You might also like
- Parental Overprotection ScaleDocument7 pagesParental Overprotection ScaleMartaria Rizky RinaldiNo ratings yet
- Cvboard - Study Strong PlannerDocument45 pagesCvboard - Study Strong PlannerZaina TNo ratings yet
- Crimson Contagion 2019 Functional Exercise Draft After-Action Report - October 2019Document63 pagesCrimson Contagion 2019 Functional Exercise Draft After-Action Report - October 2019Eric L. VanDussenNo ratings yet
- Spirit Release TherapyDocument12 pagesSpirit Release Therapyravik38100% (6)
- Rogers Infant Start Outcome Paper JADD 2014Document15 pagesRogers Infant Start Outcome Paper JADD 2014MelindaDuciagNo ratings yet
- Journal of Communication Disorders: Rachel Preston, Marie Halpin, Gemma Clarke, Sharon MillardDocument14 pagesJournal of Communication Disorders: Rachel Preston, Marie Halpin, Gemma Clarke, Sharon MillardNUR SYIFAA HAZWANI MOHAMAD SUHAIMINo ratings yet
- Diagnosis and Treatment of Children With Autism Spectrum DisordersFrom EverandDiagnosis and Treatment of Children With Autism Spectrum DisordersRating: 5 out of 5 stars5/5 (1)
- Nursing Care Plan Fluid Volume DeficitDocument2 pagesNursing Care Plan Fluid Volume DeficitXtinego89% (9)
- Evaluation of The Association of Bruxism, Psychosocial and Sociodemographic Factors in PreschoolersDocument8 pagesEvaluation of The Association of Bruxism, Psychosocial and Sociodemographic Factors in PreschoolersChristiana TomescuNo ratings yet
- Prevalence of Sleep Bruxism and Associated Factors in Tanta Preschool ChildrenDocument8 pagesPrevalence of Sleep Bruxism and Associated Factors in Tanta Preschool ChildrenChristiana TomescuNo ratings yet
- A Video-Based Measure To Identify Autism Risk in InfancyDocument7 pagesA Video-Based Measure To Identify Autism Risk in InfancyZachNo ratings yet
- Determinant Factors of Toothache in 8-And 9-Year-Old Schoolchildren, Belo Horizonte, MG, BrazilDocument7 pagesDeterminant Factors of Toothache in 8-And 9-Year-Old Schoolchildren, Belo Horizonte, MG, BrazilRenato KaindoyNo ratings yet
- Escala de AnsiedadDocument7 pagesEscala de AnsiedadMarjourie Picchotito AguilarNo ratings yet
- Periodontal Status of Individuals With Down Syndrome: Sociodemographic, Behavioural and Family Perception in UenceDocument12 pagesPeriodontal Status of Individuals With Down Syndrome: Sociodemographic, Behavioural and Family Perception in UenceRoxana OneaNo ratings yet
- Dental Fear/anxiety Among Children and Adolescents. A Systematic ReviewDocument10 pagesDental Fear/anxiety Among Children and Adolescents. A Systematic ReviewfghdhmdkhNo ratings yet
- Bruxism PediatricDentistryDocument7 pagesBruxism PediatricDentistryNour BsrNo ratings yet
- Negotiating Knowledge - Parents Experience of The NeuropsychiatricDocument11 pagesNegotiating Knowledge - Parents Experience of The NeuropsychiatricKarel GuevaraNo ratings yet
- Original Research Article: ISSN: 2230-9926Document4 pagesOriginal Research Article: ISSN: 2230-9926williamNo ratings yet
- Behavioral Problems and Emotional Stress in Children With BruxismDocument7 pagesBehavioral Problems and Emotional Stress in Children With Bruxismjeremy ludwigNo ratings yet
- Impact of Prolonged Breastfeeding On Dental Caries: A Population-Based Birth Cohort StudyDocument10 pagesImpact of Prolonged Breastfeeding On Dental Caries: A Population-Based Birth Cohort StudySusi susiNo ratings yet
- 8 CC 9Document4 pages8 CC 9dr.aljammalNo ratings yet
- Behavioral Intervention For Sleep ProblemsDocument13 pagesBehavioral Intervention For Sleep ProblemsfernandarwNo ratings yet
- Neonatal Abstinence SyndromeDocument9 pagesNeonatal Abstinence Syndromeapi-376040443No ratings yet
- Clarke2013 PDFDocument7 pagesClarke2013 PDFMartaria Rizky RinaldiNo ratings yet
- HMVJWZX 5 BW SP 7 YZc 7 T7 RDJMDocument7 pagesHMVJWZX 5 BW SP 7 YZc 7 T7 RDJMLili MéndezNo ratings yet
- JIAP October 2021 - Gingival Inflammation in Children and Adolescents With Cerebral Palsy - A Systematic Review and Meta-AnalysisDocument11 pagesJIAP October 2021 - Gingival Inflammation in Children and Adolescents With Cerebral Palsy - A Systematic Review and Meta-AnalysisMutia FauziahNo ratings yet
- 2019 - Changing Conceptualizations of Regression in Autism - OzonoffDocument9 pages2019 - Changing Conceptualizations of Regression in Autism - OzonoffJesus RiveraNo ratings yet
- Non-Nutritive Sucking Habits, Dental Malocclusions, and Facial Morphology in Brazilian Children: A Longitudinal StudyDocument6 pagesNon-Nutritive Sucking Habits, Dental Malocclusions, and Facial Morphology in Brazilian Children: A Longitudinal StudyStacia AnastashaNo ratings yet
- Alshaban Et Al-2019-Journal of Child Psychology and PsychiatryDocument15 pagesAlshaban Et Al-2019-Journal of Child Psychology and PsychiatryZachNo ratings yet
- TTo TSH en Enfoque EscolarDocument15 pagesTTo TSH en Enfoque EscolarCamila AlejandraNo ratings yet
- Infant-Mother Acoustic-Prosodic Alignment and Developmental RiskDocument13 pagesInfant-Mother Acoustic-Prosodic Alignment and Developmental RiskGintarė AmalevičiūtėNo ratings yet
- Evidence Based ProjectDocument69 pagesEvidence Based Projectapi-399918155No ratings yet
- Brief ReportDocument6 pagesBrief Reportsebastoto778No ratings yet
- Sleep Bruxism and Oral Health Related Quality of Life in Children: A Systematic ReviewDocument8 pagesSleep Bruxism and Oral Health Related Quality of Life in Children: A Systematic ReviewAishwarya AntalaNo ratings yet
- Wilson 13 04Document4 pagesWilson 13 04Liz GonzalezNo ratings yet
- Murthy Untreated Caries 2014Document5 pagesMurthy Untreated Caries 2014Kugendran VRNo ratings yet
- Journal of Pediatric Nursing: Pernilla Garmy, Eva K. Clausson, Per Nyberg, Ulf JakobssonDocument5 pagesJournal of Pediatric Nursing: Pernilla Garmy, Eva K. Clausson, Per Nyberg, Ulf JakobssonKristenne Joy TurquezaNo ratings yet
- Sleep Intervention For ASDDocument13 pagesSleep Intervention For ASDmhmd889802uNo ratings yet
- Psychometric Properties of The Screen For Child Anxiety Related Emotional Disorders (SCARED) in Brazilian Children and AdolescentsDocument8 pagesPsychometric Properties of The Screen For Child Anxiety Related Emotional Disorders (SCARED) in Brazilian Children and Adolescentsalfredinho6poqueninoNo ratings yet
- 2020 - Brancher - Social, Emotional, and Behavioral Problemsand Parent-Reported Sleep Bruxism InschoolchildrenDocument7 pages2020 - Brancher - Social, Emotional, and Behavioral Problemsand Parent-Reported Sleep Bruxism InschoolchildrenCarmo AunNo ratings yet
- Etiology Autism Spectrum DisorderDocument11 pagesEtiology Autism Spectrum DisorderfsaajaNo ratings yet
- JCPP 12381Document21 pagesJCPP 12381Javier CáceresNo ratings yet
- Peerj 3825Document30 pagesPeerj 3825Elsa shintia paramitaNo ratings yet
- Factores de Riesgo para Defectos Del Desarrollo Del EsmalteDocument4 pagesFactores de Riesgo para Defectos Del Desarrollo Del Esmaltecrispompittas41No ratings yet
- 1 s2.0 S0165178116302785 MainDocument5 pages1 s2.0 S0165178116302785 MainJohn TelekNo ratings yet
- 2016 FranciaDocument6 pages2016 FranciaRomi Sepúlveda SaldiviaNo ratings yet
- Schultz 2008Document15 pagesSchultz 2008JackNo ratings yet
- 2020 CAEPRecordingINfants Munro+Purdy++Document10 pages2020 CAEPRecordingINfants Munro+Purdy++K JaneNo ratings yet
- Journal Pedsos MadyaDocument9 pagesJournal Pedsos MadyaHajrin PajriNo ratings yet
- 10 White2016Document7 pages10 White2016Francisco CalveraNo ratings yet
- REINO UNIDO Brett2016 Article FactorsAffectingAgeAtASDDiagno PDFDocument11 pagesREINO UNIDO Brett2016 Article FactorsAffectingAgeAtASDDiagno PDFKarel GuevaraNo ratings yet
- Malocclusion in Preschool Children: Prevalence and Determinant FactorsDocument8 pagesMalocclusion in Preschool Children: Prevalence and Determinant FactorsrevinadyaNo ratings yet
- Razafimahefa-Raoelina Et Al. - Self-And Parental Assessment of Quality of Life in Child Cochlear Implant BearersDocument5 pagesRazafimahefa-Raoelina Et Al. - Self-And Parental Assessment of Quality of Life in Child Cochlear Implant BearersPablo VasquezNo ratings yet
- Content ServerDocument9 pagesContent ServerJoni RifaniNo ratings yet
- Adaptation An Validation of The Spanish Version of The Parents Evaluation of Aural-Oral Performance of Children (PEACH) Rating ScaleDocument9 pagesAdaptation An Validation of The Spanish Version of The Parents Evaluation of Aural-Oral Performance of Children (PEACH) Rating ScaleConstanza Vargas GonzálezNo ratings yet
- Observational Tools For Measuring Parent-Infant InteractionDocument34 pagesObservational Tools For Measuring Parent-Infant Interactionqs-30No ratings yet
- Evaluating Pain, Fear, Anxiety or Stress/distress Using Children's Drawings in Paediatric Dentistry: A Scoping ReviewDocument24 pagesEvaluating Pain, Fear, Anxiety or Stress/distress Using Children's Drawings in Paediatric Dentistry: A Scoping ReviewLuciana SanglardNo ratings yet
- Down Syndrome and Feeding ProblemsDocument8 pagesDown Syndrome and Feeding Problemsfelix08121992No ratings yet
- 2019 - JSLHR S 18 0301Document17 pages2019 - JSLHR S 18 0301Andreia TavaresNo ratings yet
- Anxiety Presented by Children Facing Dental TreatmentDocument7 pagesAnxiety Presented by Children Facing Dental TreatmentSudeep M. ChoudharyNo ratings yet
- Baert 2020Document14 pagesBaert 2020Arif Erdem KöroğluNo ratings yet
- Final Edited CF Review Paper Proctor-revised-IIIDocument11 pagesFinal Edited CF Review Paper Proctor-revised-IIISusan Powell-ProctorNo ratings yet
- Phytomedicine: Decandra in The Treatment of Possible Sleep Bruxism in Children: A CrossoverDocument10 pagesPhytomedicine: Decandra in The Treatment of Possible Sleep Bruxism in Children: A CrossoverHary RahmanNo ratings yet
- Behavioural/emotional Problems in Brazilian Children: Findings From Parents ' Reports On The Child Behavior ChecklistDocument10 pagesBehavioural/emotional Problems in Brazilian Children: Findings From Parents ' Reports On The Child Behavior ChecklistElton MatsushimaNo ratings yet
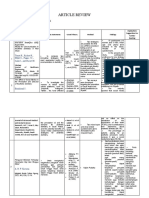
- Article Review - Mona Febiyola Azizah - J2a021043Document3 pagesArticle Review - Mona Febiyola Azizah - J2a021043Mona Febiyola AzizahNo ratings yet
- Article ReviewDocument2 pagesArticle ReviewMona Febiyola AzizahNo ratings yet
- The Effect of Social Media On The Perception and Demand of Aesthetic DentistryDocument5 pagesThe Effect of Social Media On The Perception and Demand of Aesthetic DentistryMona Febiyola AzizahNo ratings yet
- Comparison of Two Innovative Strategies Using AugmentedDocument7 pagesComparison of Two Innovative Strategies Using AugmentedMona Febiyola AzizahNo ratings yet
- Article Review - Mona Febiyola Azizah - J2a021043Document3 pagesArticle Review - Mona Febiyola Azizah - J2a021043Mona Febiyola AzizahNo ratings yet
- 2009 03 10 Organizational CultureDocument39 pages2009 03 10 Organizational CultureClaireNo ratings yet
- Post-Stroke Rehabilitation: Kazan State Medical UniversityDocument11 pagesPost-Stroke Rehabilitation: Kazan State Medical UniversityAigulNo ratings yet
- Coffee-Bean SignDocument1 pageCoffee-Bean Signjudin_oNo ratings yet
- Animal BitesDocument48 pagesAnimal BitesJalouis GabalfinNo ratings yet
- Surgery Clinical Case Presentation - (Thyroid) Riddhi SoniDocument24 pagesSurgery Clinical Case Presentation - (Thyroid) Riddhi SoniKishan S GowdaNo ratings yet
- Sandvikconstruction Dthkatalog LowresDocument44 pagesSandvikconstruction Dthkatalog Lowresroberto funezNo ratings yet
- Constitutionalist: Asa My Concern Is The True Meaning and Application of The ConstitutionDocument15 pagesConstitutionalist: Asa My Concern Is The True Meaning and Application of The ConstitutionGerrit Hendrik Schorel-HlavkaNo ratings yet
- Net Paper II Dec. 2004 NotesDocument10 pagesNet Paper II Dec. 2004 Notesvarunvenu007No ratings yet
- (Ppi) Bsi DiagnosisDocument11 pages(Ppi) Bsi DiagnosisDimas N. SunartoNo ratings yet
- The Effect of Tobacco Smoking Among Third Year Student Nurse in The University of LuzonDocument6 pagesThe Effect of Tobacco Smoking Among Third Year Student Nurse in The University of LuzonNeil Christian TadzNo ratings yet
- IMSEDocument5 pagesIMSEharith r donovanNo ratings yet
- Notes On UtiDocument15 pagesNotes On UtiSaleh Mohammad ShoaibNo ratings yet
- Successful Sample Medicine Personal Statements - July UpdateDocument50 pagesSuccessful Sample Medicine Personal Statements - July UpdateSamiha SaidNo ratings yet
- Algoritma Handling NyeriDocument21 pagesAlgoritma Handling Nyeriscan resepNo ratings yet
- พยาบาลผู้ใหญ่ 60Document14 pagesพยาบาลผู้ใหญ่ 60Rungtip RuangnaparatNo ratings yet
- Metabolic Syndrome Thesis PDFDocument5 pagesMetabolic Syndrome Thesis PDFafknawjof100% (2)
- Anemia Renal - BDF 2018-2Document38 pagesAnemia Renal - BDF 2018-2Buku Tama WaingapuNo ratings yet
- Why Do Adolescents DrinkDocument6 pagesWhy Do Adolescents DrinkchukisaliNo ratings yet
- PDDocument29 pagesPDincredible PragesNo ratings yet
- Annotated Final - Copy-1Document16 pagesAnnotated Final - Copy-1ValarmathiNo ratings yet
- Conrad - 1975 - The Discovery of Hyperkinesis - Society For The Study of Social ProblemsDocument11 pagesConrad - 1975 - The Discovery of Hyperkinesis - Society For The Study of Social ProblemsLais ArendNo ratings yet
- Human Genetics Project - SimonsonDocument24 pagesHuman Genetics Project - SimonsonChris SimonsonNo ratings yet
- Dokumen - Pub Psychiatry Made EasyDocument92 pagesDokumen - Pub Psychiatry Made Easyatq rhmNo ratings yet
- KernicterusDocument6 pagesKernicterusAirin Birthday GiftNo ratings yet
- Mini Lesson Plan & Assessment RubricDocument6 pagesMini Lesson Plan & Assessment RubricAndini PutriNo ratings yet
- Nur 218Document8 pagesNur 218Dan MichNo ratings yet