You might also like
- Case 1 History & PEDocument3 pagesCase 1 History & PEcbac1990No ratings yet
- Intern Obs Hx-1Document6 pagesIntern Obs Hx-1essasam12No ratings yet
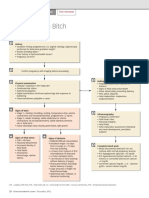
- Dystocia in The BitchDocument2 pagesDystocia in The BitchGissele ParaisoNo ratings yet
- O&G History TakingDocument5 pagesO&G History TakingAishwarya SivakumarNo ratings yet
- History ObgynDocument37 pagesHistory ObgynRana WaelNo ratings yet
- ObstetricsDocument40 pagesObstetricsعمر احمد شاكرNo ratings yet
- OB History and PEDocument3 pagesOB History and PE2D FRAN, CRISTINENo ratings yet
- Early Pregnancy ComplicationsDocument38 pagesEarly Pregnancy ComplicationsAzim Syahmi Abd RazakNo ratings yet
- ANC OB and GYN HISTORY Taking SampleDocument43 pagesANC OB and GYN HISTORY Taking SampleGebremichael Reta100% (3)
- Obstetric HistoryDocument16 pagesObstetric HistoryJeffrey XieNo ratings yet
- Obstetric History & Examination SheetDocument8 pagesObstetric History & Examination SheetVaibhav BhatiaNo ratings yet
- NCM 219 ReviewDocument32 pagesNCM 219 ReviewKeanu Win CatipayNo ratings yet
- Bleeding in Early PregnancyDocument32 pagesBleeding in Early PregnancyElangrizkyrNo ratings yet
- Open Questioning: Ob GynDocument1 pageOpen Questioning: Ob GynConcepcion R. AquinoNo ratings yet
- History Obstetrics 3Document15 pagesHistory Obstetrics 3VICTOR OLUWAKEYENo ratings yet
- LP KEHAMILAN NORMAL Zaii - Id.enDocument5 pagesLP KEHAMILAN NORMAL Zaii - Id.enMuhammad ZainuddinNo ratings yet
- Emed - OB Part 1Document6 pagesEmed - OB Part 1Princess Cate MercadoNo ratings yet
- Physical Examination, Investigation & Differential Diagnosis in Obstetrics/GynecologyDocument20 pagesPhysical Examination, Investigation & Differential Diagnosis in Obstetrics/GynecologyIsma Alif IsmaNo ratings yet
- Obstetrics by Tikrit StudentsDocument57 pagesObstetrics by Tikrit StudentsEngi KazangyNo ratings yet
- Jordie-Prenatal Care StudygramDocument7 pagesJordie-Prenatal Care StudygramNoreen Hannah GabrielNo ratings yet
- Obs-Gynae CP Final (2nd Batch)Document89 pagesObs-Gynae CP Final (2nd Batch)Dipesh ShresthaNo ratings yet
- Obstetrics HistoryDocument3 pagesObstetrics HistorymakepaNo ratings yet
- Ante Natal Care: by Naveen Sharma J.N - Medical College Belgaum, IndiaDocument37 pagesAnte Natal Care: by Naveen Sharma J.N - Medical College Belgaum, IndiaNaveen SharmaNo ratings yet
- OB JC Case of Hydatidiform MoleDocument37 pagesOB JC Case of Hydatidiform MoleBlykeBantugan100% (2)
- LaborDocument2 pagesLaborAngelyn FlorenososNo ratings yet
- Obsgyn: Mode of DeliveryDocument8 pagesObsgyn: Mode of DeliverySiti MardhiahNo ratings yet
- Breast Cancer History TakingDocument2 pagesBreast Cancer History Takingbloo tomartoNo ratings yet
- 2018 01 Early Pregnancy Loss LightDocument41 pages2018 01 Early Pregnancy Loss LightMishal FatimaNo ratings yet
- HA Lecture Week 5 ROSDocument6 pagesHA Lecture Week 5 ROSLore Anne Mhae SantosNo ratings yet
- Pregnancy HealthyDocument17 pagesPregnancy Healthyasmaa.khaledmhammed789No ratings yet
- SafariViewService - 16 Feb 2019 12.09Document1 pageSafariViewService - 16 Feb 2019 12.09Ngakan Ketut DarmawanNo ratings yet
- GYN History OSCEDocument7 pagesGYN History OSCEOccamsRazorNo ratings yet
- Previa Vs AbruptioDocument1 pagePrevia Vs AbruptioJamaica QuetuaNo ratings yet
- Pre-Partum Intrapartum: Additional Entry in Nursing HistoryDocument1 pagePre-Partum Intrapartum: Additional Entry in Nursing HistoryAngela Mae DiestroNo ratings yet
- Multiple Pregnancy HatimDocument22 pagesMultiple Pregnancy HatimHatim AbdellateifNo ratings yet
- Ca Mamma (DK)Document10 pagesCa Mamma (DK)Jody HernantoNo ratings yet
- 1000113 EUS教學 (7) 重點式急診婦產科超音波之應用Document114 pages1000113 EUS教學 (7) 重點式急診婦產科超音波之應用juice119100% (4)
- LP KEHAMILAN NORMAL Haidir (2) .Id - enDocument7 pagesLP KEHAMILAN NORMAL Haidir (2) .Id - enMuhammad ZainuddinNo ratings yet
- Antenatal Case SheetDocument4 pagesAntenatal Case SheetRichard SnellNo ratings yet
- History and PE22333Document7 pagesHistory and PE22333lugodvalerieNo ratings yet
- Maternity Nursing NotesDocument7 pagesMaternity Nursing NotesazitaaaaaNo ratings yet
- Obstetric and Clinical Medicine - Gynaecological History and ExaminationDocument7 pagesObstetric and Clinical Medicine - Gynaecological History and ExaminationShahin Kazemzadeh100% (2)
- Obstetrics: Topic OutlineDocument5 pagesObstetrics: Topic OutlineRea Dominique CabanillaNo ratings yet
- Gynae History TakingDocument23 pagesGynae History TakingAlmira PutriNo ratings yet
- The REPRODUCTION-PROCESSDocument30 pagesThe REPRODUCTION-PROCESSEJ GolimlimNo ratings yet
- Surgery CaseDocument43 pagesSurgery CaseAvni GuptaNo ratings yet
- Wa0001.Document152 pagesWa0001.YESHASWI PRASADNo ratings yet
- Obstetrics: Topic OutlineDocument22 pagesObstetrics: Topic OutlineRea Dominique CabanillaNo ratings yet
- Obsterics History C-I (Edited)Document14 pagesObsterics History C-I (Edited)Tamam JamalNo ratings yet
- MCHNDocument6 pagesMCHNJohn KenNo ratings yet
- Kerpean Obsgyn (21-08-17) PDFDocument25 pagesKerpean Obsgyn (21-08-17) PDFKhadijah Aufadina100% (2)
- 0 - Women Key Words ListDocument7 pages0 - Women Key Words ListamyngaileeNo ratings yet
- Cmca Lec ReviewerDocument32 pagesCmca Lec Reviewercuteathena11No ratings yet
- Early Pregnancy Complications: by Harvir Singh Supervised by DR Ranjit and DR SyafiqahDocument33 pagesEarly Pregnancy Complications: by Harvir Singh Supervised by DR Ranjit and DR SyafiqahShre RanjithamNo ratings yet
- Tutorial 3 APH, PP, VP, AbruptioDocument55 pagesTutorial 3 APH, PP, VP, AbruptioBahirahNo ratings yet
- Obstetrics Gynaecology ReportDocument2 pagesObstetrics Gynaecology ReportBEYOND ZFSNo ratings yet
- Obs Moses KazevuDocument285 pagesObs Moses KazevuChilufya KalasaNo ratings yet
- Gynecology History TakingDocument1 pageGynecology History TakingSulabh ShresthaNo ratings yet
- Fibrotic-Cavernous TBDocument12 pagesFibrotic-Cavernous TBRandev WannakuwatteNo ratings yet
- Comprehensive Nursing Care in Transplant Unit-1-1Document47 pagesComprehensive Nursing Care in Transplant Unit-1-1Rajani Singh BaghelNo ratings yet
- Palmones Parasitology Lab TransesDocument19 pagesPalmones Parasitology Lab TransesJISOO KimNo ratings yet
- Adriano, Ma. Niña Inocencio 2123035954Document2 pagesAdriano, Ma. Niña Inocencio 2123035954Nina NinzNo ratings yet
- Vaccination BOON or BANEDocument5 pagesVaccination BOON or BANERushil BhandariNo ratings yet
- Información: Estado Tipo de Participantes Rangos de EdadDocument11 pagesInformación: Estado Tipo de Participantes Rangos de EdadAlondraNo ratings yet
- Manejo Radiológico de Las Masas de Partes Blandas de La Mano y MuñecaDocument28 pagesManejo Radiológico de Las Masas de Partes Blandas de La Mano y MuñecaJenniffer FNo ratings yet
- Operating Room Orientation ManualDocument14 pagesOperating Room Orientation ManualHannah MercadoNo ratings yet
- Randomized Controlled Trial of Internet Cognitive Behavioural Treatment For Social Phobia With and Without Motivational Enhancement StrategiesDocument8 pagesRandomized Controlled Trial of Internet Cognitive Behavioural Treatment For Social Phobia With and Without Motivational Enhancement StrategiesCytha Nilam ChairaniNo ratings yet
- Leptospirosis - Ferri's Clinical AdvisorDocument2 pagesLeptospirosis - Ferri's Clinical AdvisorAndika GhifariNo ratings yet
- COURSE OUTLINE For STUDENT 1Document5 pagesCOURSE OUTLINE For STUDENT 1Nur Fatima SanaaniNo ratings yet
- Guidelines For New Drug Registration, CurazaoDocument8 pagesGuidelines For New Drug Registration, CurazaoNumas SalazarNo ratings yet
- RPM ACOG Practice BulletinDocument13 pagesRPM ACOG Practice BulletinGabriela Cordova GoicocheaNo ratings yet
- 1 s2.0 S1550830716301665 MainDocument7 pages1 s2.0 S1550830716301665 MainAwadAyoubNo ratings yet
- Lit 2. Sepsis-3 Abdul Hakeem Al Hashim, MD, FRCPCDocument76 pagesLit 2. Sepsis-3 Abdul Hakeem Al Hashim, MD, FRCPCKomang_JananuragaNo ratings yet
- SMS Result and Data 2021Document161 pagesSMS Result and Data 2021ChinaNo ratings yet
- J CLP 2010 05 003Document15 pagesJ CLP 2010 05 003Rofifa EvaNo ratings yet
- Chapter 16 and 17 ND QuizDocument3 pagesChapter 16 and 17 ND Quizrobertvaliente471No ratings yet
- Resep Obat Jadi - LINEDocument33 pagesResep Obat Jadi - LINEGorgaNo ratings yet
- Anesthetic Considerations For Robotassisted Gynecologic and Urology Surgery 2155 6148.1000345Document7 pagesAnesthetic Considerations For Robotassisted Gynecologic and Urology Surgery 2155 6148.1000345drsubramanian100% (1)
- Giles B1Document37 pagesGiles B1imgayNo ratings yet
- Local Anesthetics AgentsDocument56 pagesLocal Anesthetics AgentsIyad Abou-Rabii100% (1)
- Microbial EcologyDocument49 pagesMicrobial EcologyWahab KhaniNo ratings yet
- Acupressure PDFDocument15 pagesAcupressure PDFpinoybsn2692% (12)
- Case Study of Acute GastritisDocument12 pagesCase Study of Acute GastritisANCHAL SHARMANo ratings yet
- Full Download Book Fishmans Pulmonary Diseases and Disorders PDFDocument41 pagesFull Download Book Fishmans Pulmonary Diseases and Disorders PDFjeffrey.hemmings786100% (14)
- Nandini SpouseDocument10 pagesNandini SpouseGanesh GaniNo ratings yet
- Mechanical Ventilation and Noninvasive VentilationDocument6 pagesMechanical Ventilation and Noninvasive Ventilationuul ulfaNo ratings yet
- 14860Document3 pages14860Sahil DhamijaNo ratings yet
- The Background of The Plastic Surgeon by Dr. Jay Calvert.Document2 pagesThe Background of The Plastic Surgeon by Dr. Jay Calvert.Bentzen94IpsenNo ratings yet