You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5806)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (842)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Pigging ProcedureDocument11 pagesPigging ProcedureEndika Alfan100% (9)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Service Oriented Architecture - Course Notes PDFDocument93 pagesService Oriented Architecture - Course Notes PDFRoberto Luna OsorioNo ratings yet
- Milgram's Obedience To Authority: Its Origins, Controversies, and ReplicationsDocument32 pagesMilgram's Obedience To Authority: Its Origins, Controversies, and ReplicationsnabilahbilqisNo ratings yet
- Pathania 2019Document20 pagesPathania 2019nabilahbilqisNo ratings yet
- Katigbak 2018Document9 pagesKatigbak 2018nabilahbilqisNo ratings yet
- Oup Accepted Manuscript 2021Document19 pagesOup Accepted Manuscript 2021nabilahbilqisNo ratings yet
- Adhrence 1Document9 pagesAdhrence 1nabilahbilqisNo ratings yet
- Tingkat Pengetahuan HerawatiDocument7 pagesTingkat Pengetahuan HerawatinabilahbilqisNo ratings yet
- Psychology of Sport and Exercise: Changiz Mohiyeddini, Regina Pauli, Stephanie BauerDocument9 pagesPsychology of Sport and Exercise: Changiz Mohiyeddini, Regina Pauli, Stephanie BauernabilahbilqisNo ratings yet
- Avor Tri 2019Document6 pagesAvor Tri 2019nabilahbilqisNo ratings yet
- Intention and AttitudeDocument9 pagesIntention and AttitudenabilahbilqisNo ratings yet
- A Security Risk Perception Model For The Adoption of MobileDocument25 pagesA Security Risk Perception Model For The Adoption of MobilenabilahbilqisNo ratings yet
- ComplianceDocument11 pagesCompliancenabilahbilqisNo ratings yet
- Journal Pre-Proofs: Food Quality and PreferenceDocument33 pagesJournal Pre-Proofs: Food Quality and PreferencenabilahbilqisNo ratings yet
- Papies 2017Document19 pagesPapies 2017nabilahbilqisNo ratings yet
- AwarnesDocument6 pagesAwarnesnabilahbilqisNo ratings yet
- Attitude, KnowledgeDocument7 pagesAttitude, KnowledgenabilahbilqisNo ratings yet
- Behaviour & Information Technology: Click For UpdatesDocument16 pagesBehaviour & Information Technology: Click For UpdatesnabilahbilqisNo ratings yet
- Jurnal PromkesDocument14 pagesJurnal PromkesnabilahbilqisNo ratings yet
- HIV Retesting of HIV-Negative Pregnant Women in The Context of Prevention of Mother-to-Child Transmission of HIV in Primary Health Centers in Rural Zambia: What Did We Learn?Document6 pagesHIV Retesting of HIV-Negative Pregnant Women in The Context of Prevention of Mother-to-Child Transmission of HIV in Primary Health Centers in Rural Zambia: What Did We Learn?nabilahbilqisNo ratings yet
- Antenatal Care and Uptake of HIV Testing Among Pregnant Women in Sub-Saharan Africa: A Cross-Sectional StudyDocument10 pagesAntenatal Care and Uptake of HIV Testing Among Pregnant Women in Sub-Saharan Africa: A Cross-Sectional StudynabilahbilqisNo ratings yet
- Jurnal PentingDocument11 pagesJurnal PentingnabilahbilqisNo ratings yet
- Exploring The Association Between Multimorbidity and Cognitive Impairment in Older Adults Living in The Community: A Review of The LiteratureDocument11 pagesExploring The Association Between Multimorbidity and Cognitive Impairment in Older Adults Living in The Community: A Review of The LiteraturenabilahbilqisNo ratings yet
- 2018 Article 708Document7 pages2018 Article 708nabilahbilqisNo ratings yet
- Economic Systematic ReviewDocument12 pagesEconomic Systematic ReviewnabilahbilqisNo ratings yet
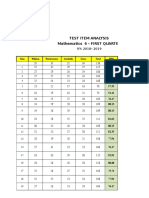
- Test Item Analysis Mathematics 6 - FIRST QUARTER: Item Wisdom Perseverance Gratitude Grace Total MPSDocument6 pagesTest Item Analysis Mathematics 6 - FIRST QUARTER: Item Wisdom Perseverance Gratitude Grace Total MPSQUISA O. LAONo ratings yet
- Activity Sheets Q1 - SVADocument5 pagesActivity Sheets Q1 - SVAAlma ReynaldoNo ratings yet
- Conjunction and Exposition Text-2Document19 pagesConjunction and Exposition Text-2keyshalaokkiNo ratings yet
- JNTUK SGPA Calculator - JNTU Kakinada R20, R19, R16 SGPA Calculator OnlineDocument3 pagesJNTUK SGPA Calculator - JNTU Kakinada R20, R19, R16 SGPA Calculator OnlineRamesh Dasari0% (1)
- HW1Document5 pagesHW1John SpartanNo ratings yet
- Development of Design Air For Tunnel Lining Design Using Analytical MethodDocument93 pagesDevelopment of Design Air For Tunnel Lining Design Using Analytical MethodChin Thau WuiNo ratings yet
- The Progress Report of The Mumbai-Ahmedabad High Speed Railway ProjectDocument4 pagesThe Progress Report of The Mumbai-Ahmedabad High Speed Railway ProjectJorge MariaNo ratings yet
- Citing SourcesDocument37 pagesCiting Sourcesasquared29No ratings yet
- Noli and El FiliDocument2 pagesNoli and El FiliGeramei Vallarta TejadaNo ratings yet
- Momentum - Action High Intensity 2022Document24 pagesMomentum - Action High Intensity 2022GabrielNo ratings yet
- Media MetricsDocument28 pagesMedia MetricsPulkit ChhabraNo ratings yet
- Mahindra & Mahindra LogisticsDocument3 pagesMahindra & Mahindra LogisticspeednaskNo ratings yet
- Formula and Functions in MS ExcelDocument9 pagesFormula and Functions in MS ExcelBhavana SangamNo ratings yet
- HW 2Document12 pagesHW 2Munish RanaNo ratings yet
- LymphomaDocument20 pagesLymphomaChairul Adilla Ardy100% (1)
- (R) Nelson JB (2017) - Mindful Eating - The Art of Presence While You EatDocument4 pages(R) Nelson JB (2017) - Mindful Eating - The Art of Presence While You EatAnonymous CuPAgQQNo ratings yet
- Projects & Operations: IN: NE Power Systm ImprvmDocument5 pagesProjects & Operations: IN: NE Power Systm ImprvmGaurang PatelNo ratings yet
- FCo Research Report Debit Card and Bitcoin in MenaDocument10 pagesFCo Research Report Debit Card and Bitcoin in MenaJhimy JeanNo ratings yet
- Grammar Translation MethodDocument22 pagesGrammar Translation MethodCeyinNo ratings yet
- The Top Level Diagram Is A Use Case Diagram That Shows The Actors andDocument5 pagesThe Top Level Diagram Is A Use Case Diagram That Shows The Actors andsin2pNo ratings yet
- The Dedicated - A Biography of NiveditaDocument384 pagesThe Dedicated - A Biography of NiveditaEstudante da Vedanta100% (2)
- Unit 5 and 6Document2 pagesUnit 5 and 6Leo GonellNo ratings yet
- Coastal Suite For Tuba SoloDocument7 pagesCoastal Suite For Tuba SoloSusanna Payne-Passmore100% (1)
- Advanced Concepts of GD&TDocument3 pagesAdvanced Concepts of GD&TPalani Trainer33% (3)
- Classroom EtiquetteDocument1 pageClassroom EtiquetteJerrold MangaoNo ratings yet
- Civil Engineering MCQ'sDocument1 pageCivil Engineering MCQ'sNISHIKANTA MONDALNo ratings yet
- Cse205 Computer-Architecture-And-Organization TH 2.00 Ac26Document2 pagesCse205 Computer-Architecture-And-Organization TH 2.00 Ac26Ravi ThejaNo ratings yet
- Finalizing The Accounting ProcessDocument2 pagesFinalizing The Accounting ProcessMilagro Del ValleNo ratings yet