You might also like
- Naplex Complete Study Outline A Topic-Wise Approach DiabetesFrom EverandNaplex Complete Study Outline A Topic-Wise Approach DiabetesRating: 4 out of 5 stars4/5 (2)
- MBBS Made Easy, Second MBBS Examination, Manoj Vimal, Jaypee Bros., 2nd Edition 2009 PDFDocument329 pagesMBBS Made Easy, Second MBBS Examination, Manoj Vimal, Jaypee Bros., 2nd Edition 2009 PDFMonica KaranthNo ratings yet
- Hypertension in PregnancyDocument20 pagesHypertension in PregnancyFAMED RESIDENTS CESMED100% (1)
- Neurology revision-2015: Benztropine side effects & status epilepticus treatmentsDocument99 pagesNeurology revision-2015: Benztropine side effects & status epilepticus treatmentsPaz Vida100% (7)
- Medical-Surgical Nursing ReviewDocument90 pagesMedical-Surgical Nursing Reviewɹǝʍdןnos99% (312)
- Neurology Paediatric ProtocolDocument44 pagesNeurology Paediatric ProtocolkirannesarajahNo ratings yet
- ECT Manual-NIMHANS Ed.2 Compressed-2Document70 pagesECT Manual-NIMHANS Ed.2 Compressed-2Utkarsh Modi50% (6)
- AEMT Medication AdministrationDocument24 pagesAEMT Medication AdministrationEmily KeenNo ratings yet
- Guide to Diagnosing and Treating Neonatal ConvulsionsDocument42 pagesGuide to Diagnosing and Treating Neonatal ConvulsionsG Venkatesh100% (1)
- Drug List: Medication Adult Dosing Pediatric DosingDocument14 pagesDrug List: Medication Adult Dosing Pediatric DosingAndrew JamesNo ratings yet
- DRUG STUDY ON PROPOFOL FOR ICU SEDATIONDocument3 pagesDRUG STUDY ON PROPOFOL FOR ICU SEDATIONAngelica shane Navarro100% (2)
- Presentation EpilepsyDocument38 pagesPresentation EpilepsypertinenteNo ratings yet
- FLCCC Alliance's I RECOVER Management Protocol For Long Haul COVID 19 SyndromeDocument3 pagesFLCCC Alliance's I RECOVER Management Protocol For Long Haul COVID 19 SyndromeAlan N100% (1)
- Epinephrine and other emergency drug doses and indicationsDocument5 pagesEpinephrine and other emergency drug doses and indicationsColette Marie PerezNo ratings yet
- Seizures and Status Epilepticus - Management Practice Guideline ©Document12 pagesSeizures and Status Epilepticus - Management Practice Guideline ©ANDREWNo ratings yet
- Status EpilepticusDocument28 pagesStatus EpilepticusDaniel AlfredNo ratings yet
- Emergency Neurological Life Support Status Epilepticus ProtocolDocument12 pagesEmergency Neurological Life Support Status Epilepticus ProtocolFransiskus MikaelNo ratings yet
- Nursing Care Plan for 1-Year-Old Male Admitted for Dehydration and SeizuresDocument3 pagesNursing Care Plan for 1-Year-Old Male Admitted for Dehydration and SeizuresKwini Jeyn50% (2)
- Status EpilepticusDocument23 pagesStatus EpilepticusSimona LiaNo ratings yet
- Evaluation and Management of Status Epilepticus in ChildrenDocument13 pagesEvaluation and Management of Status Epilepticus in ChildrenAyan BiswasNo ratings yet
- Status Epilepticus GuidelineDocument1 pageStatus Epilepticus GuidelineYuzhi PhuahNo ratings yet
- ConnectorDocument4 pagesConnectoryetaung8No ratings yet
- Status Epilepticus: Kenya Medical Training CollegeDocument21 pagesStatus Epilepticus: Kenya Medical Training CollegeSalman KhanNo ratings yet
- Status EpilepticusDocument3 pagesStatus EpilepticusVandeosNo ratings yet
- Protocolo de Estatus EpilepticoDocument3 pagesProtocolo de Estatus EpilepticojiovannaescalanteNo ratings yet
- Status Epilepticus and ICPDocument9 pagesStatus Epilepticus and ICPjoomds51No ratings yet
- Child With Fits in ED - Srl.Document2 pagesChild With Fits in ED - Srl.azeemNo ratings yet
- Neonatal Seizures GuidelineDocument15 pagesNeonatal Seizures GuidelineNURUL NADIA BINTI MOHD NAZIR / UPMNo ratings yet
- Management of Status Epilepticus 2022Document8 pagesManagement of Status Epilepticus 2022albert siraitNo ratings yet
- Estatus EpilépticoDocument16 pagesEstatus EpilépticoLizbeth PalomecNo ratings yet
- Status Epilepticus - APLSDocument3 pagesStatus Epilepticus - APLSMuhammadafif SholehuddinNo ratings yet
- Status Epilepticus Pediatric DR - RPDocument4 pagesStatus Epilepticus Pediatric DR - RPAdnin NugrohoNo ratings yet
- Status Epilepticus: BY DR Muhammad Usman DR Areeba NaeemDocument16 pagesStatus Epilepticus: BY DR Muhammad Usman DR Areeba NaeemFarhan AfzalNo ratings yet
- DroperidolDocument1 pageDroperidolIvanne HisolerNo ratings yet
- Metoclopramide for Nausea, GERD and GastroparesisDocument2 pagesMetoclopramide for Nausea, GERD and GastroparesisBeatrizz P GellaNo ratings yet
- Protocol For in Patient Status Epilepticus in Adults (Includes Convulsive and Non-Convulsive Status Epilepticus)Document3 pagesProtocol For in Patient Status Epilepticus in Adults (Includes Convulsive and Non-Convulsive Status Epilepticus)BarneyNo ratings yet
- Agitated PatientDocument2 pagesAgitated PatientCassandra GeldenhuysNo ratings yet
- Paediatric Clinical GuidelinesDocument7 pagesPaediatric Clinical GuidelinesAndriNo ratings yet
- Febrile Seizures: Status EpilepticusDocument34 pagesFebrile Seizures: Status EpilepticusSAIMA BATOOLNo ratings yet
- PRN Medications: Indications, Uses, Contraindications and Case ExamplesDocument23 pagesPRN Medications: Indications, Uses, Contraindications and Case Examplesdis_is_me100% (1)
- Status EpilepticusDocument4 pagesStatus Epilepticusypk13579No ratings yet
- Talak KejangDocument52 pagesTalak KejangRiga Medina IINo ratings yet
- Pediatric Status Epilepticus Pathway-FINALDocument5 pagesPediatric Status Epilepticus Pathway-FINALvural kesikNo ratings yet
- 2 Types of SeizuresDocument1 page2 Types of SeizuresRatu PalarNo ratings yet
- Status Epilepticus: DR Abdelmoniem SaeedDocument24 pagesStatus Epilepticus: DR Abdelmoniem SaeedYousef Al-AmeenNo ratings yet
- Eclampsia-Icu Management ProtocolDocument3 pagesEclampsia-Icu Management ProtocolmatentenNo ratings yet
- Afebrile SeizuresDocument6 pagesAfebrile SeizuresKristoffer EscletoNo ratings yet
- Seizures: DR Jonny Taitz, FRACP Geschn Paediatrician Sept 2003Document18 pagesSeizures: DR Jonny Taitz, FRACP Geschn Paediatrician Sept 2003alishba100% (2)
- kineme case studyDocument8 pageskineme case studyislafab25No ratings yet
- Medicine RotatationbookletDocument20 pagesMedicine RotatationbookletJanelle JosephsNo ratings yet
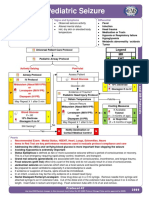
- PediatricseizureDocument2 pagesPediatricseizureRifrita Fransisca HalimNo ratings yet
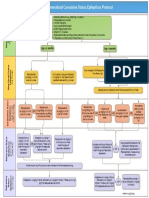
- Guideline For Management of Generalised Convulsive Status Epilepticus in ChildrenDocument11 pagesGuideline For Management of Generalised Convulsive Status Epilepticus in ChildrenAnas Sheikh ibrahimNo ratings yet
- Postpartum Preeclampsia Checklist: SafemotherhoodinitiativeDocument1 pagePostpartum Preeclampsia Checklist: SafemotherhoodinitiativeazimaNo ratings yet
- KEM Protocols - Hypertensive Emergency (Dr. Pritha)Document3 pagesKEM Protocols - Hypertensive Emergency (Dr. Pritha)Sonu AntonyNo ratings yet
- EpinephrineDocument4 pagesEpinephrinegovind_soni_15No ratings yet
- Status Epilepticus Drug Treatment GuideDocument54 pagesStatus Epilepticus Drug Treatment GuideMalik DjamaludinNo ratings yet
- Seven Ps For RSI BOARDDocument2 pagesSeven Ps For RSI BOARDJames BrownNo ratings yet
- Status Elipticus April 2018Document2 pagesStatus Elipticus April 2018walidNo ratings yet
- 7 Hypoglycaemia & ConvulsionsDocument29 pages7 Hypoglycaemia & ConvulsionsJoy KirumbaNo ratings yet
- Febrile SeizureDocument32 pagesFebrile SeizureShiva Valeska ArdhaniswariNo ratings yet
- COVID19 Management Algorithm 22042021 v1Document1 pageCOVID19 Management Algorithm 22042021 v1shivani shindeNo ratings yet
- Status EpilepsiDocument11 pagesStatus EpilepsiNurul aulia AbdullahNo ratings yet
- CHAM Generalized Convulsive Status Epilepticus ProtocolDocument1 pageCHAM Generalized Convulsive Status Epilepticus Protocold'Agung NugrohoNo ratings yet
- Postpartum Preeclampsia Checklist: Emergency Department ExampleDocument1 pagePostpartum Preeclampsia Checklist: Emergency Department ExamplewijeNo ratings yet
- Neonatal SeizuresDocument33 pagesNeonatal SeizuresNursulfia MaharaniNo ratings yet
- Management of convulsions in pregnancy 3Document29 pagesManagement of convulsions in pregnancy 3Monisha ArulalanNo ratings yet
- 038 AnaphylaxisDocument5 pages038 AnaphylaxisabbuahmedibbuNo ratings yet
- Diagnosis and Management of The Epilepsies in Adults and Children: Summary of Updated NICE GuidanceDocument8 pagesDiagnosis and Management of The Epilepsies in Adults and Children: Summary of Updated NICE GuidanceANDREWNo ratings yet
- Risk Factors Recurrence Febrile Seizures ChildrenDocument32 pagesRisk Factors Recurrence Febrile Seizures ChildrenRahul KambleNo ratings yet
- Seizures and Epilepsy After Intracerebral Hemorrhage: An UpdateDocument11 pagesSeizures and Epilepsy After Intracerebral Hemorrhage: An UpdateWilfrido Jose Barrios AgamezNo ratings yet
- Assessment of Febrile Seizures in Children: ReviewDocument12 pagesAssessment of Febrile Seizures in Children: ReviewFerdina NidyasariNo ratings yet
- Status Epilepticus-Patient Management and Pharmocologic TheraphyDocument7 pagesStatus Epilepticus-Patient Management and Pharmocologic Theraphytaner_soysuren100% (1)
- Status Epilepticus PathophysiologyDocument22 pagesStatus Epilepticus PathophysiologySurat TanprawateNo ratings yet
- BJAS - Volume 5 - Issue Issue 1 Part (2) - Pages 275-281Document7 pagesBJAS - Volume 5 - Issue Issue 1 Part (2) - Pages 275-281Vengky UtamiNo ratings yet
- Diagnosis and Management of Nonconvulsive Status Epilepticus (NCSEDocument10 pagesDiagnosis and Management of Nonconvulsive Status Epilepticus (NCSEMasitoh MasitohNo ratings yet
- Anti Epileptic DrugsDocument6 pagesAnti Epileptic DrugsFaria Islam JuhiNo ratings yet
- Critical Care of Neurology 14072022Document103 pagesCritical Care of Neurology 14072022VinaNo ratings yet
- Anaesthesia - 2022 - Migdady - Management of Status Epilepticus A Narrative Review-1Document14 pagesAnaesthesia - 2022 - Migdady - Management of Status Epilepticus A Narrative Review-1Verónica Rojas NavaNo ratings yet
- Febrile Seizures A. Gupta 2016 Continuum (Minneap Minn) 2016 22 (1) 51-59Document9 pagesFebrile Seizures A. Gupta 2016 Continuum (Minneap Minn) 2016 22 (1) 51-59Jose Fernando DiezNo ratings yet
- Understanding Seizures and Epilepsy: Causes, Types, Diagnosis and TreatmentDocument22 pagesUnderstanding Seizures and Epilepsy: Causes, Types, Diagnosis and TreatmentDr venkatesh jalluNo ratings yet
- Eeg NcsDocument5 pagesEeg NcsFathy ShaabanNo ratings yet
- Paleracio Case StudyDocument18 pagesPaleracio Case StudySONY MANDAPNo ratings yet
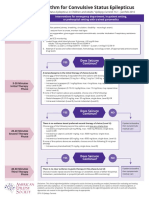
- 2016-TreatmentCSE Algorithm PrintReadyDocument1 page2016-TreatmentCSE Algorithm PrintReadyMauricio Rene Gutierrez CaballeroNo ratings yet
- Status Epilepticus and ICPDocument9 pagesStatus Epilepticus and ICPjoomds51No ratings yet
- Status Triphasicus Vs Status EpilepticusDocument8 pagesStatus Triphasicus Vs Status EpilepticusZaida RojasNo ratings yet
- Status EpilepticusDocument17 pagesStatus EpilepticusXavier AbrilNo ratings yet
- Treatment and Prognosis of Febrile Seizures - UpToDateDocument14 pagesTreatment and Prognosis of Febrile Seizures - UpToDateDinointernosNo ratings yet
- Evaluating A Patient With Seizure Disorders 2Document47 pagesEvaluating A Patient With Seizure Disorders 2Yvonne Sorviel SiiloNo ratings yet
- Understanding the Causes and Classification of SeizuresDocument106 pagesUnderstanding the Causes and Classification of SeizuresLife PediaNo ratings yet
- Status Epilepticus in The ICU: ReviewDocument16 pagesStatus Epilepticus in The ICU: ReviewRotsen Alessandra Tapia VelazcoNo ratings yet