Biol 309 Test Question Bank Cell CycleDocument6 pagesBiol 309 Test Question Bank Cell CycleottermanerttwbNo ratings yet
- Download textbook Ganongs Review Of Medical Physiology Kim E Barrett ebook all chapter pdfDocument53 pagesDownload textbook Ganongs Review Of Medical Physiology Kim E Barrett ebook all chapter pdfmichael.penland389100% (8)
- Lung CancerDocument33 pagesLung CancerPirma Ivan Ricky MNo ratings yet
- Darwin Digital Library of Evolution Alphabetical Listing of WorksDocument211 pagesDarwin Digital Library of Evolution Alphabetical Listing of WorksEduardo Martín PérezNo ratings yet
- Get To The Root of ItDocument4 pagesGet To The Root of Itscmsliteracy0% (1)
- Matrix ThinkingDocument102 pagesMatrix Thinkingskiiidse100% (12)
- Lesson Plan Science Demo Junior HighDocument4 pagesLesson Plan Science Demo Junior HighDotecho Jzo Ey100% (1)
- Topic # 6 Plant NutritionDocument43 pagesTopic # 6 Plant Nutritionraimaadnan646No ratings yet
- Eur Heart J Suppl 2007 Guidelines On Diabetes, Pre Diabetes, and Cardiovascular DiseasesDocument72 pagesEur Heart J Suppl 2007 Guidelines On Diabetes, Pre Diabetes, and Cardiovascular DiseasesJonida HaxhiNo ratings yet
- Effect of Mixed Starters On Proteolysis and Formation of Biogenic Amines in Dry Fermented Mutton SausagesDocument15 pagesEffect of Mixed Starters On Proteolysis and Formation of Biogenic Amines in Dry Fermented Mutton SausagesRoberto DegenhardtNo ratings yet
- Types of PathogensDocument56 pagesTypes of PathogensMelody DacanayNo ratings yet
- Staphylococcus Aureus: Presented byDocument29 pagesStaphylococcus Aureus: Presented byAyesha ArshadNo ratings yet
- LIFS 1902 - General Biology II: Video 4 - Human DevelopmentDocument20 pagesLIFS 1902 - General Biology II: Video 4 - Human DevelopmentGary TsangNo ratings yet
- Nanorobots The Heart SurgeonDocument7 pagesNanorobots The Heart SurgeonPoonguzhali MadhavanNo ratings yet
- I Can't Believe It!Document1 pageI Can't Believe It!Jonathan PrietoNo ratings yet
- MCAT Sample Questions Template 1Document42 pagesMCAT Sample Questions Template 1gendut_novri0% (1)
- April Green PrintDocument8 pagesApril Green PrintNikki ReiffNo ratings yet
- Acute Effects of Different Temperature in The Blood Parameters of Common Carp (Cyprinus Carpio)Document4 pagesAcute Effects of Different Temperature in The Blood Parameters of Common Carp (Cyprinus Carpio)BlagojaNo ratings yet
- NCM 109 Reviewer Module 1Document6 pagesNCM 109 Reviewer Module 1tamsmadjad18No ratings yet