You might also like
- Oxford Textbook of Neurocritical CareDocument750 pagesOxford Textbook of Neurocritical CareMykhailo LysianskyiNo ratings yet
- NCM 107 - Final Exam 2020Document12 pagesNCM 107 - Final Exam 2020Charissa Magistrado De LeonNo ratings yet
- NCM 109 Course Outline For Online LearningDocument7 pagesNCM 109 Course Outline For Online LearningGynesis Lim RoqueroNo ratings yet
- Leopold's Maneuver PDFDocument13 pagesLeopold's Maneuver PDFBiway RegalaNo ratings yet
- RETURN DEMONSTRATION EVALUATION TOOLDocument3 pagesRETURN DEMONSTRATION EVALUATION TOOLsfd33% (3)
- How to Do a Tepid Sponge Bath: A 16-Step GuideDocument2 pagesHow to Do a Tepid Sponge Bath: A 16-Step Guidealexineabidin75% (4)
- Naegele's RuleDocument5 pagesNaegele's RuleSarah Jane MaganteNo ratings yet
- Checklists For Heat and Cold ApplicationDocument6 pagesChecklists For Heat and Cold ApplicationKrisianne Mae Lorenzo Francisco100% (1)
- Checklist of Skills in CHN 1Document5 pagesChecklist of Skills in CHN 1Gi100% (2)
- NGT ProcedureDocument5 pagesNGT ProcedureFrances MercadoNo ratings yet
- Pericare With Heat Lamp TreatmentDocument5 pagesPericare With Heat Lamp Treatmentako at ang exoNo ratings yet
- PTSD - A Short History (PDFDrive)Document257 pagesPTSD - A Short History (PDFDrive)Parisa FadayeeNo ratings yet
- MAALOX (Drug Study)Document3 pagesMAALOX (Drug Study)Kian HerreraNo ratings yet
- Checklist On Internal ExaminationDocument2 pagesChecklist On Internal ExaminationMhel MG100% (1)
- IV Meds in Volumetric Set C RationaleDocument2 pagesIV Meds in Volumetric Set C RationalePascal Marie IzhaqNo ratings yet
- Immediate Newborn Care Definition 23Document6 pagesImmediate Newborn Care Definition 23Courtney Dela FierraNo ratings yet
- Enc Return DemoDocument3 pagesEnc Return DemoJoyce MadarangNo ratings yet
- Nursing Care of Pregnancy ComplicationsDocument3 pagesNursing Care of Pregnancy ComplicationsGynesis Lim Roquero100% (1)
- CHN Bag ContentsDocument1 pageCHN Bag ContentsJulia Shane BarriosNo ratings yet
- Checklist For Newborn: Cavite State UniversityDocument2 pagesChecklist For Newborn: Cavite State UniversityChloe MorningstarNo ratings yet
- NEW CHECKLIST Oropharyngeal SuctioningDocument2 pagesNEW CHECKLIST Oropharyngeal SuctioningDan Dan Manaois100% (1)
- Crisostomo Soapie ChartingDocument2 pagesCrisostomo Soapie ChartingMica OmotsosircNo ratings yet
- Leopold S ManeuverDocument5 pagesLeopold S Maneuverastak ghisingNo ratings yet
- Nutrition (LAB) SAS23Document7 pagesNutrition (LAB) SAS23nicoleangela ubasroselloNo ratings yet
- Medical-Surgical Nursing 1: Pamantasan NG Lungsod NG MaynilaDocument3 pagesMedical-Surgical Nursing 1: Pamantasan NG Lungsod NG MaynilaAye DumpNo ratings yet
- Hot Sitz Bath and Perilite ExposureDocument29 pagesHot Sitz Bath and Perilite ExposureSusan Maglaqui100% (1)
- MCN RLE Sitz Bath Procedure ChecklistDocument3 pagesMCN RLE Sitz Bath Procedure ChecklistHannah Angelu Cabading100% (1)
- Leopolds Maneuver ProcedureDocument3 pagesLeopolds Maneuver ProcedureJoshua ABNo ratings yet
- Expanded Program On Immunization ReportDocument38 pagesExpanded Program On Immunization ReportKimm Delos ReyesNo ratings yet
- Bag Technique 2 UCDocument2 pagesBag Technique 2 UCSoleil Maxwell0% (1)
- Benedict's Test: Detect Glucose in UrineDocument1 pageBenedict's Test: Detect Glucose in UrineSan Dy100% (1)
- Chest Tube Reflective EssayDocument2 pagesChest Tube Reflective EssayAnjae GariandoNo ratings yet
- FCP (Gorres)Document3 pagesFCP (Gorres)Kaloy KamaoNo ratings yet
- Foley Catheterization Insertion and RemovalDocument5 pagesFoley Catheterization Insertion and RemovalArmySapphireNo ratings yet
- Anthropometric MeasurementDocument22 pagesAnthropometric MeasurementJOSLINNo ratings yet
- Finalrationale CAGABCABDocument9 pagesFinalrationale CAGABCABCagabcab Canibel MelanyNo ratings yet
- NCM 109N: Frameworks For Maternal & Child Health NursingDocument37 pagesNCM 109N: Frameworks For Maternal & Child Health NursingZudota100% (1)
- 1 - Excellent 2 - Very Satisfactory Drug Ordered (Ex. Terbutaline Sulfate (Ventolin) Nebule) 3 - Satisfactory 4 - Needs Improvement 5 - PoorDocument1 page1 - Excellent 2 - Very Satisfactory Drug Ordered (Ex. Terbutaline Sulfate (Ventolin) Nebule) 3 - Satisfactory 4 - Needs Improvement 5 - PoorKatriona IntingNo ratings yet
- Oropharyngeal and Nasopharyngeal SuctioningDocument2 pagesOropharyngeal and Nasopharyngeal SuctioningAlana Caballero100% (1)
- Checklist Preparing Medications From Vials and AmpulesDocument4 pagesChecklist Preparing Medications From Vials and AmpulesDenvic0% (1)
- Assisting Normal DeliveryDocument3 pagesAssisting Normal Deliveryrnrmmanphd100% (1)
- Performing Oropharyngeal and Nasopharyngeal SuctioningDocument3 pagesPerforming Oropharyngeal and Nasopharyngeal SuctioningYa Mei LiNo ratings yet
- Prelims Exam - (NCM 107)Document4 pagesPrelims Exam - (NCM 107)conahs nasugbu100% (1)
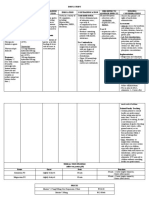
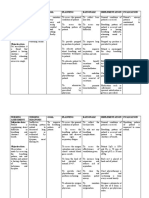
- Nursing Assessment Nursing Diagnosis Goal Planning Rationale Implementation Evaluation Subjective DataDocument5 pagesNursing Assessment Nursing Diagnosis Goal Planning Rationale Implementation Evaluation Subjective DataDimpal Choudhary100% (1)
- TLGDocument1 pageTLGKylie GolindangNo ratings yet
- Pedia AbnormalDocument34 pagesPedia Abnormallight_tyrNo ratings yet
- Perilite Exposure: Therapeutic Effects and Nursing GuidelinesDocument15 pagesPerilite Exposure: Therapeutic Effects and Nursing GuidelinesBella Cy Lopez67% (3)
- Electrocardiogram Return Demonstration ScriptDocument3 pagesElectrocardiogram Return Demonstration ScriptRio Dante100% (1)
- Week 8 - Activity (Case Scenario)Document7 pagesWeek 8 - Activity (Case Scenario)Jollan Marie BuenvenidaNo ratings yet
- Checklist Urinalysis Acetic Benedicts NCM 104Document7 pagesChecklist Urinalysis Acetic Benedicts NCM 104Bethrice MelegritoNo ratings yet
- Wound Dressing ProcedureDocument2 pagesWound Dressing ProcedureCaptainMarksmanNo ratings yet
- I. Mother and Child HealthDocument70 pagesI. Mother and Child Healthconahs nasugbuNo ratings yet
- Delivery Room Nursing Knowledge QuizDocument14 pagesDelivery Room Nursing Knowledge QuizPadilla, John AndrewNo ratings yet
- Clinical Teaching Plan SampleDocument9 pagesClinical Teaching Plan SampleElaine RetesNo ratings yet
- Community Health Nursing Expanded Program On ImmunizationDocument11 pagesCommunity Health Nursing Expanded Program On ImmunizationRaymond EdgeNo ratings yet
- NCM 109 PEDIA PPT 2 High Risk Infant A New Pre TermDocument72 pagesNCM 109 PEDIA PPT 2 High Risk Infant A New Pre TermJoyce EricaNo ratings yet
- Disaster Preparedness - Leadership and Coordination in Disaster in Health Care System With LectureDocument29 pagesDisaster Preparedness - Leadership and Coordination in Disaster in Health Care System With LectureArvie ReyesNo ratings yet
- Kardex: Date/ Time Medications Date Treatment/ ManagementDocument2 pagesKardex: Date/ Time Medications Date Treatment/ ManagementJuviely PremacioNo ratings yet
- I. Framework For Maternal and Child Health Nursing (MCN) Focusing On At-Risk, High Risk, and Sick ClientsDocument5 pagesI. Framework For Maternal and Child Health Nursing (MCN) Focusing On At-Risk, High Risk, and Sick ClientsSophia Loraine Dorone Jesura100% (1)
- Vital Signs Procedure ChecklistDocument10 pagesVital Signs Procedure Checklistako at ang exoNo ratings yet
- NCM 109 LP RLE On HIGH RISK FOR PEDIATRIC CASE 1Document7 pagesNCM 109 LP RLE On HIGH RISK FOR PEDIATRIC CASE 1Melinda Cariño BallonNo ratings yet
- Giving Intradermal Injections ChecklistDocument3 pagesGiving Intradermal Injections ChecklistCamillus Carillo AngelesNo ratings yet
- Day 15 - NCM-109 Children With Alteration in Oxygenation (A)Document50 pagesDay 15 - NCM-109 Children With Alteration in Oxygenation (A)Sheena Patricia ArasulaNo ratings yet
- Pregnancy Induced HypertensionDocument4 pagesPregnancy Induced HypertensionFatmah Sarah CornellNo ratings yet
- The Gut-Kidney Connection inDocument1 pageThe Gut-Kidney Connection inAdrian CraciunNo ratings yet
- 5 - National Clinical Guideline of Dengue Timor Leste - Clean - Final 12 Dec 2022Document93 pages5 - National Clinical Guideline of Dengue Timor Leste - Clean - Final 12 Dec 2022Ahmad FaizNo ratings yet
- Second Degree Av Block Type 1 (Mobitz I or Wenckebach)Document1 pageSecond Degree Av Block Type 1 (Mobitz I or Wenckebach)christine louise bernardoNo ratings yet
- 2000 - GI - Endo InterpretationDocument19 pages2000 - GI - Endo InterpretationambaNo ratings yet
- Murtaghs Patient EducationDocument3 pagesMurtaghs Patient Educationrohancomet100100% (1)
- Outcomes Pre-Int VocabBuilder Unit9Document8 pagesOutcomes Pre-Int VocabBuilder Unit9Eyad SobehNo ratings yet
- Unit - 2nd-WPS Office-1Document8 pagesUnit - 2nd-WPS Office-1Suneel Kumar PrajapatiNo ratings yet
- Neurofibromatosis - Pediatrics - MSD Manual Professional EditionDocument8 pagesNeurofibromatosis - Pediatrics - MSD Manual Professional Editioncynthiadamayanti_drNo ratings yet
- DS & LTsDocument11 pagesDS & LTsLemuel Glenn BautistaNo ratings yet
- Anatomy and Physiology of the Respiratory SystemDocument24 pagesAnatomy and Physiology of the Respiratory SystemRhod Jayson RicaldeNo ratings yet
- Anginal EquivalentDocument20 pagesAnginal Equivalentoki harisandiNo ratings yet
- Uveitis: Classification, Etiologies and Clinical Signs: E-ISSN 2454-2784Document8 pagesUveitis: Classification, Etiologies and Clinical Signs: E-ISSN 2454-2784Lenutza LenutaNo ratings yet
- Enteropathogenic Escherichia Coli Infection in ChildrenDocument10 pagesEnteropathogenic Escherichia Coli Infection in ChildrenAnca MareNo ratings yet
- Genogram: Amanda Yufika, MD, MSC Department of Family Medicine Faculty of Medicine, Syiah Kuala UniversityDocument27 pagesGenogram: Amanda Yufika, MD, MSC Department of Family Medicine Faculty of Medicine, Syiah Kuala UniversityFebbby Mutia SafiraNo ratings yet
- Intoxicación Por VoriconazolDocument2 pagesIntoxicación Por VoriconazolMariana fotos FotosNo ratings yet
- Specific Objevtive Content AV Aids Time Teachin G Learnin G Activit Y Evaluatio NDocument25 pagesSpecific Objevtive Content AV Aids Time Teachin G Learnin G Activit Y Evaluatio NAnanthibalaNo ratings yet
- Heart DiseasesDocument16 pagesHeart DiseasesSanaNo ratings yet
- MICROBIOLOGY & PATHOLOGY NuggetsDocument233 pagesMICROBIOLOGY & PATHOLOGY NuggetsFaraz SayedNo ratings yet
- Chest X-ray, Echo, CBC, Electrolytes for HF DiagnosisDocument2 pagesChest X-ray, Echo, CBC, Electrolytes for HF DiagnosisJeno Luis J. ACUBNo ratings yet
- OphthalmologyDocument12 pagesOphthalmologyAmy StampNo ratings yet
- Cornelia de Lange SyndromeDocument10 pagesCornelia de Lange SyndromeKelvinNo ratings yet
- Common Viral Exanthemas (Measles, Chickenpox & Rubella) : DR Sarika Gupta (MD, PHD), Assistant ProfessorDocument52 pagesCommon Viral Exanthemas (Measles, Chickenpox & Rubella) : DR Sarika Gupta (MD, PHD), Assistant ProfessorashighaNo ratings yet
- 2016 Esc Guidelines For The Diagnosis and Treatment of Acute and 2016Document85 pages2016 Esc Guidelines For The Diagnosis and Treatment of Acute and 2016aslinNo ratings yet
- Muscle Relaxants: Jake A. Nerio BSN 2ADocument19 pagesMuscle Relaxants: Jake A. Nerio BSN 2AMonette Abalos MendovaNo ratings yet
- Doctor's Order Levodopa +carbidopa 250mg/25mg 1 Tab BIDDocument25 pagesDoctor's Order Levodopa +carbidopa 250mg/25mg 1 Tab BIDspain michaelisNo ratings yet
- Understanding Your Sexual SelfDocument15 pagesUnderstanding Your Sexual Selfjohn austin dyNo ratings yet