You might also like
- BPH PDFDocument7 pagesBPH PDFJody FelizioNo ratings yet
- Medscape BPHDocument41 pagesMedscape BPHEugenia ShepanyNo ratings yet
- Clinical Manifestations and Diagnostic Evaluation of Benign Prostatic Hyperplasia - UpToDateDocument13 pagesClinical Manifestations and Diagnostic Evaluation of Benign Prostatic Hyperplasia - UpToDateJhonnyJesùsHonorioEstelaNo ratings yet
- Clinical Manifestations and Diagnostic Evaluation of Benign Prostatic Hyperplasia - UpToDateDocument17 pagesClinical Manifestations and Diagnostic Evaluation of Benign Prostatic Hyperplasia - UpToDateMario Lopez CastellanosNo ratings yet
- BPH - TextDocument7 pagesBPH - TextSomesh GuptaNo ratings yet
- CBL 2 REPORT - Fuzna Dahlia M - I1J020010Document9 pagesCBL 2 REPORT - Fuzna Dahlia M - I1J020010Fuzna DahliaNo ratings yet
- AUA MedStudent BPHDocument13 pagesAUA MedStudent BPHCirugía Residentes AjuscoNo ratings yet
- BPH - TextDocument7 pagesBPH - TextSomesh GuptaNo ratings yet
- Benign Prostatic HyperplasiaDocument15 pagesBenign Prostatic HyperplasiaAilene GuzmanNo ratings yet
- Benign Prostate HyperplasiaDocument49 pagesBenign Prostate HyperplasiaRohani TaminNo ratings yet
- Benign Prostatic Hyperplasia and Male Lower Urinary Symptoms: A Guide For Family PhysiciansDocument4 pagesBenign Prostatic Hyperplasia and Male Lower Urinary Symptoms: A Guide For Family PhysiciansAndi Nurul FadhilahNo ratings yet
- Pharmacotherapy of - Benign Prostatic HyperplasiaDocument4 pagesPharmacotherapy of - Benign Prostatic HyperplasiaBaarid HamidiNo ratings yet
- RENAL (PBL4) - Mohamad Arbian Karim - FMUI20Document4 pagesRENAL (PBL4) - Mohamad Arbian Karim - FMUI20Mohamad Arbian KarimNo ratings yet
- Adult Nursing 2 Teaching PlanDocument5 pagesAdult Nursing 2 Teaching PlanJerilee SoCute WattsNo ratings yet
- Prostate Hyperplasia, Benign: Author: Raymond J Leveillee, MD, FRCS (Glasg), Professor of Clinical Urology, RadiologyDocument36 pagesProstate Hyperplasia, Benign: Author: Raymond J Leveillee, MD, FRCS (Glasg), Professor of Clinical Urology, RadiologyGerald FilomenoNo ratings yet
- Benign Prostatic Hyperplasia and Male Lower Urinary Symptoms: A Guide For Family PhysiciansDocument4 pagesBenign Prostatic Hyperplasia and Male Lower Urinary Symptoms: A Guide For Family Physiciansmuhammad hasan fuadyNo ratings yet
- Benign Prostatic HyperplasiaDocument10 pagesBenign Prostatic HyperplasiaRoshwill KingNo ratings yet
- Pa Tho PhysiologyDocument9 pagesPa Tho PhysiologyMabz Posadas BisnarNo ratings yet
- SL No Content NODocument12 pagesSL No Content NOPdianghunNo ratings yet
- Seminar On: Benign Prostatic HyperplasiaDocument19 pagesSeminar On: Benign Prostatic HyperplasiaHoney PrasadNo ratings yet
- Benign Prostatic Hyperplasia and Male Lower Urinary Symptoms: A Guide For Family PhysiciansDocument4 pagesBenign Prostatic Hyperplasia and Male Lower Urinary Symptoms: A Guide For Family PhysiciansAndi Tiara S. AdamNo ratings yet
- Benign Prostatic HyperplasiaDocument34 pagesBenign Prostatic Hyperplasiaanwar jabariNo ratings yet
- 1 BPHDocument27 pages1 BPHVikrant GholapNo ratings yet
- Intro (BPH)Document2 pagesIntro (BPH)ametrine2010No ratings yet
- Powell 2020Document7 pagesPowell 2020kanaNo ratings yet
- BPHDocument57 pagesBPHDiannetotz MoralesNo ratings yet
- Managing Urinary Tract Problem: FOCUS On The FollowingDocument11 pagesManaging Urinary Tract Problem: FOCUS On The FollowingLovely DaroleNo ratings yet
- Benign Prostatic Hyperplasia-Gabrilia Geaby RoringDocument19 pagesBenign Prostatic Hyperplasia-Gabrilia Geaby RoringDedylihawaNo ratings yet
- WONG Activity#9Document4 pagesWONG Activity#9Lecery Sophia WongNo ratings yet
- Case Presentation Benign Prostatic HyperplasiaDocument19 pagesCase Presentation Benign Prostatic HyperplasiaWidya Amalia SwastikaNo ratings yet
- BPH and Its Scope in HomeopathyDocument3 pagesBPH and Its Scope in HomeopathyEditor IJTSRDNo ratings yet
- Benign Prostatic Hyperplasia (BPH) : University of California, San FranciscoDocument1 pageBenign Prostatic Hyperplasia (BPH) : University of California, San FranciscoMaich ScdNo ratings yet
- Arc BPH Chapter1Document8 pagesArc BPH Chapter1Civa NuhaNo ratings yet
- The Prostate GlandDocument8 pagesThe Prostate GlandRACHMAH KURNIASARINo ratings yet
- Benign Prostatic HyperplasiaDocument22 pagesBenign Prostatic HyperplasiaQueen SofiaNo ratings yet
- HSC2 - Case Presentation - Final PaperDocument42 pagesHSC2 - Case Presentation - Final PaperLance RafaelNo ratings yet
- BPH DefinitionDocument5 pagesBPH DefinitionMadhu Sudhan PandeyaNo ratings yet
- Ju 0000000000002183Document12 pagesJu 0000000000002183AlizaPinkyNo ratings yet
- Benign Prostatic HyperplasiaDocument9 pagesBenign Prostatic Hyperplasiaanju rachel joseNo ratings yet
- Benign Prostatic HyperplasiaDocument6 pagesBenign Prostatic HyperplasiaAnonymous 9OkFvNzdsNo ratings yet
- BPHDocument20 pagesBPHHerly KakaNo ratings yet
- Disease of Prostate Tutorial-Dec-2014Document49 pagesDisease of Prostate Tutorial-Dec-2014marina_shawkyNo ratings yet
- Benign Prostatic Hyperplasia: A Case Analysis OnDocument70 pagesBenign Prostatic Hyperplasia: A Case Analysis OnAngelica RelanaNo ratings yet
- Clinical Manifestations and Diagnostic Evaluation of Benign Prostatic Hyperplasia - UpToDateDocument11 pagesClinical Manifestations and Diagnostic Evaluation of Benign Prostatic Hyperplasia - UpToDateFeer VillarrealNo ratings yet
- BPH (Benign Prostatic Hyperplasia)Document11 pagesBPH (Benign Prostatic Hyperplasia)AviZhafiraNo ratings yet
- Benign Prostatic Hypertrophy - ClinicalKeyDocument24 pagesBenign Prostatic Hypertrophy - ClinicalKeyJhosept Perez AlvaNo ratings yet
- Medical Therapy For Benign Prostatic Hyperplasia: A ReviewDocument11 pagesMedical Therapy For Benign Prostatic Hyperplasia: A ReviewEfson Sustera IrawanNo ratings yet
- Benign Prostatic Hyperplasia (BPH) and Bladder Outlet Obstruction (BOO)Document73 pagesBenign Prostatic Hyperplasia (BPH) and Bladder Outlet Obstruction (BOO)Swe Zin NaingNo ratings yet
- Revised BPHDocument2 pagesRevised BPHCyril Jane Caanyagan AcutNo ratings yet
- Journal ReadingDocument7 pagesJournal ReadingcharissabibilNo ratings yet
- BPH by SamuelDocument33 pagesBPH by SamuelIan Smith AkampuriraNo ratings yet
- Benign Prostatic Hypertrophy: Pathophysiology and EtiologyDocument4 pagesBenign Prostatic Hypertrophy: Pathophysiology and EtiologyErnestomalamionNo ratings yet
- Clinical Case of Evidence Based MedicineDocument6 pagesClinical Case of Evidence Based MedicinempNo ratings yet
- Practice Essentials: Signs and SymptomsDocument4 pagesPractice Essentials: Signs and Symptomsyeni62No ratings yet
- Benign Prostatic HyperplasiaDocument5 pagesBenign Prostatic HyperplasiaLag Lag AlbercaNo ratings yet
- BPH InternetDocument72 pagesBPH InternetDesty ArianiNo ratings yet
- Benign Prostatic Hyperplasia PDFDocument496 pagesBenign Prostatic Hyperplasia PDFnurul_nufafinaNo ratings yet
- Hematuria, (Blood in Urine) A Simple Guide to The Condition, Related Diseases And Use in Diagnosis of DiseasesFrom EverandHematuria, (Blood in Urine) A Simple Guide to The Condition, Related Diseases And Use in Diagnosis of DiseasesRating: 5 out of 5 stars5/5 (2)
- Phase 4 Medicine Intended Learning Outcomes (Ilos)Document19 pagesPhase 4 Medicine Intended Learning Outcomes (Ilos)AmaNo ratings yet
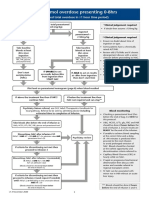
- Paracetamol Overdose Presenting 0-8hrs: (Ingested Total Overdose inDocument1 pageParacetamol Overdose Presenting 0-8hrs: (Ingested Total Overdose inAmaNo ratings yet
- Eportfolio User Guide For Trainees: March 2009Document30 pagesEportfolio User Guide For Trainees: March 2009AmaNo ratings yet
- Spirit of ScotlandDocument1 pageSpirit of ScotlandAmaNo ratings yet
- ChoeDocument116 pagesChoeJihad AnadNo ratings yet
- Saw Palmetto and Liver ToxicityDocument3 pagesSaw Palmetto and Liver ToxicityPeter SerranoNo ratings yet
- Incontinentia Urine Kuliah Uniba 6-11-12. ADocument53 pagesIncontinentia Urine Kuliah Uniba 6-11-12. AHumaira AzmiNo ratings yet
- Dihydrotestosterone (DHT) - DHT Stimulates Cell Growth in The Tissue That Lines The Prostate GlandDocument7 pagesDihydrotestosterone (DHT) - DHT Stimulates Cell Growth in The Tissue That Lines The Prostate GlandPeter Kenneth LampitocNo ratings yet
- The Relationship Between Erectile Dysfunction and Lower Urinary Tract Symptoms and The Role of Phosphodiesterase Type 5 InhibitorsDocument11 pagesThe Relationship Between Erectile Dysfunction and Lower Urinary Tract Symptoms and The Role of Phosphodiesterase Type 5 InhibitorsVignesh KymalNo ratings yet
- Original Research Paper AyurvedaDocument3 pagesOriginal Research Paper Ayurvedamade dharmaNo ratings yet
- Mobilisasi Dini Dan Penurunan Skala Nyeri Pada Pasien Post Operasi Turp Benign Prostate HyperplasiaDocument8 pagesMobilisasi Dini Dan Penurunan Skala Nyeri Pada Pasien Post Operasi Turp Benign Prostate HyperplasiaM Fadlillah Al FitrahNo ratings yet
- Jurnal LUTS PDFDocument8 pagesJurnal LUTS PDFmitaNo ratings yet
- 30140-Article Text-56524-1-10-20201030Document11 pages30140-Article Text-56524-1-10-20201030melendezjmanuelNo ratings yet
- Clinical Presentation and Diagnosis of Urinary IncontinenceDocument18 pagesClinical Presentation and Diagnosis of Urinary IncontinenceMartín SánchezNo ratings yet
- Guide For Good Prostate HealthDocument9 pagesGuide For Good Prostate HealthAlceir FerreiraNo ratings yet
- Patient Care Plan SPVDocument55 pagesPatient Care Plan SPVCarlton Anthony George IINo ratings yet
- Dumbre - 2012 - Effect of Chandraprabha Vati in Experimental Prostatic Hyperplasia and Inflammation in RatsDocument3 pagesDumbre - 2012 - Effect of Chandraprabha Vati in Experimental Prostatic Hyperplasia and Inflammation in RatsHendra Wana Nur'aminNo ratings yet
- 06 Understanding Herbal MedicinesDocument101 pages06 Understanding Herbal MedicinesSelfreliantman98% (45)
- History Taking in Urology-UndergraduateDocument12 pagesHistory Taking in Urology-Undergraduateasmaaburas100% (1)
- Benign Prostatic HyperplasiaDocument55 pagesBenign Prostatic HyperplasiaJeffrey DyerNo ratings yet
- Urologic Complications of DiabetesDocument9 pagesUrologic Complications of DiabetesMaria Marcella RusliNo ratings yet
- Catheter Care GuidelinesDocument35 pagesCatheter Care GuidelinesClaire BeetNo ratings yet
- 10.male Reproductive System 2 BlocksDocument220 pages10.male Reproductive System 2 BlocksANA CAROLINE ANDRADE DE MELONo ratings yet
- EAU Guidelines On Male Sexual Dysfunction 2019Document96 pagesEAU Guidelines On Male Sexual Dysfunction 2019Muti IlmarifaNo ratings yet
- Open Prostatectomy For Huge Prostates Our Experience in A Developing Country 2329 9088.1000132Document3 pagesOpen Prostatectomy For Huge Prostates Our Experience in A Developing Country 2329 9088.1000132Ahmed Ben BellaNo ratings yet
- Even Urologists Get Kidney Stones 1st PDFDocument205 pagesEven Urologists Get Kidney Stones 1st PDFIosub Lica-ClaudiuNo ratings yet
- Bagian Kedua Tes Bahasa Inggris (NOMOR 121 S.D. 180) Structure and Written ExpressionDocument4 pagesBagian Kedua Tes Bahasa Inggris (NOMOR 121 S.D. 180) Structure and Written ExpressionamirahalimaNo ratings yet
- Herbal Medicine IntroDocument14 pagesHerbal Medicine IntrocryarNo ratings yet
- URO Final 2023Document31 pagesURO Final 2023دشيرين إبراهيمNo ratings yet
- Comprehensive Review On Ayurvedic UrologyDocument12 pagesComprehensive Review On Ayurvedic UrologyInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- CH19 Patho D&R AgamDocument21 pagesCH19 Patho D&R Agam062No ratings yet
- Radhwa International SchoolDocument45 pagesRadhwa International Schoolsafamanz001 safaNo ratings yet
- Niyats Proposal DraftDocument35 pagesNiyats Proposal DraftrobelNo ratings yet
- 2018 - Alshammari The Benign Prostatic Hyperplasia and It's AetiologiesDocument6 pages2018 - Alshammari The Benign Prostatic Hyperplasia and It's AetiologieskanaNo ratings yet