You might also like
- Worksheets - Isbar 1Document3 pagesWorksheets - Isbar 1api-673621869No ratings yet
- Pedia Census ArrythmiaDocument48 pagesPedia Census ArrythmiaBhi-An BatobalonosNo ratings yet
- Mang Raul Case StudyDocument3 pagesMang Raul Case StudyTom CuencaNo ratings yet
- Aling Marites Case Study:: Endorsement ForDocument4 pagesAling Marites Case Study:: Endorsement ForTom CuencaNo ratings yet
- IANs Presentation - Atrial Fibrillation (RMO Kerenga)Document26 pagesIANs Presentation - Atrial Fibrillation (RMO Kerenga)Samuel.MoriNo ratings yet
- Morbidity April 2022: Aileen Concepcion M. AgustinDocument24 pagesMorbidity April 2022: Aileen Concepcion M. AgustinConcepcion R. AquinoNo ratings yet
- RRT With Emphasis On PD (Recovered)Document92 pagesRRT With Emphasis On PD (Recovered)Seyi AdeogunNo ratings yet
- OR CommsDocument4 pagesOR CommsAngela NeriNo ratings yet
- Case StudyDocument20 pagesCase StudyYiella AlagarNo ratings yet
- Mortality by YvonneDocument25 pagesMortality by YvonneYvonne SiiloNo ratings yet
- Purnachandrao Death PPT FINALDocument38 pagesPurnachandrao Death PPT FINALkalyanpavuralaNo ratings yet
- Case Presentation: EclampsiaDocument44 pagesCase Presentation: Eclampsiamutiara sitepuNo ratings yet
- 3 - Bacterial Sepsis - Case 1Document36 pages3 - Bacterial Sepsis - Case 1koteshwara raoNo ratings yet
- CBL Perforated Peptic Ulcer'Document10 pagesCBL Perforated Peptic Ulcer'KubendranArikrishnanNo ratings yet
- Malignant Hyperthermia: Review and Case Studies Holly Price, CRNADocument48 pagesMalignant Hyperthermia: Review and Case Studies Holly Price, CRNAnurse_kellyNo ratings yet
- DKAPPTxDocument34 pagesDKAPPTxMuhammad FurqanNo ratings yet
- Doctor's OrderDocument2 pagesDoctor's OrderWiljohn de la CruzNo ratings yet
- Sample Fous Charting Templates: Nurses' Progress Notes AdmissionDocument10 pagesSample Fous Charting Templates: Nurses' Progress Notes AdmissionLevy Garcia Sanchez100% (1)
- The PatientDocument9 pagesThe PatientJan Crizza Dale R. FrancoNo ratings yet
- Case Scenario BronchitisDocument4 pagesCase Scenario BronchitisJamelyn AsuncionNo ratings yet
- EclampsiaDocument31 pagesEclampsiaMona SayanikaNo ratings yet
- Advance Cardiac Life Support (ACLS)Document13 pagesAdvance Cardiac Life Support (ACLS)Nozomi YukiNo ratings yet
- Nursing Care PlanDocument10 pagesNursing Care PlanZerica Andaca83% (6)
- Case Presentation On Perforated Gastric Ulcer With Alcoholic Cirrhosis and Tongue CancerDocument19 pagesCase Presentation On Perforated Gastric Ulcer With Alcoholic Cirrhosis and Tongue CancerUmme habeebaNo ratings yet
- 02NTD 2022 - Approach To Severe DengueDocument54 pages02NTD 2022 - Approach To Severe DengueInstitute for Clinical ResearchNo ratings yet
- OB HMRGDocument11 pagesOB HMRGpaulaNo ratings yet
- NCP, FHP, and Pharma Card of Patient R.K. With Myocardial InfarctionDocument21 pagesNCP, FHP, and Pharma Card of Patient R.K. With Myocardial InfarctionJoi Owen Yap TevesNo ratings yet
- Patient Update Day 4Document2 pagesPatient Update Day 4Jamie LeeNo ratings yet
- Diabetes: Section B2 - Group 5Document49 pagesDiabetes: Section B2 - Group 5Marvin OcampoNo ratings yet
- General Data and Chief ComplaintDocument21 pagesGeneral Data and Chief ComplaintAyen FornollesNo ratings yet
- F - Case Scenario Peritoneal Dialysis - PDF - 173767042Document5 pagesF - Case Scenario Peritoneal Dialysis - PDF - 173767042yumulNo ratings yet
- 37 Page Revised NCLEXDocument38 pages37 Page Revised NCLEXJohnasse Sebastian NavalNo ratings yet
- Camba-Course Task 4Document5 pagesCamba-Course Task 4Rachelle CambaNo ratings yet
- Cardiovascular 4416Document5 pagesCardiovascular 4416api-3703191No ratings yet
- New Format MasterDocument34 pagesNew Format MasterMuhammad FurqanNo ratings yet
- 0730 Cunningham Fluids and Electrolytes 2012Document19 pages0730 Cunningham Fluids and Electrolytes 2012Wan HafizNo ratings yet
- Februari, 22 Morning ReportDocument25 pagesFebruari, 22 Morning Reportnadia shabriNo ratings yet
- Grand Rounds: Roxanne Jeen L. Fornolles, M.DDocument61 pagesGrand Rounds: Roxanne Jeen L. Fornolles, M.DRj FornollesNo ratings yet
- Microsoft Word Oxygenation Handouts 2007 Nclex 1232010737844931 1Document23 pagesMicrosoft Word Oxygenation Handouts 2007 Nclex 1232010737844931 1api-19824701100% (1)
- Cedar Crest College Clinical and Concept Map Worksheet For Nursing 330 PediatricsDocument17 pagesCedar Crest College Clinical and Concept Map Worksheet For Nursing 330 Pediatricsapi-380115954No ratings yet
- Cva Case STROKEDocument27 pagesCva Case STROKEUmme habeebaNo ratings yet
- SampleCharting 418Document2 pagesSampleCharting 418Lai KuanlinNo ratings yet
- Assessing Vital Signs HandoutsDocument9 pagesAssessing Vital Signs Handoutsyhudz100% (3)
- Mariano Marcos State University: College of Health SciencesDocument3 pagesMariano Marcos State University: College of Health SciencesJoshua GonzalesNo ratings yet
- GE BasavaDocument21 pagesGE BasavaAmalin PrãdhãñNo ratings yet
- TablesDocument21 pagesTablesMélissa BlancNo ratings yet
- Alcoholic Hepatitis C5Document15 pagesAlcoholic Hepatitis C5srija vijjapuNo ratings yet
- Dka NewDocument37 pagesDka NewMuhammad FurqanNo ratings yet
- Case Report A Patient With Severe MalariaDocument38 pagesCase Report A Patient With Severe MalariaGloria ThomasNo ratings yet
- Tumor Lysis Oral Boards CasesDocument15 pagesTumor Lysis Oral Boards Casesczalesky66No ratings yet
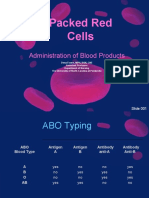
- Packed Red Cells: Administration of Blood ProductsDocument36 pagesPacked Red Cells: Administration of Blood ProductsRj SantosNo ratings yet
- Hypertermia CrisisDocument1 pageHypertermia CrisislisaNo ratings yet
- Case Scenario 1Document3 pagesCase Scenario 1AC SantosNo ratings yet
- Placenta Previa: G4 T2 P0 A1 L2Document42 pagesPlacenta Previa: G4 T2 P0 A1 L2SteffiNo ratings yet
- From SIRS To Septic Shock (2022!01!22 00-25-28 UTC)Document1 pageFrom SIRS To Septic Shock (2022!01!22 00-25-28 UTC)Andrea AndradaNo ratings yet
- TB-meningitis CPCDocument47 pagesTB-meningitis CPCPed SilvestreNo ratings yet
- DicDocument5 pagesDicmarielleNo ratings yet
- NCP TorresDocument7 pagesNCP TorresbabiNo ratings yet
- Coarse in The WardDocument41 pagesCoarse in The WardPandesal with EggNo ratings yet
- Previous BON Files (MCHN)Document13 pagesPrevious BON Files (MCHN)Tom CuencaNo ratings yet
- Previous BON Files (Leadership, Management, Bioethics and Research)Document11 pagesPrevious BON Files (Leadership, Management, Bioethics and Research)Tom CuencaNo ratings yet
- Previous BON Files (Community Health Nursing)Document10 pagesPrevious BON Files (Community Health Nursing)Tom CuencaNo ratings yet
- Tiktok Pilit-PilitDocument1 pageTiktok Pilit-PilitTom CuencaNo ratings yet
- Previous BON Files (Medical-Surgical Nursing)Document14 pagesPrevious BON Files (Medical-Surgical Nursing)Tom CuencaNo ratings yet
- Previous BON Files (Foundation of Professional Nursing Practice)Document16 pagesPrevious BON Files (Foundation of Professional Nursing Practice)Tom Cuenca100% (1)
- Extra Minor PageDocument2 pagesExtra Minor PageTom CuencaNo ratings yet
- (HCE) Prelims Trans 5Document1 page(HCE) Prelims Trans 5Tom CuencaNo ratings yet
- (HCE) Prelims Trans 4Document1 page(HCE) Prelims Trans 4Tom CuencaNo ratings yet
- Extra Major PageDocument2 pagesExtra Major PageTom CuencaNo ratings yet
- Evidence Based Research: EBR #1 Name: April Tom O. CuencaDocument1 pageEvidence Based Research: EBR #1 Name: April Tom O. CuencaTom CuencaNo ratings yet
- Day 1 Daily Objectives KyangDocument1 pageDay 1 Daily Objectives KyangTom CuencaNo ratings yet
- (GN) (Cuenca) E-ProjectDocument12 pages(GN) (Cuenca) E-ProjectTom CuencaNo ratings yet
- Prioritization of Problems Rank Problem Identified: San Francisco St. Butuan City 8600, Region XIII Caraga, PhilippinesDocument5 pagesPrioritization of Problems Rank Problem Identified: San Francisco St. Butuan City 8600, Region XIII Caraga, PhilippinesTom CuencaNo ratings yet
- (GN) Introduction To AgingDocument3 pages(GN) Introduction To AgingTom CuencaNo ratings yet
- Prednisone Drug StudyDocument4 pagesPrednisone Drug StudyTom CuencaNo ratings yet
- (CUENCA) Reliability Analysis InterpretationDocument1 page(CUENCA) Reliability Analysis InterpretationTom CuencaNo ratings yet
- Prioritization of Problems Rank Problem Identified: San Francisco St. Butuan City 8600, Region XIII Caraga, PhilippinesDocument5 pagesPrioritization of Problems Rank Problem Identified: San Francisco St. Butuan City 8600, Region XIII Caraga, PhilippinesTom CuencaNo ratings yet
- Prioritization of Problems Rank Problem Identified: San Francisco St. Butuan City 8600, Region XIII Caraga, PhilippinesDocument5 pagesPrioritization of Problems Rank Problem Identified: San Francisco St. Butuan City 8600, Region XIII Caraga, PhilippinesTom CuencaNo ratings yet
- (CHNLAB) Family Health Care Researches #1Document1 page(CHNLAB) Family Health Care Researches #1Tom CuencaNo ratings yet
- (PCOL) Gastrointestinal Drugs (Drug Study #2)Document1 page(PCOL) Gastrointestinal Drugs (Drug Study #2)Tom CuencaNo ratings yet
- Case Study AlcoholismDocument31 pagesCase Study Alcoholismilakkiya ilakkiya100% (8)
- Prevention of Pin Site Infection in External FixatioDocument11 pagesPrevention of Pin Site Infection in External FixatioKim Gabrielle Exene LeeNo ratings yet
- Cara Membaca Foto Thoraks Yang BaikDocument2 pagesCara Membaca Foto Thoraks Yang BaikIdi Nagan RayaNo ratings yet
- Worksheet - Respiratory SystemDocument8 pagesWorksheet - Respiratory SystemDhen MarcNo ratings yet
- DR Dina - TB & CovidDocument10 pagesDR Dina - TB & CovidDina FaizahNo ratings yet
- Psychological Problems and Coping Strategies Adopted by Post Menopausal WomenDocument9 pagesPsychological Problems and Coping Strategies Adopted by Post Menopausal WomenJannica Mae D SacristiaNo ratings yet
- CSOMDocument29 pagesCSOMsuciNo ratings yet
- 52111-Article Text-79480-1-10-20100302Document3 pages52111-Article Text-79480-1-10-20100302jaheerNo ratings yet
- Ozone Therapy by Saul Pressman at Oxygen Therapies Support Forum, Topic 443552 PDFDocument15 pagesOzone Therapy by Saul Pressman at Oxygen Therapies Support Forum, Topic 443552 PDFHello MisterNo ratings yet
- Fever in Children With ChemoteraphyDocument23 pagesFever in Children With ChemoteraphyImanuel Far-FarNo ratings yet
- BPT Notes Applied PsychologyDocument36 pagesBPT Notes Applied PsychologyVivek Chandra0% (1)
- Benefits of Living DonationDocument1 pageBenefits of Living DonationRanga RajanNo ratings yet
- 001 201056034 CF6 117 6Document1 page001 201056034 CF6 117 6RSNo ratings yet
- Bone Mineral Density (BMD) Test 2Document1 pageBone Mineral Density (BMD) Test 2Rica adriani SantikaNo ratings yet
- BFSA-Volume 46-Issue 1 - Page 647-657Document11 pagesBFSA-Volume 46-Issue 1 - Page 647-657mizranitaNo ratings yet
- IBRDocument2 pagesIBRAde HermawanNo ratings yet
- E-Book C Arms-NewDocument9 pagesE-Book C Arms-NewHugoNo ratings yet
- MEDISEP Hospital ListDocument3 pagesMEDISEP Hospital ListQ8123No ratings yet
- Answer Key EXAM DRILL 1 - Community Health Nursing Nursing Practice Ii - CHN and Care of The Mother and ChildDocument11 pagesAnswer Key EXAM DRILL 1 - Community Health Nursing Nursing Practice Ii - CHN and Care of The Mother and Childbetiful100% (5)
- Hubungan Ketepatan Penulisan Informasi Diagnosis Dengan Keakuratan Kode Diagnosis Kasus Obstetry Di Rumah Sakit Umi Barokah BoyolaliDocument5 pagesHubungan Ketepatan Penulisan Informasi Diagnosis Dengan Keakuratan Kode Diagnosis Kasus Obstetry Di Rumah Sakit Umi Barokah BoyolaliirmasariNo ratings yet
- Case Study Presentation On Diabetic Foot UlcerDocument61 pagesCase Study Presentation On Diabetic Foot UlcerBindu GC100% (1)
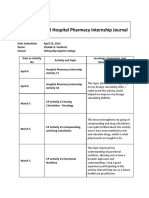
- Chokde Hudierez - Virtual Hospital Pharmacy Internship JournalDocument5 pagesChokde Hudierez - Virtual Hospital Pharmacy Internship JournalCHOKDE HUDIEREZNo ratings yet
- Anatomy & Physiology - Chapter 19: BLOOD Book Questions and AnswersDocument6 pagesAnatomy & Physiology - Chapter 19: BLOOD Book Questions and AnswersVanessa CarmodyNo ratings yet
- Hipertensi KrisisDocument30 pagesHipertensi KrisisLuthfan HakimNo ratings yet
- AJACM 2010 5 2 Wang Juyi Interview Part 1 of 2 - LiuDocument7 pagesAJACM 2010 5 2 Wang Juyi Interview Part 1 of 2 - LiuYagtaliNo ratings yet
- Bites by Crotalinae Snakes (Rattlesnakes, Water Moccasins (Cottonmouths), or Copperheads) in The United States - Management - UpToDateDocument19 pagesBites by Crotalinae Snakes (Rattlesnakes, Water Moccasins (Cottonmouths), or Copperheads) in The United States - Management - UpToDateAlin VázquezNo ratings yet
- Jurnal Daun Jati Cina Senna AlexandriaDocument7 pagesJurnal Daun Jati Cina Senna AlexandriaFransLei Vadoel SaelNo ratings yet
- 1 Latifah Jehloh - งานนำเสนอDocument41 pages1 Latifah Jehloh - งานนำเสนอAisyahNo ratings yet
- Olicy: Magna Carta of Public Health Workers: Does It Really Fulfill Its Intent?Document4 pagesOlicy: Magna Carta of Public Health Workers: Does It Really Fulfill Its Intent?Krystal Jane SalinasNo ratings yet
- NanoparticlesDocument18 pagesNanoparticlesMihaela BalasNo ratings yet