You might also like
- 003 DkaDocument9 pages003 DkaMohammedNo ratings yet
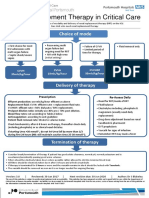
- Renal Replacement Therapy in Critical Care: Choice of ModeDocument15 pagesRenal Replacement Therapy in Critical Care: Choice of ModeJelena Obrenovic StankovicNo ratings yet
- Surviving Sepsis Campaign - NewDocument21 pagesSurviving Sepsis Campaign - NewIrfan SyakirNo ratings yet
- Patient Units Severe Sepsis Screening ToolDocument2 pagesPatient Units Severe Sepsis Screening ToolArnelli HutagalungNo ratings yet
- Sepsis Flow Chart FinalDocument2 pagesSepsis Flow Chart FinalDevindraPrptNo ratings yet
- Massive Transfusion Protocol-BbhDocument17 pagesMassive Transfusion Protocol-Bbhkrgdurai100% (1)
- DR. DR Umar Zein, SP - PD DTM&H - New Generation Antibiotic in SepsisDocument27 pagesDR. DR Umar Zein, SP - PD DTM&H - New Generation Antibiotic in SepsisOlivia DwimaswastiNo ratings yet
- D 8 Rate of Infusion For Blood Products V3Document2 pagesD 8 Rate of Infusion For Blood Products V3Abu HuzaifaNo ratings yet
- Kegawatdaruratan Bidang Ilmu Penyakit Dalam: I.Penyakit Dalam - MIC/ICU FK - UNPAD - RS DR - Hasan Sadikin BandungDocument47 pagesKegawatdaruratan Bidang Ilmu Penyakit Dalam: I.Penyakit Dalam - MIC/ICU FK - UNPAD - RS DR - Hasan Sadikin BandungEfa FathurohmiNo ratings yet
- Adrenal CrisisDocument27 pagesAdrenal CrisissayednourNo ratings yet
- Reviewer Special Blood Collection and PointDocument8 pagesReviewer Special Blood Collection and PointRicanie CadornaNo ratings yet
- Induced HPDocument4 pagesInduced HPmaddythedocNo ratings yet
- SKILL STATION Management of Critically Ill Patient With Septic Shock Provider GuideDocument27 pagesSKILL STATION Management of Critically Ill Patient With Septic Shock Provider GuidesrinidhiNo ratings yet
- PT, Aptt, TTDocument44 pagesPT, Aptt, TTswaraj sharmaNo ratings yet
- Traumatic Brain Injury 2023Document17 pagesTraumatic Brain Injury 2023Fernando Martinez AguilarNo ratings yet
- Adult: Diabetic Emergencies: Care Protocol and ChartDocument4 pagesAdult: Diabetic Emergencies: Care Protocol and ChartvladhdNo ratings yet
- Renal Replacement Therapy in Critical Care: Choice of ModeDocument15 pagesRenal Replacement Therapy in Critical Care: Choice of ModePeter AgabaNo ratings yet
- Nursing Sciences: Pyramid PointsDocument12 pagesNursing Sciences: Pyramid PointsEmmanuel GarciaNo ratings yet
- Peri - Operative ManagementDocument32 pagesPeri - Operative Managementrichamalik99No ratings yet
- Baseline:: Notify Transfusion Laboratory To: Activate MTP'. Footscray: 56292 Sunshine: 51480 Allocate Team RolesDocument2 pagesBaseline:: Notify Transfusion Laboratory To: Activate MTP'. Footscray: 56292 Sunshine: 51480 Allocate Team RolesDumindu PereraNo ratings yet
- Coaguchek & International Normalization Ratio (Inr) : SpeakerDocument26 pagesCoaguchek & International Normalization Ratio (Inr) : Speakerswaraj sharma100% (1)
- Course Task CU 7Document7 pagesCourse Task CU 7Kyla PamaNo ratings yet
- Blood AdministrationDocument35 pagesBlood AdministrationnurminieNo ratings yet
- ASA Physical Status ClassificationDocument5 pagesASA Physical Status Classificationpolushky100% (1)
- Endorsement of Aling AnnaDocument2 pagesEndorsement of Aling AnnaTom CuencaNo ratings yet
- Packed Red Cells: Administration of Blood ProductsDocument36 pagesPacked Red Cells: Administration of Blood ProductsRj SantosNo ratings yet
- Royal Hospital For Women: Clinical Policies, Procedures & Guidelines ManualDocument5 pagesRoyal Hospital For Women: Clinical Policies, Procedures & Guidelines ManualahmadsebastianakbarNo ratings yet
- Surviving Sepsis CampaignDocument16 pagesSurviving Sepsis CampaignKHAIRUL REDZUANNo ratings yet
- DKA Guidelines Version 4.0 28 Dec 2016FINALDocument4 pagesDKA Guidelines Version 4.0 28 Dec 2016FINALbenNo ratings yet
- Day in The Life 2019Document30 pagesDay in The Life 2019Hoa Cỏ ĐậuNo ratings yet
- Advance Cardiac Life Support (ACLS)Document13 pagesAdvance Cardiac Life Support (ACLS)Nozomi YukiNo ratings yet
- Haemorrhage ProtocolDocument1 pageHaemorrhage ProtocolHerwinda GeraldineNo ratings yet
- 12a Diabetic Emergencies DKA Case StudiesDocument13 pages12a Diabetic Emergencies DKA Case StudiesAnonymous yTdBi7100% (1)
- Blood TransfusionDocument52 pagesBlood TransfusionAnonymous GC8uMx367% (3)
- 8.1 - Cases - ViralDocument25 pages8.1 - Cases - Viralkoteshwara raoNo ratings yet
- Laboratory Control of Anticoagulant Therapy - PPTX LectDocument69 pagesLaboratory Control of Anticoagulant Therapy - PPTX LectTusabe FredNo ratings yet
- NURS 2028 Quiz 1 Review Lab SkillsDocument13 pagesNURS 2028 Quiz 1 Review Lab SkillsNicholas ObasiNo ratings yet
- Paper Telaah Jurnal Evidence Based Practice Keperawatan Kritis Dengan Judul Treatment of Patients With Severe Sepsis and Septic ShockDocument11 pagesPaper Telaah Jurnal Evidence Based Practice Keperawatan Kritis Dengan Judul Treatment of Patients With Severe Sepsis and Septic ShockTheresia AvilaNo ratings yet
- Blood Component Therapy F17Document33 pagesBlood Component Therapy F17Crystal LynaeNo ratings yet
- Nursing Care PlanDocument10 pagesNursing Care PlanZerica Andaca83% (6)
- PBM Module1 MTP Template 0Document2 pagesPBM Module1 MTP Template 0Daniela Marie RonquilloNo ratings yet
- NCP For Delivery RoomDocument4 pagesNCP For Delivery RoomGiselle EstoquiaNo ratings yet
- DKA PosterDocument2 pagesDKA PosterainizatiNo ratings yet
- JBDS 02 Single Page Pathway Amended June 2021Document2 pagesJBDS 02 Single Page Pathway Amended June 2021Oliverio MéndezNo ratings yet
- What Documents Do You Need After A Blood Transfusion?: BT Checklist 1Document5 pagesWhat Documents Do You Need After A Blood Transfusion?: BT Checklist 1Edelweiss Marie CayetanoNo ratings yet
- Disseminated Intravascular CoagulationDocument37 pagesDisseminated Intravascular CoagulationMuhammad Adeeb100% (1)
- Coronary Artery DiseaseDocument32 pagesCoronary Artery DiseasecjissamNo ratings yet
- OB HMRGDocument11 pagesOB HMRGpaulaNo ratings yet
- Blood and Blood Components-LectureDocument13 pagesBlood and Blood Components-LectureMelissa GinesNo ratings yet
- 24hr Fluid Balance ADULT Chart - v3Document2 pages24hr Fluid Balance ADULT Chart - v3anggita diah100% (1)
- Acute Stroke Nursing GuidelineFINAL 1 2Document5 pagesAcute Stroke Nursing GuidelineFINAL 1 2radanikmaNo ratings yet
- Hash Hash-Basema-AliDocument2 pagesHash Hash-Basema-AliBasema HashhashNo ratings yet
- NCP2 - DengueDocument4 pagesNCP2 - DengueSummer SuarezNo ratings yet
- Flow Chart For Diabetic Ketoacidosis in Adults Management ofDocument1 pageFlow Chart For Diabetic Ketoacidosis in Adults Management ofsheryl maeNo ratings yet
- Ventura County Medical Center: Mi Thrombolysis, Management ofDocument3 pagesVentura County Medical Center: Mi Thrombolysis, Management ofblackcat657No ratings yet
- From SIRS To Septic Shock (2022!01!22 00-25-28 UTC)Document1 pageFrom SIRS To Septic Shock (2022!01!22 00-25-28 UTC)Andrea AndradaNo ratings yet
- Severe TBI 2017Document18 pagesSevere TBI 2017DM internaNo ratings yet
- Nursing Care Plan 6 Impaired Gas ExchangeDocument9 pagesNursing Care Plan 6 Impaired Gas Exchangedbryant0101100% (12)
- Orthopedic Inpatient Protocols: A Guide to Orthopedic Inpatient RoundingFrom EverandOrthopedic Inpatient Protocols: A Guide to Orthopedic Inpatient RoundingNo ratings yet
- C SuiteDocument10 pagesC SuiteTom BiusoNo ratings yet
- TAVR CostsDocument11 pagesTAVR CostsTom BiusoNo ratings yet
- SGLT2 IDocument23 pagesSGLT2 ITom BiusoNo ratings yet
- Farmacos y Diabetes 2023Document18 pagesFarmacos y Diabetes 2023Valentina GonzalezNo ratings yet
- Chronic Kidney DiseaseDocument12 pagesChronic Kidney DiseaseTom BiusoNo ratings yet
- TV TeerDocument15 pagesTV TeerTom BiusoNo ratings yet
- Standards of Care in Diabetes - 2023: 10. Cardiovascular Disease and Risk ManagementDocument33 pagesStandards of Care in Diabetes - 2023: 10. Cardiovascular Disease and Risk ManagementMenethil Terenas ElijiahNo ratings yet
- Glycemic Targets Standards of Care in Diabetes-2023Document14 pagesGlycemic Targets Standards of Care in Diabetes-2023ÁngelesNo ratings yet
- Capital StructureDocument12 pagesCapital StructureTom BiusoNo ratings yet
- ECGsDocument4 pagesECGsTom BiusoNo ratings yet
- Insurer Market PowerDocument7 pagesInsurer Market PowerTom BiusoNo ratings yet
- TAVR Low RiskDocument5 pagesTAVR Low RiskTom BiusoNo ratings yet
- Bill Evans - Quiet NowDocument9 pagesBill Evans - Quiet NowTom Biuso100% (2)
- Expenses 2020Document7 pagesExpenses 2020Tom BiusoNo ratings yet
- Aortic StenosisDocument11 pagesAortic StenosisTom BiusoNo ratings yet
- Pharmacologic Diabetes 2022Document19 pagesPharmacologic Diabetes 2022Tom BiusoNo ratings yet
- Aortic StenosisDocument11 pagesAortic StenosisTom BiusoNo ratings yet
- NCDRDocument9 pagesNCDRTom BiusoNo ratings yet
- STLDDocument9 pagesSTLDTom BiusoNo ratings yet
- Personality DisorderDocument8 pagesPersonality DisorderTom BiusoNo ratings yet
- Acute Inferior Wall Myocardial Infarction: What Is The Culprit Artery?Document3 pagesAcute Inferior Wall Myocardial Infarction: What Is The Culprit Artery?Tom BiusoNo ratings yet
- Cardiovascular Diabetes 2022Document31 pagesCardiovascular Diabetes 2022Tom BiusoNo ratings yet
- Where To InvestDocument7 pagesWhere To InvestTom BiusoNo ratings yet
- Anaphylaxis: Emergency Department TreatmentDocument14 pagesAnaphylaxis: Emergency Department TreatmentTom BiusoNo ratings yet
- D-Dimer Testing For The Exclusion of Pulmonary Embolism Among Hospitalized Patients With COVID-19Document4 pagesD-Dimer Testing For The Exclusion of Pulmonary Embolism Among Hospitalized Patients With COVID-19Tom BiusoNo ratings yet
- 7 Beaten-Up Tech Stocks That Could Be Bargains: Connor SmithDocument3 pages7 Beaten-Up Tech Stocks That Could Be Bargains: Connor SmithTom BiusoNo ratings yet
- The Medical Letter: On Drugs and TherapeuticsDocument11 pagesThe Medical Letter: On Drugs and TherapeuticsTom BiusoNo ratings yet
- When Do I Give Fluids?Document14 pagesWhen Do I Give Fluids?Tom BiusoNo ratings yet
- Home Based CareDocument13 pagesHome Based CareTom BiusoNo ratings yet
- Equianalgesic Dose Initial Adult Dose (Adults 50kg) Drug CommentsDocument2 pagesEquianalgesic Dose Initial Adult Dose (Adults 50kg) Drug CommentsTom BiusoNo ratings yet
- Task 1: Choose The Present Simple, The Present Continuous, The PresentDocument5 pagesTask 1: Choose The Present Simple, The Present Continuous, The PresentAlexandra KupriyenkoNo ratings yet
- A Letter From Sir William R. Hamilton To John T. Graves, EsqDocument7 pagesA Letter From Sir William R. Hamilton To John T. Graves, EsqJoshuaHaimMamouNo ratings yet
- July 2006 Bar Exam Louisiana Code of Civil ProcedureDocument11 pagesJuly 2006 Bar Exam Louisiana Code of Civil ProcedureDinkle KingNo ratings yet
- Houses WorksheetDocument3 pagesHouses WorksheetYeferzon Clavijo GilNo ratings yet
- A History of The Church Part 1 (1) Coverage of Midterm ExamDocument117 pagesA History of The Church Part 1 (1) Coverage of Midterm ExamMary CecileNo ratings yet
- LEARNING MODULE Entrep Lesson 1-2Document19 pagesLEARNING MODULE Entrep Lesson 1-2Cindy BononoNo ratings yet
- Chapter 4 Higher Order Differential EquationsDocument50 pagesChapter 4 Higher Order Differential EquationsAlaa TelfahNo ratings yet
- King of Chess American English American English TeacherDocument6 pagesKing of Chess American English American English TeacherJuliana FigueroaNo ratings yet
- SurrealismDocument121 pagesSurrealismLaurence SamonteNo ratings yet
- Pier Cap Corbel 30m SGDocument3 pagesPier Cap Corbel 30m SGSM ConsultantsNo ratings yet
- Phase/State Transitions of Confectionery Sweeteners: Thermodynamic and Kinetic AspectsDocument16 pagesPhase/State Transitions of Confectionery Sweeteners: Thermodynamic and Kinetic AspectsAlicia MartinezNo ratings yet
- Unit 2 Lab Manual ChemistryDocument9 pagesUnit 2 Lab Manual ChemistryAldayne ParkesNo ratings yet
- Lecture 4 - Consumer ResearchDocument43 pagesLecture 4 - Consumer Researchnvjkcvnx100% (1)
- S1-TITAN Overview BrochureDocument8 pagesS1-TITAN Overview BrochureصصNo ratings yet
- Diec Russias Demographic Policy After 2000 2022Document29 pagesDiec Russias Demographic Policy After 2000 2022dawdowskuNo ratings yet
- Leadership and Turnaround Management Concepts Applied in The Agribusiness Environment in RomaniaDocument6 pagesLeadership and Turnaround Management Concepts Applied in The Agribusiness Environment in RomaniaLoredana PredaNo ratings yet
- World Price List 2014: Adventys Induction Counter TopsDocument4 pagesWorld Price List 2014: Adventys Induction Counter TopsdiogocorollaNo ratings yet
- Chest Physiotherapy BPTDocument20 pagesChest Physiotherapy BPTWraith GAMINGNo ratings yet
- Family Decision MakingDocument23 pagesFamily Decision MakingNishant AnandNo ratings yet
- Excavations OSHA 2226Document44 pagesExcavations OSHA 2226Al DubNo ratings yet
- Eric Thomas Grissen - The American Technology Awards, or "The Termans"Document1 pageEric Thomas Grissen - The American Technology Awards, or "The Termans"Eric Thomas GrissenNo ratings yet
- General Mathematics-FINALDocument187 pagesGeneral Mathematics-FINALDummy AccountNo ratings yet
- Past Paper1Document8 pagesPast Paper1Ne''ma Khalid Said Al HinaiNo ratings yet
- Verb TensesDocument3 pagesVerb TensesVeronicaGelfgren92% (12)
- Journal of Exceptional Experiences and PDocument62 pagesJournal of Exceptional Experiences and Pbinzegger100% (1)
- MKTG4471Document9 pagesMKTG4471Aditya SetyaNo ratings yet
- Aptitude For Civil ServicesDocument17 pagesAptitude For Civil Servicesnagarajuvcc123No ratings yet
- Evolut Pro Mini Product Brochure PDFDocument8 pagesEvolut Pro Mini Product Brochure PDFBalázs PalcsikNo ratings yet
- Sajid, Aditya (Food Prossing)Document29 pagesSajid, Aditya (Food Prossing)Asif SheikhNo ratings yet
- Business Research Chapter 1Document27 pagesBusiness Research Chapter 1Toto H. Ali100% (2)