You might also like
- Psychiatric EmergencyDocument7 pagesPsychiatric EmergencySiti TiaraNo ratings yet
- QTC Flow Diagram With Medications Final Dec 17 A3 With LogosDocument1 pageQTC Flow Diagram With Medications Final Dec 17 A3 With LogosMelissa MurilloNo ratings yet
- ASRA - Summary Flash CardsDocument2 pagesASRA - Summary Flash CardsParvathy R NairNo ratings yet
- Orthopedic Inpatient Protocols: A Guide to Orthopedic Inpatient RoundingFrom EverandOrthopedic Inpatient Protocols: A Guide to Orthopedic Inpatient RoundingNo ratings yet
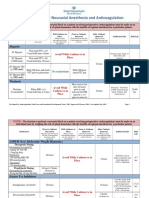
- (ASRA) Guidelines Neuraxial and AnticoagulationDocument6 pages(ASRA) Guidelines Neuraxial and Anticoagulationfraditayyunus82% (11)
- Induced HPDocument4 pagesInduced HPmaddythedocNo ratings yet
- McCarty, Koopman - Arthritis and Allied Conditions A Textbook of Rheumatology 12th Ed PDFDocument1,529 pagesMcCarty, Koopman - Arthritis and Allied Conditions A Textbook of Rheumatology 12th Ed PDFKirilNo ratings yet
- Section 504 Examples of Disabilities and AccommodationsDocument17 pagesSection 504 Examples of Disabilities and Accommodationsapi-434662376No ratings yet
- PediatricDocument16 pagesPediatricSwagnikNo ratings yet
- Society For Obesity and Bariatric Anaesthesia: OS-MRS Calculator Tools - Farmacologiaclinica.infoDocument1 pageSociety For Obesity and Bariatric Anaesthesia: OS-MRS Calculator Tools - Farmacologiaclinica.infoHizami Norddin100% (2)
- Price List Mai New Juni 2021Document14 pagesPrice List Mai New Juni 2021Hardhi SuryatnoNo ratings yet
- Emergency Executive Order No. 2020-04!03!24-20Document7 pagesEmergency Executive Order No. 2020-04!03!24-20Emilee Speck56% (9)
- Pharmacological Tools: Doses, Routes, and Uses of Common DrugDocument1 pagePharmacological Tools: Doses, Routes, and Uses of Common DrugApuntesdemedicinaa blogNo ratings yet
- QA in Bacteriology and Immunology WHODocument185 pagesQA in Bacteriology and Immunology WHOjuanescribd100% (1)
- Health Care (Hospital) Industry: Pristine HospitalsDocument27 pagesHealth Care (Hospital) Industry: Pristine Hospitalssamknight2009No ratings yet
- Ecart MedsDocument5 pagesEcart Medsしゃいな ふかみNo ratings yet
- Thrombolytic Therapy For Stroke: Reconstitution and Administration Rtpa ActivaseDocument24 pagesThrombolytic Therapy For Stroke: Reconstitution and Administration Rtpa ActivaseRosalinda S CambriNo ratings yet
- AcetaminophenDocument1 pageAcetaminophensalwakh266No ratings yet
- Acetaminophen (APAP) ToxicityDocument12 pagesAcetaminophen (APAP) ToxicityJessa MaeNo ratings yet
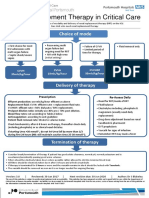
- Renal Replacement Therapy in Critical Care: Choice of ModeDocument15 pagesRenal Replacement Therapy in Critical Care: Choice of ModePeter AgabaNo ratings yet
- Paracetamol Overdose ManagementDocument11 pagesParacetamol Overdose ManagementKarthika SampathkumarNo ratings yet
- Initial Full-Dose Heparin For Adult: 1-Venous Thromboembolism (DVT/PE), TreatmentDocument3 pagesInitial Full-Dose Heparin For Adult: 1-Venous Thromboembolism (DVT/PE), TreatmentLamNo ratings yet
- Management of Paracetamol ToxicityDocument28 pagesManagement of Paracetamol ToxicityA94-WONG JING TONGNo ratings yet
- Reviewer Special Blood Collection and PointDocument8 pagesReviewer Special Blood Collection and PointRicanie CadornaNo ratings yet
- When Do I Give Fluids?Document14 pagesWhen Do I Give Fluids?Tom BiusoNo ratings yet
- Acute PancreatitisDocument11 pagesAcute PancreatitisJessa MaeNo ratings yet
- Trilostane Dosing MonitoringDocument1 pageTrilostane Dosing Monitoringnessimmounir100% (1)
- Document PDFDocument4 pagesDocument PDFDebasis SahooNo ratings yet
- TransfusionDocument3 pagesTransfusionjulissand10No ratings yet
- Enoxaparin - Safe Prescribing - Check It Out 1Document3 pagesEnoxaparin - Safe Prescribing - Check It Out 1Zaid DewachiNo ratings yet
- TDM Practical Guide Part1Document7 pagesTDM Practical Guide Part1Ahmedshaker21100% (1)
- Intravenous Infusion Orders For Common Medications in The ED and ICU - Bunbury HospitalDocument39 pagesIntravenous Infusion Orders For Common Medications in The ED and ICU - Bunbury Hospital9wb646hq7mNo ratings yet
- Anticoagulation Guidelines For Neuraxial Procedures: Anticoagulants, InjectableDocument4 pagesAnticoagulation Guidelines For Neuraxial Procedures: Anticoagulants, InjectablepaulaNo ratings yet
- Renal Replacement Therapy in Critical Care: Choice of ModeDocument15 pagesRenal Replacement Therapy in Critical Care: Choice of ModeJelena Obrenovic StankovicNo ratings yet
- Pediatric Oral Anticoagulation Prescription and Administration RecordDocument2 pagesPediatric Oral Anticoagulation Prescription and Administration RecordMohammed IbrahimNo ratings yet
- Periarestne AritmijeDocument10 pagesPeriarestne AritmijeMustafa ŠabićNo ratings yet
- Anticoagulation Protocol For PostDocument8 pagesAnticoagulation Protocol For PostMohammed IbrahimNo ratings yet
- MedicationsDocument63 pagesMedicationssaraNo ratings yet
- 9 Ketamine Drug StudyDocument7 pages9 Ketamine Drug Studyshadow gonzalezNo ratings yet
- Patient Controlled AnalgesiaDocument35 pagesPatient Controlled AnalgesiamochkurniawanNo ratings yet
- Pharma Evaluation 3Document13 pagesPharma Evaluation 3janina mykaNo ratings yet
- Drug Study SurgeryDocument1 pageDrug Study SurgerygorgeazNo ratings yet
- Amended Intravenous Unfractionated Heparin Recommended StandardDocument4 pagesAmended Intravenous Unfractionated Heparin Recommended StandardTOJO JOSEPH TOMNo ratings yet
- Acetaminophen ToxicityDocument16 pagesAcetaminophen ToxicityMohil PratapNo ratings yet
- Medication Review (Example of Patient Questionnaire)Document3 pagesMedication Review (Example of Patient Questionnaire)Sophia AndresNo ratings yet
- VTE - Treating With The Right Anticoagulant and Duration (May 2018)Document6 pagesVTE - Treating With The Right Anticoagulant and Duration (May 2018)Dexter SiaNo ratings yet
- NOACs DOACs Coagulation Tests 2018nov16Document5 pagesNOACs DOACs Coagulation Tests 2018nov16Agam AsikNo ratings yet
- Doac Switch Guidance Oct 2016Document1 pageDoac Switch Guidance Oct 2016RouaNo ratings yet
- ASA Physical Status ClassificationDocument5 pagesASA Physical Status Classificationpolushky100% (1)
- Massive Haemorrhage Protocol (MHP) : Lead Clinician Activates MHPDocument1 pageMassive Haemorrhage Protocol (MHP) : Lead Clinician Activates MHPonlyhamsterNo ratings yet
- Heparin Royal Protocol SRBDocument3 pagesHeparin Royal Protocol SRBВладимир НовковићNo ratings yet
- Clinical Practice Guide On Antithrombotic Drug Dosing and Management of Antithrombotic Drug-Associated Bleeding Complications in AdultsDocument8 pagesClinical Practice Guide On Antithrombotic Drug Dosing and Management of Antithrombotic Drug-Associated Bleeding Complications in AdultsdarekshepardNo ratings yet
- Troponin PathwayDocument1 pageTroponin PathwayAllana AngelesNo ratings yet
- 7698alorithm SeizureDocument3 pages7698alorithm Seizureboromeus abyasa daniswara100% (1)
- WF Lab Clin TM Admin Quick Ref Adult CZDocument2 pagesWF Lab Clin TM Admin Quick Ref Adult CZAbu HuzaifaNo ratings yet
- PRADAXA: Dosing Guide: Starting Patients On PRADAXADocument2 pagesPRADAXA: Dosing Guide: Starting Patients On PRADAXAPapp Szodorai BeátaNo ratings yet
- Dat e Physicians Order RationaleDocument4 pagesDat e Physicians Order Rationaleember parkNo ratings yet
- ACLS ACS Algorithm NewDocument3 pagesACLS ACS Algorithm Newsambo100% (1)
- Rotherham CCG Asthma Guidelines FINAL MMC Version V6.1Document6 pagesRotherham CCG Asthma Guidelines FINAL MMC Version V6.1Verónica Rojas NavaNo ratings yet
- Myocardial Infarction Concept MapDocument7 pagesMyocardial Infarction Concept Mapkarelclarke629280% (5)
- Early Medical Abortion Procedure SummaryDocument1 pageEarly Medical Abortion Procedure SummaryNusratNo ratings yet
- Generic Name: Pre-Administration Assessment: Post Administration Evaluation: Nursing ConsiderationsDocument16 pagesGeneric Name: Pre-Administration Assessment: Post Administration Evaluation: Nursing ConsiderationsIsabella SamsonNo ratings yet
- AIIMS/ ICMR-COVID-19 National Task Force/ Joint Monitoring Group (Dte - GHS) Ministry of Health & Family Welfare, Government of IndiaDocument1 pageAIIMS/ ICMR-COVID-19 National Task Force/ Joint Monitoring Group (Dte - GHS) Ministry of Health & Family Welfare, Government of IndiaSomnath Das GuptaNo ratings yet
- Central Neuraxial & Plexus Block in Presence of Anticoagulant & Antiplatelet MedicationDocument41 pagesCentral Neuraxial & Plexus Block in Presence of Anticoagulant & Antiplatelet MedicationIndrani HemantkumarNo ratings yet
- Antithrombotics and Neuraxial Anesthesia GuidelineDocument6 pagesAntithrombotics and Neuraxial Anesthesia Guidelinelokeswara reddyNo ratings yet
- Guideline 133FM PDFDocument13 pagesGuideline 133FM PDFPangestu DhikaNo ratings yet
- AlgorithmsDocument16 pagesAlgorithmsirish laglevaNo ratings yet
- ACLS - Guidelines From 2005USADocument62 pagesACLS - Guidelines From 2005USAsbontchevNo ratings yet
- Phase 4 Medicine Intended Learning Outcomes (Ilos)Document19 pagesPhase 4 Medicine Intended Learning Outcomes (Ilos)AmaNo ratings yet
- Eportfolio User Guide For Trainees: March 2009Document30 pagesEportfolio User Guide For Trainees: March 2009AmaNo ratings yet
- Case 2 ReflectionDocument5 pagesCase 2 ReflectionAmaNo ratings yet
- Spirit of ScotlandDocument1 pageSpirit of ScotlandAmaNo ratings yet
- Directory of Services PDFDocument11 pagesDirectory of Services PDFogo IbuNo ratings yet
- Update Stock PT KMD 14-6Document46 pagesUpdate Stock PT KMD 14-6rio1995No ratings yet
- JR 2 Prosthodontic Treatment in Patients With Temporomandibular Disorders and Orofacial Pain And:or BruxismDocument10 pagesJR 2 Prosthodontic Treatment in Patients With Temporomandibular Disorders and Orofacial Pain And:or Bruxismaulia zahroNo ratings yet
- DyspepsiaDocument8 pagesDyspepsiaaspNo ratings yet
- Abrazo West Celebrates Five YearsDocument1 pageAbrazo West Celebrates Five YearsAnonymous jxvAZce4No ratings yet
- Eteeap - NCM 106 Page 1Document5 pagesEteeap - NCM 106 Page 1Marisol Jane JomayaNo ratings yet
- Ikatan TaliDocument11 pagesIkatan TaliPRA1062021 Nursyahzrenda Atasha Binti Mohamad AzliNo ratings yet
- Wound Care Observation Checklist - FINALDocument2 pagesWound Care Observation Checklist - FINALHagar HanounNo ratings yet
- SDH Customized NQAS Checklists TN 27.12.2021Document165 pagesSDH Customized NQAS Checklists TN 27.12.2021saravananNo ratings yet
- Div Memo On Wellness Program and PoliciesDocument2 pagesDiv Memo On Wellness Program and PoliciesBen Jan BasiliscoNo ratings yet
- LabsDocument19 pagesLabsmobilevasNo ratings yet
- MFD Exam Regulations November 2014Document17 pagesMFD Exam Regulations November 2014guajacolNo ratings yet
- Sexual Problems EssayDocument2 pagesSexual Problems EssayPAMELA CLAUDIA SORIANo ratings yet
- Check-List Enclosures (Dissertation) : Amit Documents For DissertationDocument14 pagesCheck-List Enclosures (Dissertation) : Amit Documents For DissertationAmit TamboliNo ratings yet
- Brit J Clinical Pharma - 2021 - Tusino - Rethinking The Role of Research Ethics Committees in The Light of Regulation EUDocument7 pagesBrit J Clinical Pharma - 2021 - Tusino - Rethinking The Role of Research Ethics Committees in The Light of Regulation EUCanache DamianNo ratings yet
- WockhardtDocument22 pagesWockhardtArpit GuptaNo ratings yet
- Ebr MacalolotDocument4 pagesEbr Macalolotquen.chuaNo ratings yet
- 225 DIV1 5503623 Personal+SpecificationDocument28 pages225 DIV1 5503623 Personal+SpecificationDr Pranesh BalasubramaniamNo ratings yet
- Notice: Applications, Hearings, Determinations, Etc.: Millette, Michael J., M.D.Document4 pagesNotice: Applications, Hearings, Determinations, Etc.: Millette, Michael J., M.D.Justia.comNo ratings yet
- Pamj 36 186Document9 pagesPamj 36 186PMKP RSIAANUGRAHNo ratings yet
- Client Satisfaction Questionnaire CSQ 8Document4 pagesClient Satisfaction Questionnaire CSQ 8Reyzza Mae EspenesinNo ratings yet
- Assignment For BSN 3 - A - RLEDocument2 pagesAssignment For BSN 3 - A - RLEKarina Madriaga100% (1)