Volume 7, Issue 6, June – 2022 International Journal of Innovative Science and Research Technology
ISSN No:-2456-2165
Tibial Pilon Fractures Treated by Percutaneous
Screw Fixation with Plaster Cast Immobilization:
Analysis of a Series of 13 Cases
Samir Ben Salah 1,2*, Ayman Ben Abdallah1,2, Adnane Lachkar 1,2, Hicham Yacoubi1,2, Najib Abdeljaouad1,2
1
Orthopedic trauma department, Mohammed VI university hospital, Oujda, Morocco.
2
Faculty of medicine and pharmacy of Oujda, Mohammed first university of Oujda, Morocco
Abstract- Fractures of the tibial pilon remain a result in depression at the point of impact and associated
complicated situation, due to their articular location in lesions (fracture of the external malleolus, the talus, skin
the majority of cases, whose reconstruction in case of lesions...). Fractures of the tibial pilon are among the
fracture of a correct tibioastragalar articular surface therapeutic emergencies that must be managed as soon as
constitutes a great challenge for the surgeon. The thin possible before the aggravation of skin damage that is
and fragile skin covering the distal part of the tibia characterized by the evolutionary even in case of
further complicates the therapeutic strategy for these immobilization of the fracture [2].
fractures, since it is the site of progressive suffering that
may require the open site to be removed. In this sense, II. MATERIALS AND METHODS
the treatment of tibial pilon fractures by closed focus
osteosynthesis (percutaneous screw fixation more or less In this work, we report the experience of the
pinning on demand or external fixation) has an department of traumatology and orthopedics CHU Med VI
important place in the therapeutic management of this of Oujda with a series of patients made of 13 cases having
type of fracture (especially when they are open or been admitted in the department for the management of a
associated with significant skin damage). Closed focus tibial pilon fractures over a period of 7 years spread out
osteosynthesis, regardless of the technique used, allows between the years 2015 and 2021. The treatment of which
was made by percutaneous screwing more or less pinning on
preservation of the skin, but does not allow reduction of
the fracture as is obtained with open focus demand associated with an immobilization by a posterior
osteosynthesis. In this work, we report our experience splint or a plastered boot during 3 to 4 weeks. All patients
with a series of 13 patients with a tibial pilon fracture underwent a complete clinical examination with a standard
treated with percutaneous screw fixation more or less radiograph of the ankle in front and side view and a
pinning on demand associated with plaster cast radiograph of the homolateral knee in front and side view.
immobilization for 3 to 4 weeks. This approach allowed Thus, 70% of the cases benefited from a CT scan of the
us to obtain anatomical reduction of the fracture in 80% ankle with three dimensional reconstruction. For therapeutic
of cases, and satisfactory reduction (contact of more than management, all patients were admitted to the operating
70% on either side of the fracture site as well as room under spinal anesthesia and fluoroscopic control, with
reconstruction of a correct tibiotalar articular surface) reduction of the fracture by external maneuvering (reduction
in 20% of cases. Thus, this approach allowed us to was stabilized by percutaneous screw fixation more or less
obtain consolidation for 12 cases of fractures in an pinning on demand with plaster cast immobilization). A
average of 4 months with a good functional result standard postoperative radiograph of the ankle in front and
(average AOFAS score is 87.2). side view checked the assembly.
Keywords:- Tibial pilon; fracture; percutaneous screw; III. RESULTS
plaster cast immobilisation. For gender, 61.5% of the patients were males and
I. INTRODUCTION 38.5% were females. 100% of the patients were admitted in
the context of a public road accident of which 80% were
Tibial pilon fractures are fractures in which the line is motorcycle accidents and 20% were domestic accidents. In
located in the metaphyseal and epiphyseal region of the our series, 100% of the fractures were closed fractures, for
lower end of the tibia. The degree of comminution of the which the degree of skin damage was assessed by the
fracture site, the involvement of the articular surface and the Tscherne classification (69.2% stage 0, 30.7% stage 1 and
condition of the skin opposite determine the degree of 0% stage 2). For the radiological assessment, all patients had
complexity of management of this type of fracture, as well a standard radiograph of the ankle in front and side view
as the prognosis of these fractures [1]. Fractures of the tibial with front and side view radiograph of the homolateral knee.
pilon are due in the majority of cases to a high energy In our patients, 84.6% of the tibial pilon fractures were
trauma (road accident remains the first etiology in associated with a fracture of the lateral malleolus. The
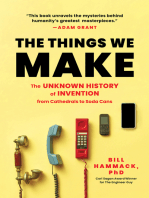
Morocco). The mechanism essentially associates an axial different types of fractures were classified according to the
compression force with accessory forces (dorsal or plantar AO classification (Figure 1,2,3).
hyperflexion, adduction or forced abduction); all of which
IJISRT22JUN1189 www.ijisrt.com 1187
Volume 7, Issue 6, June – 2022 International Journal of Innovative Science and Research Technology
ISSN No:-2456-2165
different types of fractures according to
the AO classification
A2
A3
15%
23% B1
B2
15%
8% B3
C1
8% 8%
C2
8%
15% C3
Fig. 1: different types of fractures according to the AO classification.
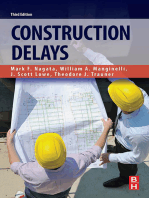
Figure 2 : different types of fractures according to the AO classification.
Fig. 2: Initial radiograph (A, B) of a comminuted fracture involving the epiphyseal region of the tibial pilon with a CT image (C)
in axial section objectifying the degree of epiphyseal comminution.
IJISRT22JUN1189 www.ijisrt.com 1188
Volume 7, Issue 6, June – 2022 International Journal of Innovative Science and Research Technology
ISSN No:-2456-2165
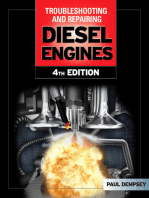
Fig. 3: Initial radiograph of a tibial pilon fracture in frontal (A1) and lateral (A2) views, with postoperative radiographic control in
frontal (B1) and lateral (B2) views.
Fig. 4: Immediate postoperative radiographic control (A1, A2) and after 3 months showing fracture consolidation (B1, B2).
For the therapeutic management of our patients, all cases, we did not obtain a perfect reduction (but we accepted
cases were admitted to the operating room under spinal the set up allowing contact between the edges on either side
anesthesia, and under fluoroscopic control underwent of the fracture site of more than 70%, with reconstruction of
reduction of the fracture by external maneuvering (traction a correct tibioastragalar articular surface), (Figures 3,4,5).
with rotational movements) in an attempt to obtain the Ankle rehabilitation was started immediately
perfect reduction possible. After reduction, the 13 patients postoperatively (without support) in 61.5% of cases, and
received percutaneous screw fixation (associated with after the cast was removed in 38.4%. Early support was
pinning on demand in 38% of cases) followed by allowed after 6 weeks. Thus, in the evolution of our patients,
immobilization with a posterior splint or boot cast for 3 to 4 12 cases had consolidation of the pilon after an average of 4
weeks. When associated, osteosynthesis of the lateral months after the operation (Figures 4,6).
malleolus was performed in all cases (open osteosynthesis
via an external approach to the fibula with placement of a There was only one case of mechanical pseudarthrosis
screw plate in 100% of cases). Osteosynthesis of the (surgical revision performed after 1 year in open surgery
lateral malleolus was always performed first, in order to through an anterointernal approach to the ankle with revival
restore the correct axis and length (it has been observed that of the fracture site, re permeabilization of the centro
reduction of the fibula first improves the reduction of the medullary canal with placement of a corticospongy graft
pilon). In terms of bone, we were able to obtain an from the anterior iliac crest). In terms of septic
anatomical reduction of the fracture site and of the complications, there were no cases of infection, and the
tibioastragalar articular surface in 80% of cases. In 20% of same was true for the skin (no cases of skin necrosis).
IJISRT22JUN1189 www.ijisrt.com 1189
Volume 7, Issue 6, June – 2022 International Journal of Innovative Science and Research Technology
ISSN No:-2456-2165
The functional outcome of our patients was evaluated Lameness.
by the AOFAS score (the American Foot and Ankle Score), Ankle mobility in the sagittal plane.
it is a score based on the analysis of: Mobility of the hind foot (eversion, inversion).
Pain. Forefoot/hindfoot alignment.
The function of the ankle.
The degree of difficulty of walking according to the In our series, we obtained a mean AOFAS score of 87.2
surface (regular surface, stairs, uneven ground...).
IV. DISCUSSION
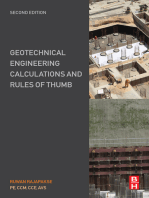
Fig. 5: Initial radiographs with frontal and lateral views (A1,A2) and CT images of the tibial pilon in axial (B3), sagittal (B2) and
three-dimensional (B1) sections, with postoperative radiographic control of the face (C1) and profile (C2).
Fig. 6: Control radiograph after 3 months of surgery in front (A) and side (B) views showing fracture consolidation
IJISRT22JUN1189 www.ijisrt.com 1190
Volume 7, Issue 6, June – 2022 International Journal of Innovative Science and Research Technology
ISSN No:-2456-2165
Despite the progress that has revolutionized trauma African context, we are almost limited by the lack of means
and orthopedic surgery (in terms of diagnostic, therapeutic, (low socioeconomic level), and we do not have a large series
and postoperative physical therapy, which determines the of patients.
outcome of the treatment), tibial pilon fractures remain
among the metaphyseal and epiphyseal fractures that pose V. CONCLUSION
real therapeutic difficulties. This difficulty is linked not only
to the epiphyseal location of this type of fracture, with all In conclusion, the treatment of tibial pilon fractures by
the problems encountered in reconstructing the articular percutaneous screw fixation more or less pinning associated
surface, which in most cases evolves into osteoarthritis, but with plaster cast immobilization for 3 to 4 weeks that we
also to the soft tissue representing the envelope of the distal performed on this series of 13 cases has proven its
leg, which is thin and fragile, and which suffers significantly advantages, firstly on the cutaneous level (since it is done at
in the majority of distal tibia fractures, and which closed focus it preserves the fragile envelope of the distal
determines the therapeutic method, which must never tibia and it can be used whatever the degree of cutaneous
aggravate this suffering [5]. suffering), the same result for the septic complications. This
closed focus did not prevent us from obtaining a perfect
Thus, the degree of fracture comminution and the reduction of the fracture site and the repair of a correct
associated bone lesions (fracture of the lateral malleolus and tibiotalar articular surface, and finally the functional result
the talus) guide the choice of the therapeutic attitude, which obtained (average AOFAS score of 87.2) confirms the
must ensure a normal axis and languor and eliminate all interest of this attitude.
rotation disorders. All these factors involved in the
management of tibial pilon fractures constitute a challenge ACKNOWLEDGMENT
for the surgeon who must ensure a reduction with the most I want to thank all the medical and paramedical staff of
anatomical reconstruction of the tibiotalar articular surface the Mohammed VI University Hospital who helped to
possible without aggravating skin suffering, and for this the complete this work.
surgeon will be obliged to initiate external fixation
whenever possible with or without minimal osteosynthesis REFERENCES
depending on the type of the fracture. Osteosynthesis of the
tibial pilon remains a mission that is not easy from a [1.] Encinas-Ullán CA, Fernandez-Fernandez R, Rubio-
technical point of view for the traumatologist and that Suárez JC, Gil-Garay E. Medial versus lateral plating
depends to a large extent on the experience and habit of the in distal tibial fractures: A prospective study of 40
surgeon who must in all cases put before him all the possible fractures. Rev Esp Cir Ortopédica Traumatol Engl
therapeutic modalities. In this series, we adopted a Ed. 2013 Mar-Apr;57(2):117–22. Epub 2013 Feb 22.
somewhat unusual therapeutic approach (percutaneous [2.] Bastias C, Henríquez H, Pellegrini M, Rammelt S,
screw fixation more or less pinning on request) which Natalio Cuchacovich, Leonardo Lagos, et al. Are
respects the fragile envelope of the ankle, and in fact, we locking plates better than non-locking plates for
won the challenge of not aggravating the skin suffering (0% treating distal tibial fractures? Foot Ankle Surg. 2014
skin necrosis). Thus, in terms of complications, there was Jun;20(2):115–9.
only one case of mechanical pseudarthrosis. In the literature, [3.] Kuo Feng Kao, Peng Ju Huang, Ying Wang Cheng,
there are not many studies on series that have adopted this Lin SY, Ko SH. Postero-medio-anterior approach of
therapeutic approach, especially for type C fractures, where the ankle for the pilon fracture Injury. 2000
percutaneous screw fixation is not widely used. The rate of Mar;31(2):71–4.
pseudarthrosis reported in the published series is variable; [4.] Pugh KJ, Wolinsky PR, Mcandrew MP, Johnson KD.
Bastias [2] did not note any pseudarthrosis when using Tibial pilon fractures: a comparison of treatment
internal osteosynthesis. On the other hand, Pugh [4] methods. J Trauma. 1999 Nov;47(5):937–41.
obtained a significantly higher number of pseudarthrosis in [5.] Plaweski S, Huboud-Peron A, Faure C et Merloz P.
his patients treated with external fixators compared to those Fractures du pilon tibial. Encycl Méd Chir (Elsevier,
treated with internal fixation. In addition, there were no Paris), Appareil locomoteur, 14-087-A-10, 1999, 15 p.
cases of postoperative infection in any of the 13 patients. [6.] Tornetta P, Weiner L, Bergman M. Pilon fractures:
treatment with combined internal and external fixation.
A study of a series of 36 patients with pilon fractures J Orthop Trauma 1993;7:489–96.
treated by combined internal and external fixation revealed a [7.] Salton HL, Rush S, Schuberth J. Tibial plafond
rate of 8% of septic complications [6,7,8,9,10,11,12,13,14], fractures: limited incision reduction with percutaneous
another series of 127 cases of tibial pilon fractures treated fixation. J Foot Ankle Surg 2007;46:261–9
by external fixator with minimal fixation revealed a rate of [8.] Carr JB, Trafton PG. Medial Malleolar and Soft Tissue
0-4% of infectious complications [15,16,17,18,19,20,21,22], Injuries of the Ankle Philadelphia, PA: Saunders; 2003.
and this confirms the advantage of the closed approach, [9.] Sommer C, Chen MS, Espinoza K, Joeris A, Voegtli D
which always gives a lower rate of septic complications than , Stoffel K. The influence of initial cartilage damages
the open approach. The AOFAS score in our series found a in pilon fractures on the development of osteoarthritis
mean of 87.2. These results are consistent with the results and functional outcomes: A prospective multicentre
found in the literature. Encinas, Ullan [1] found a mean case series. J Musculoskelet Surg Res. 2019;3:334-41.
AOFAS score of 84.9 points, Bastias [2] had a mean score
of 89 Kao [3] also obtained a mean score of 87.3. In our
IJISRT22JUN1189 www.ijisrt.com 1191
Volume 7, Issue 6, June – 2022 International Journal of Innovative Science and Research Technology
ISSN No:-2456-2165
[10.] Moreland JR, Bassett LW, Hanker GJ. Radiographic
analysis of the axial alignment of the lower extremity. J
Bone Joint Surg Am. 1987;69:745-9.
[11.] Ruedi TP, Allgower M. The operative treatment of
intra-articular fractures of the lower end of the
tibia. Clin Orthop Relat Res. 1979;138:105-10
[12.] Harper MC, Keller TS. A radiographic evaluation of
the tibiofibular syndesmosis. Foot Ankle. 1989;10:156-
60.
[13.] Sommer C, Nork SE, Graves M, Blauth M, Rudin M, S
toffel K. Quality of fracture reduction assessed by
radiological parameters and its influence on functional
results in patients with pilon fractures a prospective
multicentre study. Injury. 2017;48:2853-63.
[14.] Ramappa M, Bajwa A, Singh A, Mackenney P, Hui A,
Port A. Interobserver and intraobserver variations in
tibial pilon fracture classification systems. Foot.
2010;20:61-3.
[15.] Kreder HJ, Hanel DP, McKee M, Jupiter J, McGillivar
y G, Swiontkowski MF. X-ray film measurements for
healed distal radius fractures. J Hand Surg Am.
1996;21:31-9.
[16.] Paley D, Herzenberg JE, Tetsworth K, McKie J, Bhave
A. Deformity planning for frontal and sagittal plane
corrective osteotomies. Orthop Clin North Am.
1994;25:425-65.
[17.] Tile M, Steele-Scott C, Gollish JD, Begg R. Fractures
of the ankle clinical and biomechanical
considerations. J Bone Joint Surg Am. 1977;59:510.
[18.] Gaudinez RF, Malik AR, Szporn M. Hybrid external
fixation in tibial plafond fractures. Clin Orthop Relat
Res 1996;329:223–32.
[19.] Bacon S, Smith WR, Morgan SJ, Hasenboehler E,
Philips G, Williams A, et al. A retrospective analysis
of comminuted intra-articular fractures of the tibial
plafond: open reduction and internal fixation versus
external Ilizarov fixation. Injury 2008;39:196–202.
[20.] Kapoor SK, Kataria H, Patra SR, Boruah T.
Capsuloligamentotaxis and definitive fixation by an
ankle-spanning Ilizarov fixator in high-energy pilon
fractures. J Bone Joint Surg Br 2010;92:1100–6
[21.] Endres T, Grass R, Biewener A, Barthel S, Zwipp H.
Advantages of minimally invasive reposition,
retention, and Illizarov – hybrid fixation for pilon tibial
fractures with particular emphasis on C2/C3 fractures.
Unfallchirurg 2004;107:273–84
[22.] Kim HS, Jahng JS, Kim SS, Chun CH, Han HJ.
Treatment of tibial pilon fractures using ring fixators
and arthroscopy. Clin Orthop Relat Res 1997;334:
244–50.
IJISRT22JUN1189 www.ijisrt.com 1192
You might also like
- Atlas of Temporomandibular Joint SurgeryFrom EverandAtlas of Temporomandibular Joint SurgeryPeter D. QuinnNo ratings yet
- Long-Term Stability of A Class III Malocclusion With Severe Anterior Open Bite and Bilateral Posterior Crossbite in A Hyperdivergent PatientDocument14 pagesLong-Term Stability of A Class III Malocclusion With Severe Anterior Open Bite and Bilateral Posterior Crossbite in A Hyperdivergent PatientErna NaharuddinNo ratings yet
- Plate Removal Following Orthognathic SurgeryDocument7 pagesPlate Removal Following Orthognathic SurgeryAdam HaytoumiNo ratings yet
- 1 s2.0 S0889540618302683 MainDocument11 pages1 s2.0 S0889540618302683 MainOrtodoncia 1No ratings yet
- Usumi Fujita2018Document15 pagesUsumi Fujita2018Yeimi ArdilaNo ratings yet
- Classification and Treatment of Zygomatic FracturesDocument13 pagesClassification and Treatment of Zygomatic FracturesJeane SuyantoNo ratings yet
- Cao 2020Document5 pagesCao 2020Claudia Ramirez GuevaraNo ratings yet
- Credibility of Three Column Fixation in Schatzker Types V and VI Tibial Plateau FracturesDocument6 pagesCredibility of Three Column Fixation in Schatzker Types V and VI Tibial Plateau FracturesInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- A Case Report of Prosthodontics Treatment of Maxillary DefectDocument4 pagesA Case Report of Prosthodontics Treatment of Maxillary DefectAyu DamayantiNo ratings yet
- Faciomaxillary Fractures in North India A Statistical Analysis and Review of ManagementDocument5 pagesFaciomaxillary Fractures in North India A Statistical Analysis and Review of ManagementKaranPadhaNo ratings yet
- Premaxilla Excess CleftDocument7 pagesPremaxilla Excess CleftDean Faculty of DentistryNo ratings yet
- Admin, Journal Manager, 08-GazzottiDocument9 pagesAdmin, Journal Manager, 08-GazzottistedorasNo ratings yet
- McGonagle2019 Article TibiaPlateauFractureMappingAndDocument6 pagesMcGonagle2019 Article TibiaPlateauFractureMappingAndFarizka Dwinda HNo ratings yet
- New Trends and Techniques in Open Reduction and Internal Fixation of Fractures of The Tibial PlateauDocument8 pagesNew Trends and Techniques in Open Reduction and Internal Fixation of Fractures of The Tibial PlateauCosmina BribanNo ratings yet
- Midfacial Fractures: Our Experience: Le Fratture Medio-Facciali: Nostra EsperienzaDocument9 pagesMidfacial Fractures: Our Experience: Le Fratture Medio-Facciali: Nostra EsperienzaRicky HerdiantoNo ratings yet
- Tibial Plateau Fracture: Anatomy, Diagnosis and Management: Doctors in TrainingDocument9 pagesTibial Plateau Fracture: Anatomy, Diagnosis and Management: Doctors in TrainingChấm TrấmNo ratings yet
- Curettage and Allograft Reconstruction For Giant Cell TumoursDocument5 pagesCurettage and Allograft Reconstruction For Giant Cell TumoursMonem ShakeerNo ratings yet
- The Use of Temporary Anchorage Devices For ORTHODONTIC TREATMENT of Class III Uin A Patient With An Impacred Upper CanineDocument7 pagesThe Use of Temporary Anchorage Devices For ORTHODONTIC TREATMENT of Class III Uin A Patient With An Impacred Upper CanineMargarita Lopez MartinezNo ratings yet
- 1 s2.0 S2352587820300693 MainDocument11 pages1 s2.0 S2352587820300693 Mainabhishekjha0082No ratings yet
- Treating Patella Fractures With A Fixed-Angle Patella PlateDocument7 pagesTreating Patella Fractures With A Fixed-Angle Patella PlateAldrovando JrNo ratings yet
- Functional and Radiological Outcomes of Displaced Mid Shaft Clavicle Fractures Managed Operatively by Precontoured Locking PlateDocument6 pagesFunctional and Radiological Outcomes of Displaced Mid Shaft Clavicle Fractures Managed Operatively by Precontoured Locking PlateIJAR JOURNALNo ratings yet
- Outcomes of Zygomatic Complex Reconstruction With Patient-Specific Titanium Mesh Using Computer-Assisted TechniquesDocument13 pagesOutcomes of Zygomatic Complex Reconstruction With Patient-Specific Titanium Mesh Using Computer-Assisted TechniquesDessy Dwi UtamiNo ratings yet
- Lip Line Changes in Class III Facial Asymmetry Patients After Orthodontic Camouflage Treatment, One-Jaw Surgery, and Two-Jaw Surgery, Lee 2017Document7 pagesLip Line Changes in Class III Facial Asymmetry Patients After Orthodontic Camouflage Treatment, One-Jaw Surgery, and Two-Jaw Surgery, Lee 2017GeromelNo ratings yet
- Trauma Case ReportsDocument6 pagesTrauma Case Reportsarisnicole5No ratings yet
- A Flexion Osteotomy For Correction of A Distal Tibial Recurvatum Deformity - A Retrospective Case SeriesDocument9 pagesA Flexion Osteotomy For Correction of A Distal Tibial Recurvatum Deformity - A Retrospective Case SeriesHamelinYangNo ratings yet
- All Arthroscopic Coracoacromial Ligament TransferDocument9 pagesAll Arthroscopic Coracoacromial Ligament TransferMinh ChíNo ratings yet
- Management of Zygomatic Arch Fractures by Intraoral Open Reduction and Transbuccal FixationDocument3 pagesManagement of Zygomatic Arch Fractures by Intraoral Open Reduction and Transbuccal FixationsevattapillaiNo ratings yet
- Fasciocutaneous Flaps in Reconstruction of Lower Extremity OurDocument7 pagesFasciocutaneous Flaps in Reconstruction of Lower Extremity OurPraganesh VarshneyNo ratings yet
- Current Concepts On Meniscal Repairs, SrimongkolpitakDocument12 pagesCurrent Concepts On Meniscal Repairs, SrimongkolpitakAlhoi lesley davidsonNo ratings yet
- Complications of The Surgical Treatment of Fractures of The Tibial Plateau Prevalence, Causes, and ManagementDocument15 pagesComplications of The Surgical Treatment of Fractures of The Tibial Plateau Prevalence, Causes, and ManagementraynaldidjohariofcNo ratings yet
- Treatment of Tibial Plateau Fractures Dual Plating Dual IncisionDocument6 pagesTreatment of Tibial Plateau Fractures Dual Plating Dual IncisionAnnie JoNo ratings yet
- Osteoarthritis and Osteoporosis 2Document38 pagesOsteoarthritis and Osteoporosis 2tarikeopsNo ratings yet
- Orthodontic Management of A Maxillary Midline Diastema Using Beggs Mechanics Case ReportDocument3 pagesOrthodontic Management of A Maxillary Midline Diastema Using Beggs Mechanics Case ReportEditor IJTSRDNo ratings yet
- Acromioclavicular Fracture Dislocation Fixation TeDocument7 pagesAcromioclavicular Fracture Dislocation Fixation TeMinh ChíNo ratings yet
- Conservative Treatment of Medial Shaft Clavicle Fracture With Borderline Criteria A Case ReportDocument9 pagesConservative Treatment of Medial Shaft Clavicle Fracture With Borderline Criteria A Case ReportAthenaeum Scientific PublishersNo ratings yet
- Fraktur PatellaDocument6 pagesFraktur PatellaPutri AndiraNo ratings yet
- Bicolumnar 90-90 Plating of AO 13C Type Fractures - ScienceDirectDocument16 pagesBicolumnar 90-90 Plating of AO 13C Type Fractures - ScienceDirectNavin ChandarNo ratings yet
- Sectional Denture For Microstomia Patient: A Clinical ReportDocument6 pagesSectional Denture For Microstomia Patient: A Clinical Reportbhuvanesh4668No ratings yet
- AXISDocument8 pagesAXISElianaNo ratings yet
- Eur J Ophthalmol 2020 May 13 Diamint DVDocument5 pagesEur J Ophthalmol 2020 May 13 Diamint DVFernando SousaNo ratings yet
- 2020 Article 265Document7 pages2020 Article 265Fabian BarretoNo ratings yet
- ASimple Techniqueforcorrrectionof Relapsed OverbiteDocument3 pagesASimple Techniqueforcorrrectionof Relapsed OverbiteFabio RibeiroNo ratings yet
- Ortog Com AR - RaffainiDocument7 pagesOrtog Com AR - RaffainiÂngelo Rosso LlantadaNo ratings yet
- C-Arm Assisted Zygoma Fracture Repair: A Critical Analysis of The First 20 CasesDocument8 pagesC-Arm Assisted Zygoma Fracture Repair: A Critical Analysis of The First 20 CasesYeison HidalgoNo ratings yet
- Orthodontic-Surgical Treatment of Class Iii Malocclusion With Mandibular Asymmetry: A Case ReportDocument12 pagesOrthodontic-Surgical Treatment of Class Iii Malocclusion With Mandibular Asymmetry: A Case ReportIJAR JOURNALNo ratings yet
- Titanium Screw Anchorage For Correction of Canted Occlusal Plane in Patients With Facial AsymmetryDocument6 pagesTitanium Screw Anchorage For Correction of Canted Occlusal Plane in Patients With Facial AsymmetryNeeraj AroraNo ratings yet
- Delta Wiring Technique To Treat Bony Mallet Fracture Technique Description and Case SeriesDocument4 pagesDelta Wiring Technique To Treat Bony Mallet Fracture Technique Description and Case SeriesInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Changes in Joint Space Dimension After The Correction of Class II Division 1 MalocclusionDocument7 pagesChanges in Joint Space Dimension After The Correction of Class II Division 1 Malocclusionangiw fuentesNo ratings yet
- Hand Fractures PDFDocument92 pagesHand Fractures PDFfiestaNo ratings yet
- Marcheggianimuccioli 2019Document12 pagesMarcheggianimuccioli 2019Ghusun MadaniNo ratings yet
- Principles and Guidelines in The Management of AnkDocument8 pagesPrinciples and Guidelines in The Management of AnkGeoffrey Muriithi KiogoraNo ratings yet
- Measurement of Tip Apex Distance and Its Relation With Cut-Out After Fixation of Proximal Femoral Fractures With Dynamic Hip Screw or Proximal Femoral Nail a Retrospective Longitudinal Analysis of 106 PatientsDocument4 pagesMeasurement of Tip Apex Distance and Its Relation With Cut-Out After Fixation of Proximal Femoral Fractures With Dynamic Hip Screw or Proximal Femoral Nail a Retrospective Longitudinal Analysis of 106 PatientsInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Treatment of Class I Malocclusion With Mild Crowdi PDFDocument8 pagesTreatment of Class I Malocclusion With Mild Crowdi PDFAristya SidhartaNo ratings yet
- DJMKG 38756 Onay+et+alDocument5 pagesDJMKG 38756 Onay+et+alFebrima Nancy SilabanNo ratings yet
- Dorsal Bridge Plating or Transarticular Screws For Lisfranc Fracture DislocationsDocument7 pagesDorsal Bridge Plating or Transarticular Screws For Lisfranc Fracture DislocationsmaudiaNo ratings yet
- AJODO-2013 Bizetto 144 1 110Document9 pagesAJODO-2013 Bizetto 144 1 110player osamaNo ratings yet
- Injury: David J. Wright, Brent Etiz, John A. ScolaroDocument7 pagesInjury: David J. Wright, Brent Etiz, John A. ScolaroasdasdNo ratings yet
- V-Y Advancement Flap Coverage of Toe-Tip InjuriesDocument4 pagesV-Y Advancement Flap Coverage of Toe-Tip InjuriesreyNo ratings yet
- Treating Patella Fractures With A Locking Patella Plate - First Clinical ResultsDocument5 pagesTreating Patella Fractures With A Locking Patella Plate - First Clinical ResultsLi A VélezNo ratings yet
- Multidetector Coputed Tomographic Evaluation of Maxilofacial TraumaDocument5 pagesMultidetector Coputed Tomographic Evaluation of Maxilofacial TraumaDwi PascawitasariNo ratings yet
- Impact of Stress and Emotional Reactions due to the Covid-19 Pandemic in IndiaDocument6 pagesImpact of Stress and Emotional Reactions due to the Covid-19 Pandemic in IndiaInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- An Overview of Lung CancerDocument6 pagesAn Overview of Lung CancerInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Entrepreneurial Creative Thinking and Venture Performance: Reviewing the Influence of Psychomotor Education on the Profitability of Small and Medium Scale Firms in Port Harcourt MetropolisDocument10 pagesEntrepreneurial Creative Thinking and Venture Performance: Reviewing the Influence of Psychomotor Education on the Profitability of Small and Medium Scale Firms in Port Harcourt MetropolisInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Ambulance Booking SystemDocument7 pagesAmbulance Booking SystemInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Designing Cost-Effective SMS based Irrigation System using GSM ModuleDocument8 pagesDesigning Cost-Effective SMS based Irrigation System using GSM ModuleInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Detection and Counting of Fake Currency & Genuine Currency Using Image ProcessingDocument6 pagesDetection and Counting of Fake Currency & Genuine Currency Using Image ProcessingInternational Journal of Innovative Science and Research Technology100% (9)
- Utilization of Waste Heat Emitted by the KilnDocument2 pagesUtilization of Waste Heat Emitted by the KilnInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Forensic Advantages and Disadvantages of Raman Spectroscopy Methods in Various Banknotes Analysis and The Observed Discordant ResultsDocument12 pagesForensic Advantages and Disadvantages of Raman Spectroscopy Methods in Various Banknotes Analysis and The Observed Discordant ResultsInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Digital Finance-Fintech and it’s Impact on Financial Inclusion in IndiaDocument10 pagesDigital Finance-Fintech and it’s Impact on Financial Inclusion in IndiaInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Computer Vision Gestures Recognition System Using Centralized Cloud ServerDocument9 pagesComputer Vision Gestures Recognition System Using Centralized Cloud ServerInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Study Assessing Viability of Installing 20kw Solar Power For The Electrical & Electronic Engineering Department Rufus Giwa Polytechnic OwoDocument6 pagesStudy Assessing Viability of Installing 20kw Solar Power For The Electrical & Electronic Engineering Department Rufus Giwa Polytechnic OwoInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Predictive Analytics for Motorcycle Theft Detection and RecoveryDocument5 pagesPredictive Analytics for Motorcycle Theft Detection and RecoveryInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Auto Tix: Automated Bus Ticket SolutionDocument5 pagesAuto Tix: Automated Bus Ticket SolutionInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Effect of Solid Waste Management on Socio-Economic Development of Urban Area: A Case of Kicukiro DistrictDocument13 pagesEffect of Solid Waste Management on Socio-Economic Development of Urban Area: A Case of Kicukiro DistrictInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Smart Health Care SystemDocument8 pagesSmart Health Care SystemInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Blockchain Based Decentralized ApplicationDocument7 pagesBlockchain Based Decentralized ApplicationInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Factors Influencing The Use of Improved Maize Seed and Participation in The Seed Demonstration Program by Smallholder Farmers in Kwali Area Council Abuja, NigeriaDocument6 pagesFactors Influencing The Use of Improved Maize Seed and Participation in The Seed Demonstration Program by Smallholder Farmers in Kwali Area Council Abuja, NigeriaInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Cyber Security Awareness and Educational Outcomes of Grade 4 LearnersDocument33 pagesCyber Security Awareness and Educational Outcomes of Grade 4 LearnersInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Visual Water: An Integration of App and Web To Understand Chemical ElementsDocument5 pagesVisual Water: An Integration of App and Web To Understand Chemical ElementsInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Unmasking Phishing Threats Through Cutting-Edge Machine LearningDocument8 pagesUnmasking Phishing Threats Through Cutting-Edge Machine LearningInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Compact and Wearable Ventilator System For Enhanced Patient CareDocument4 pagesCompact and Wearable Ventilator System For Enhanced Patient CareInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- An Industry That Capitalizes Off of Women's Insecurities?Document8 pagesAn Industry That Capitalizes Off of Women's Insecurities?International Journal of Innovative Science and Research TechnologyNo ratings yet
- Implications of Adnexal Invasions in Primary Extramammary Paget's Disease: A Systematic ReviewDocument6 pagesImplications of Adnexal Invasions in Primary Extramammary Paget's Disease: A Systematic ReviewInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Smart Cities: Boosting Economic Growth Through Innovation and EfficiencyDocument19 pagesSmart Cities: Boosting Economic Growth Through Innovation and EfficiencyInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Insights Into Nipah Virus: A Review of Epidemiology, Pathogenesis, and Therapeutic AdvancesDocument8 pagesInsights Into Nipah Virus: A Review of Epidemiology, Pathogenesis, and Therapeutic AdvancesInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Air Quality Index Prediction Using Bi-LSTMDocument8 pagesAir Quality Index Prediction Using Bi-LSTMInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Parastomal Hernia: A Case Report, Repaired by Modified Laparascopic Sugarbaker TechniqueDocument2 pagesParastomal Hernia: A Case Report, Repaired by Modified Laparascopic Sugarbaker TechniqueInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Impact of Silver Nanoparticles Infused in Blood in A Stenosed Artery Under The Effect of Magnetic Field Imp. of Silver Nano. Inf. in Blood in A Sten. Art. Under The Eff. of Mag. FieldDocument6 pagesImpact of Silver Nanoparticles Infused in Blood in A Stenosed Artery Under The Effect of Magnetic Field Imp. of Silver Nano. Inf. in Blood in A Sten. Art. Under The Eff. of Mag. FieldInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Predict The Heart Attack Possibilities Using Machine LearningDocument2 pagesPredict The Heart Attack Possibilities Using Machine LearningInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Parkinson's Detection Using Voice Features and Spiral DrawingsDocument5 pagesParkinson's Detection Using Voice Features and Spiral DrawingsInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Shoulder Pain in Hemiplegia: Statistical Relationship With Five VariablesDocument3 pagesShoulder Pain in Hemiplegia: Statistical Relationship With Five VariablesSahithya MNo ratings yet
- B. Mahmoud - Salmonella - A Dangerous Foodborne Pathogen-Intech (2011)Document450 pagesB. Mahmoud - Salmonella - A Dangerous Foodborne Pathogen-Intech (2011)kiệt lêNo ratings yet
- (PEDIA) 2.04 Pediatric Neurologic Exam - Dr. Rivera PDFDocument15 pages(PEDIA) 2.04 Pediatric Neurologic Exam - Dr. Rivera PDFJudith Dianne IgnacioNo ratings yet
- Influenza Vaccine (Influvac) Consent Form: Title: Name: Age: GenderDocument1 pageInfluenza Vaccine (Influvac) Consent Form: Title: Name: Age: GenderIan BondocNo ratings yet
- WT OetDocument13 pagesWT OetRomana PereiraNo ratings yet
- Nursing Care To Promote Fetal and Maternal HealthDocument4 pagesNursing Care To Promote Fetal and Maternal HealthKristine BartsNo ratings yet
- Clinical Psych BookletDocument36 pagesClinical Psych BookletNancy MohamedNo ratings yet
- Kode Nama Barang Stok Selling Price Disc: KemasanDocument9 pagesKode Nama Barang Stok Selling Price Disc: KemasanEny EndarwatiNo ratings yet
- Tolerance - 2. Regulatory T Cells Why Tolerance Fails: Abul K. Abbas UcsfDocument35 pagesTolerance - 2. Regulatory T Cells Why Tolerance Fails: Abul K. Abbas UcsfMeity ElvinaNo ratings yet
- Bhs InggrisDocument4 pagesBhs InggrisNUR WULAN SARINo ratings yet
- BLS-CPR TRAINING PRESENTATION Rev0Document50 pagesBLS-CPR TRAINING PRESENTATION Rev0aymenmoatazNo ratings yet
- Teaching Learning Guide Topic: Severe Pre-Eclampsia Date: March 11, 2013 FacilitatorsDocument3 pagesTeaching Learning Guide Topic: Severe Pre-Eclampsia Date: March 11, 2013 FacilitatorsJezza Sanchez-Rellita VillariasNo ratings yet
- I. LearningsDocument5 pagesI. LearningsMarie Kelsey Acena MacaraigNo ratings yet
- Essentials of Microbiology 1st Edition PDFDocument648 pagesEssentials of Microbiology 1st Edition PDFJohn Khna100% (1)
- ABO Blood Group System CAIDocument34 pagesABO Blood Group System CAIrupertgrint2000No ratings yet
- Chapter 8. Vaginal and Vulvovaginal DisordersDocument22 pagesChapter 8. Vaginal and Vulvovaginal DisordersMonica CiorneiNo ratings yet
- Admission Nursing AssessmentDocument20 pagesAdmission Nursing Assessmentmonir61No ratings yet
- DEngue FlowchartDocument2 pagesDEngue FlowchartJelly Cruz100% (3)
- Things To Read: A. Trauma: Fractures and DislocationsDocument4 pagesThings To Read: A. Trauma: Fractures and DislocationsHanien YeeNo ratings yet
- Case Study BipolarDocument12 pagesCase Study Bipolarapi-353954238No ratings yet
- Case Study On RDS - NicuDocument32 pagesCase Study On RDS - NicuGandimarei89% (19)
- MalariaDocument4 pagesMalariaAna May Ramas DelgadoNo ratings yet
- Urinary Tract InfectionsDocument44 pagesUrinary Tract Infectionstummalapalli venkateswara rao100% (2)
- This Study Resource Was: Head-To - Toe Assessment Documentation SampleDocument2 pagesThis Study Resource Was: Head-To - Toe Assessment Documentation SampleA Sung100% (3)
- Introduction To NCM 118Document16 pagesIntroduction To NCM 118Frank Jomari MurilloNo ratings yet
- Anti Tuberculosis AgentsDocument15 pagesAnti Tuberculosis Agentsejg26100% (1)
- CV For FellowshipDocument3 pagesCV For Fellowshipapi-568710214No ratings yet
- The Pearson Guide To GPAT and o Umang H Shah SRJ Ilovepdf CompressedDocument5 pagesThe Pearson Guide To GPAT and o Umang H Shah SRJ Ilovepdf CompressedDrSidharth MehanNo ratings yet
- Post-Cardiac Arrest Management in Adults - UpToDateDocument34 pagesPost-Cardiac Arrest Management in Adults - UpToDatehatsune100% (1)
- Manual of Obstetrics, 8e (Jun 25, 2014) - (1451186770) - (LWW) PDFDocument766 pagesManual of Obstetrics, 8e (Jun 25, 2014) - (1451186770) - (LWW) PDFPrem100% (9)
- The Great Bridge: The Epic Story of the Building of the Brooklyn BridgeFrom EverandThe Great Bridge: The Epic Story of the Building of the Brooklyn BridgeRating: 4.5 out of 5 stars4.5/5 (59)
- Crossings: How Road Ecology Is Shaping the Future of Our PlanetFrom EverandCrossings: How Road Ecology Is Shaping the Future of Our PlanetRating: 4.5 out of 5 stars4.5/5 (10)
- The Things We Make: The Unknown History of Invention from Cathedrals to Soda Cans (Father's Day Gift for Science and Engineering Curious Dads)From EverandThe Things We Make: The Unknown History of Invention from Cathedrals to Soda Cans (Father's Day Gift for Science and Engineering Curious Dads)No ratings yet
- Rocks and Minerals of The World: Geology for Kids - Minerology and SedimentologyFrom EverandRocks and Minerals of The World: Geology for Kids - Minerology and SedimentologyRating: 4.5 out of 5 stars4.5/5 (5)
- The Things We Make: The Unknown History of Invention from Cathedrals to Soda CansFrom EverandThe Things We Make: The Unknown History of Invention from Cathedrals to Soda CansRating: 4.5 out of 5 stars4.5/5 (21)
- To Engineer Is Human: The Role of Failure in Successful DesignFrom EverandTo Engineer Is Human: The Role of Failure in Successful DesignRating: 4 out of 5 stars4/5 (138)
- Composite Structures of Steel and Concrete: Beams, Slabs, Columns and Frames for BuildingsFrom EverandComposite Structures of Steel and Concrete: Beams, Slabs, Columns and Frames for BuildingsNo ratings yet
- Troubleshooting and Repair of Diesel EnginesFrom EverandTroubleshooting and Repair of Diesel EnginesRating: 1.5 out of 5 stars1.5/5 (2)
- Finite Element Analysis and Design of Steel and Steel–Concrete Composite BridgesFrom EverandFinite Element Analysis and Design of Steel and Steel–Concrete Composite BridgesNo ratings yet
- Summary of Neil Postman's Amusing Ourselves to DeathFrom EverandSummary of Neil Postman's Amusing Ourselves to DeathRating: 4 out of 5 stars4/5 (2)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Geotechnical Engineering Calculations and Rules of ThumbFrom EverandGeotechnical Engineering Calculations and Rules of ThumbRating: 4 out of 5 stars4/5 (17)
- The Finite Element Method: Linear Static and Dynamic Finite Element AnalysisFrom EverandThe Finite Element Method: Linear Static and Dynamic Finite Element AnalysisRating: 5 out of 5 stars5/5 (3)
- Summary of Taiichi Ohno's Taiichi Ohno's Workplace ManagementFrom EverandSummary of Taiichi Ohno's Taiichi Ohno's Workplace ManagementNo ratings yet
- Structural Cross Sections: Analysis and DesignFrom EverandStructural Cross Sections: Analysis and DesignRating: 4.5 out of 5 stars4.5/5 (19)
- CAREC Road Safety Engineering Manual 3: Roadside Hazard ManagementFrom EverandCAREC Road Safety Engineering Manual 3: Roadside Hazard ManagementNo ratings yet
- Rock Fracture and Blasting: Theory and ApplicationsFrom EverandRock Fracture and Blasting: Theory and ApplicationsRating: 5 out of 5 stars5/5 (2)
- Construction Innovation and Process ImprovementFrom EverandConstruction Innovation and Process ImprovementAkintola AkintoyeNo ratings yet