You might also like
- Urinery IncontinsetenceDocument1 pageUrinery IncontinsetenceLanaAmerieNo ratings yet
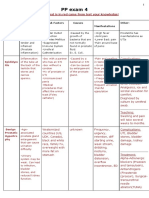
- PP Exam 4: Everything That Is in Red Came From Test Your Knowledge!Document15 pagesPP Exam 4: Everything That Is in Red Came From Test Your Knowledge!netanya DoanNo ratings yet
- Elderly Urinary Tract Disorders FixDocument36 pagesElderly Urinary Tract Disorders FixRyan Adi PutraNo ratings yet
- Care of Clients With Problems of The Male Reproductive SystemDocument18 pagesCare of Clients With Problems of The Male Reproductive SystemwakswafuNo ratings yet
- Benign Prostatic HyperplasiaDocument4 pagesBenign Prostatic Hyperplasiaエド パジャロンNo ratings yet
- UTI - Concept MapDocument1 pageUTI - Concept MapZam Pamate50% (2)
- Urological Emergencies: Julian ManderDocument43 pagesUrological Emergencies: Julian ManderDara MirandaNo ratings yet
- Symptomatology of GUT DisordersDocument75 pagesSymptomatology of GUT DisordersMaraJoRNNo ratings yet
- Wa0038.Document5 pagesWa0038.sham gowliNo ratings yet
- UTI - Concept MapDocument1 pageUTI - Concept MapZam Pamate100% (4)
- Male Reproductive ProblemsDocument17 pagesMale Reproductive Problemsluna nguyenNo ratings yet
- Pelvic Anatomy Slides FINALDocument36 pagesPelvic Anatomy Slides FINALRajashekharNo ratings yet
- Genitourinary System Clinical GuidelinesDocument41 pagesGenitourinary System Clinical Guidelinessnowlover boyNo ratings yet
- Null - PDF 2Document30 pagesNull - PDF 2مهند حسام محمد سعيد عبدNo ratings yet
- Benign Prostatic HyperplasiaDocument5 pagesBenign Prostatic Hyperplasiatabangin_hilario100% (1)
- MS 2Document9 pagesMS 2Vincent AmitNo ratings yet
- Surgery - Female Urology and Incontinence (Tutorial)Document6 pagesSurgery - Female Urology and Incontinence (Tutorial)halesNo ratings yet
- Acute and Chronic Urinary RetentionDocument3 pagesAcute and Chronic Urinary RetentionParyNo ratings yet
- BLadder Outlet ObstructionDocument28 pagesBLadder Outlet ObstructionCodillia Cheong100% (1)
- Benign Prostatic HyperplasiaDocument4 pagesBenign Prostatic HyperplasiaAdelle Fortunato100% (2)
- Inkontinensia UrinDocument24 pagesInkontinensia UrinloyaNo ratings yet
- Infeksi Saluran KemihDocument27 pagesInfeksi Saluran KemihEvan PermanaNo ratings yet
- Benign Prostatic Hyperplasia. NCM 109Document16 pagesBenign Prostatic Hyperplasia. NCM 109Niña Jean Tormis AldabaNo ratings yet
- General Anatomu UrologyDocument60 pagesGeneral Anatomu UrologyAllan ManiNo ratings yet
- Types and Causes of Urinary IncontinenceDocument13 pagesTypes and Causes of Urinary IncontinenceAshadeep KaurNo ratings yet
- Benign Prostate HyperthropyDocument3 pagesBenign Prostate Hyperthropyzmae23No ratings yet
- 313 - Disorders of Renal and Urinary SystemsDocument8 pages313 - Disorders of Renal and Urinary SystemsChrissy Mendoza100% (2)
- Alpha Blockers & 5ARIs Relieve BPH SymptomsDocument73 pagesAlpha Blockers & 5ARIs Relieve BPH SymptomsSisay FentaNo ratings yet
- Guide to Urinary & Renal DeviationsDocument60 pagesGuide to Urinary & Renal DeviationsmolyebeedNo ratings yet
- UrinaryRetention_508(1)Document8 pagesUrinaryRetention_508(1)earldioborrinagaNo ratings yet
- Canine Prostatic Diseases: Reproduction and Periparturient CareDocument13 pagesCanine Prostatic Diseases: Reproduction and Periparturient CareSatria Adi MarhendraNo ratings yet
- History Taking in Urology-UndergraduateDocument12 pagesHistory Taking in Urology-Undergraduateasmaaburas100% (1)
- Acute Urinary ObstructionDocument34 pagesAcute Urinary ObstructionHafizur RashidNo ratings yet
- Urinary Tract Infection: DR Humna Najeeb KhanDocument28 pagesUrinary Tract Infection: DR Humna Najeeb KhanSaliha AkramNo ratings yet
- Urinary Tract Infection (UTI)Document6 pagesUrinary Tract Infection (UTI)Anonymous iG0DCOfNo ratings yet
- Urological Emergencies: DR Ahmed BekeerDocument31 pagesUrological Emergencies: DR Ahmed BekeerAh BakaNo ratings yet
- Acute Urinary Retention: Anith T VDocument17 pagesAcute Urinary Retention: Anith T VAnn Merlin JobinNo ratings yet
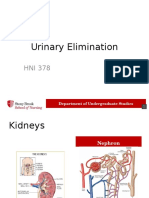
- Urinary Elimination 2014 VoiceDocument32 pagesUrinary Elimination 2014 VoiceMohammad Usman QureshiNo ratings yet
- Urinary Incontinence - Treatment, Causes, Types, and SymptomsDocument13 pagesUrinary Incontinence - Treatment, Causes, Types, and SymptomsJimmy GillNo ratings yet
- Managing Benign Prostatic Hyperplasia (BPHDocument9 pagesManaging Benign Prostatic Hyperplasia (BPHhussain Altaher0% (1)
- BPH Treatment and Surgical OptionsDocument25 pagesBPH Treatment and Surgical OptionsShreevidya GurunageshNo ratings yet
- Kuliah UtiDocument20 pagesKuliah UtiERNINo ratings yet
- UTI Guide: Symptoms, Diagnosis and TreatmentDocument39 pagesUTI Guide: Symptoms, Diagnosis and TreatmentHafid Adi NugrohoNo ratings yet
- Emergencies in UrologyDocument112 pagesEmergencies in UrologySusiyadiNo ratings yet
- Acute Urological EmergenciesDocument58 pagesAcute Urological EmergenciesDr. NasrumminallahNo ratings yet
- Uti, Incontinence, Neurogenic BladderDocument3 pagesUti, Incontinence, Neurogenic Bladdermaan20No ratings yet
- Emergencies in UrologyDocument112 pagesEmergencies in UrologyafiwahyuNo ratings yet
- Urologic TDocument7 pagesUrologic TMariaNo ratings yet
- Urinary Tract Infection in Children: DR Nada Qawasmi Alquds Faculty of MedicineDocument25 pagesUrinary Tract Infection in Children: DR Nada Qawasmi Alquds Faculty of Medicineولاء إبراهيمNo ratings yet
- UTIDocument27 pagesUTIDianeNo ratings yet
- Benign Prostatic HyperplasiaDocument3 pagesBenign Prostatic HyperplasiaBebeness MoNo ratings yet
- Benigna Hiperplasia ProstatDocument23 pagesBenigna Hiperplasia ProstatShanti ArianiNo ratings yet
- BPHDocument20 pagesBPHHerly KakaNo ratings yet
- IncontinenceDocument9 pagesIncontinenceHanaNo ratings yet
- Benign Prostatic Hyperplasia (BPH) Hyperplasia (BPH) : BY. Abdi MohamedDocument112 pagesBenign Prostatic Hyperplasia (BPH) Hyperplasia (BPH) : BY. Abdi MohamedTILAHUNNo ratings yet
- Benign Prostatic HyperplasiaDocument28 pagesBenign Prostatic HyperplasiaFedrick MasatuNo ratings yet
- Catheter troubleshooting guide NBT 2019_0Document6 pagesCatheter troubleshooting guide NBT 2019_0Ali QureshiNo ratings yet
- BPH 180828154943Document42 pagesBPH 180828154943Amandeep SinghNo ratings yet
- UTI Disorder PDFDocument23 pagesUTI Disorder PDFMonarahayuNo ratings yet
- Interferential Therapy Versus Pelvic Floor Exercise For The Management of Stress Urinary Incontinence in WomenDocument7 pagesInterferential Therapy Versus Pelvic Floor Exercise For The Management of Stress Urinary Incontinence in WomenjothiNo ratings yet
- Effect of Bladder Training on Urine Expenditure Acceleration in Post-Caesarean WomenDocument9 pagesEffect of Bladder Training on Urine Expenditure Acceleration in Post-Caesarean WomenIndah MadaNo ratings yet
- Interpretation of The Lab Result (Except Urinalysis) : (Adiba)Document4 pagesInterpretation of The Lab Result (Except Urinalysis) : (Adiba)EkahBaikCantikNo ratings yet
- Best Laparoscopic Urologist and Kidney Specialist - DR Shyam VarmaDocument3 pagesBest Laparoscopic Urologist and Kidney Specialist - DR Shyam Varmashyam varmaNo ratings yet
- Pregnancy Induced Urinary Tract Changes Urinary Tract InfectionsDocument5 pagesPregnancy Induced Urinary Tract Changes Urinary Tract InfectionsDilausan B MolukNo ratings yet
- Male Reproductive SystemDocument30 pagesMale Reproductive SystemRaisashimi M.S.100% (1)
- Acute Kidney InjuryDocument17 pagesAcute Kidney InjuryPrecious C. MamaradloNo ratings yet
- Acute Kidney Injury: Causes, Stages, and ManagementDocument62 pagesAcute Kidney Injury: Causes, Stages, and ManagementApidha KartinasariNo ratings yet
- 1153 3589 1 PBDocument7 pages1153 3589 1 PBalda aldaNo ratings yet
- Ultra Thin Uretero-Renoscope 4.5 / 6.5 FRDocument4 pagesUltra Thin Uretero-Renoscope 4.5 / 6.5 FRIndra JayaNo ratings yet
- A True Complete Diphalliahas Proven To Be A More Complex Case of Caudal Duplication SyndromeDocument4 pagesA True Complete Diphalliahas Proven To Be A More Complex Case of Caudal Duplication SyndromeLuminita PopaNo ratings yet
- Urinalysis CaseDocument3 pagesUrinalysis CaseAzriel Al MushoriNo ratings yet
- Cases Journal: Acquired Nonobstructive Urinary Bladder Diverticulum: A CaseDocument3 pagesCases Journal: Acquired Nonobstructive Urinary Bladder Diverticulum: A CaseIrma Suriani DarwisNo ratings yet
- Sexual Survey Results From Over 100 WomenDocument129 pagesSexual Survey Results From Over 100 Womengurudeb91% (11)
- Histology of Urinary SystemDocument36 pagesHistology of Urinary Systemdiraf100% (2)
- NMIBC Guide: Diagnosis and Management of Non-Muscle Invasive Bladder CancerDocument20 pagesNMIBC Guide: Diagnosis and Management of Non-Muscle Invasive Bladder CancerMade Moniaga PrawiraNo ratings yet
- Health Education PlanDocument3 pagesHealth Education PlanCamille VegaNo ratings yet
- Natural Penis Enlargement Exercises 1 PDFDocument12 pagesNatural Penis Enlargement Exercises 1 PDFCatherine Mic100% (5)
- Atlas of Laparoscopic and Robotic Single Site Surgery: Jihad H. Kaouk Robert J. Stein Georges-Pascal Haber EditorsDocument315 pagesAtlas of Laparoscopic and Robotic Single Site Surgery: Jihad H. Kaouk Robert J. Stein Georges-Pascal Haber EditorsMarc PagniezNo ratings yet
- Female & Male Sexual AnatomyDocument37 pagesFemale & Male Sexual AnatomynissashiblyNo ratings yet
- Oral Sex: What's The Real Risk For HIV?Document2 pagesOral Sex: What's The Real Risk For HIV?Mohamed KhattabNo ratings yet
- Neurogenic Lower Urinary Tract Dysfunction: Guidelines OnDocument52 pagesNeurogenic Lower Urinary Tract Dysfunction: Guidelines OnPatrascu CristiNo ratings yet
- Handbook of Pediatric Urology PDFDocument547 pagesHandbook of Pediatric Urology PDFJany Bueno MontielNo ratings yet
- New Post Grad ProgramDocument8 pagesNew Post Grad ProgramPradeep KumarNo ratings yet
- Case Report BPH Qorry WelendriDocument39 pagesCase Report BPH Qorry WelendriDindaNo ratings yet
- Susunan AcaraDocument2 pagesSusunan Acaraniko4eyesNo ratings yet
- Uti in PregnancyDocument42 pagesUti in Pregnancydeepak122No ratings yet
- WNS Technical TestDocument15 pagesWNS Technical TestRohit Kumar MahatoNo ratings yet
- Cghs ListDocument49 pagesCghs Listnew_soulNo ratings yet
- Presentation Prof Mtioui CSDocument15 pagesPresentation Prof Mtioui CSNaoufalMtiouiChkairiNo ratings yet