Professional Documents
Culture Documents
Acr 200303 Relation Between Chest CT Findings and Clinical Conditions of Covid19 Pneumonia A Multicenter Study5293495235082734965
Uploaded by
Michael RamosoOriginal Title
Copyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
Acr 200303 Relation Between Chest CT Findings and Clinical Conditions of Covid19 Pneumonia A Multicenter Study5293495235082734965
Uploaded by
Michael RamosoCopyright:
Available Formats
Cardiopulmonar y Imaging • Original Research
Zhao et al.
Chest CT Findings in COVID-19 Pneumonia
Cardiopulmonary Imaging
Original Research
Relation Between Chest CT
Downloaded from www.ajronline.org by 175.176.24.108 on 03/12/20 from IP address 175.176.24.108. Copyright ARRS. For personal use only; all rights reserved
Findings and Clinical Conditions of
Coronavirus Disease (COVID-19)
Pneumonia: A Multicenter Study
Wei Zhao1 OBJECTIVE. The increasing number of cases of confirmed coronavirus disease
Zheng Zhong2,3 (COVID-19) in China is striking. The purpose of this study was to investigate the relation be-
Xingzhi Xie1 tween chest CT findings and the clinical conditions of COVID-19 pneumonia.
Qizhi Yu2,3 MATERIALS AND METHODS. Data on 101 cases of COVID-19 pneumonia were retro-
Jun Liu1,4 spectively collected from four institutions in Hunan, China. Basic clinical characteristics and de-
tailed imaging features were evaluated and compared between two groups on the basis of clinical
Zhao W, Zhong Z, Xie X, Yu Q, Liu J status: nonemergency (mild or common disease) and emergency (severe or fatal disease).
RESULTS. Patients 21–50 years old accounted for most (70.2%) of the cohort, and five
(5.0%) patients had disease associated with a family outbreak. Most patients (78.2%) had fe-
ver as the onset symptom. Most patients with COVID-19 pneumonia had typical imaging fea-
tures, such as ground-glass opacities (GGO) (87 [86.1%]) or mixed GGO and consolidation
(65 [64.4%]), vascular enlargement in the lesion (72 [71.3%]), and traction bronchiectasis (53
[52.5%]). Lesions present on CT images were more likely to have a peripheral distribution (88
[87.1%]) and bilateral involvement (83 [82.2%]) and be lower lung predominant (55 [54.5%])
and multifocal (55 [54.5%]). Patients in the emergency group were older than those in the non-
emergency group. Architectural distortion, traction bronchiectasis, and CT involvement score
Keywords: coronavirus disease, COVID-19, CT,
pneumonia, SARS-CoV-2 aided in evaluation of the severity and extent of the disease.
CONCLUSION. Patients with confirmed COVID-19 pneumonia have typical imaging
doi.org/10.2214/AJR.20.22976 features that can be helpful in early screening of highly suspected cases and in evaluation
of the severity and extent of disease. Most patients with COVID-19 pneumonia have GGO
W. Zhao and Z. Zhong contributed equally to this study.
or mixed GGO and consolidation and vascular enlargement in the lesion. Lesions are more
Received February 18, 2020; accepted without revision likely to have peripheral distribution and bilateral involvement and be lower lung predomi-
February 19, 2020. nant and multifocal. CT involvement score can help in evaluation of the severity and extent
of the disease.
Supported by Key Emergency Project of Pneumonia
Epidemic of Novel Coronavirus Infection in Hunan
n December 2019, a series of cas- cases were confirmed in Thailand, Japan,
I
Province, National Natural Science Foundation of China
(grant no. 81671671), and the Key R & D projects in Hunan es of pneumonia of unknown South Korea, and the United States [5–8]. On
Province (grant no. 2019SK2131). causation emerged in Wuhan, January 31, 2020, the World Health Organi-
1
Department of Radiology, The Second Xiangya Hospital,
Hubei, China, and quickly raised zation [9] declared the outbreak of coronavi-
Central South University, No. 139 Middle Remin Rd, intense attention around the world [1]. A nov- rus disease (COVID-19) a Public Health
Changsha, Hunan, 410011, P.R. China. Address el bat-origin coronavirus, 2019 novel corona- Emergency of International Concern. Given
correspondence to J. Liu (junliu123@csu.edu.cn). virus, was identified by means of deep se- the striking speed of virus transmission, the
2 quencing analysis [2]. The virus, named ongoing COVID-19 outbreak has undoubted-
Department of Radiology, First Hospital of Changsha,
Hunan, P.R. China. severe acute respiratory syndrome coronavi- ly been linked to panicked memories of two
rus 2 (SARS-CoV-2) [3], is phylogenetically previous betacoronavirus outbreaks in the
3
Changsha Public Health Treatment Center, Hunan, closest to bat SARS-like coronavirus but in a 21st century: SARS-CoV [10, 11] and Middle
P.R. China. separate clade, which means that a novel East respiratory syndrome coronavirus
4
Department of Radiology, Quality Control Center,
coronavirus is spreading [2]. As of February (MERS-CoV) [12, 13].
Changsha, Hunan, P.R. China. 17, 2020, 72,436 laboratory-confirmed cases SARS-CoV-2 proved to have the ability
were consecutively reported in 31 provinces for efficient human-to-human transmission
AJR 2020; 215:1–6 (municipalities and regions) in China, in- [14–16]. The explosion of confirmed cases
ISSN-L 0361–803X/20/2154–1
cluding 11,741 severe cases, 1868 fatal cases, of COVID-19 has been overwhelming, even
and 6242 suspected cases [4]. After the first though the mortality of COVID-19 is low-
© American Roentgen Ray Society reported case in Wuhan, several exported er than that of SARS-CoV and MERS-CoV
AJR:215, October 2020 1
Zhao et al.
infections [17]. A curative vaccine has not formed consent was waived in accordance with cavitation, tree-in-bud, bronchial wall thicken-
yet been developed. Early detection and ef- Council for International Organizations of Medi- ing, reticulation, subpleural bands, traction bron-
ficient control of the route of transmission cal Sciences guidelines. chiectasis, intrathoracic lymph node enlargement,
(i.e., isolation of suspected cases, disinfec- vascular enlargement in the lesion, and pleural ef-
tion) are still the most effective way to fight Patients fusions. We described four distributions: cranio-
the COVID-19 outbreak. The epidemiolog- We retrospectively collected the records of pa- caudal, transverse, lung region, and scattered. A
Downloaded from www.ajronline.org by 175.176.24.108 on 03/12/20 from IP address 175.176.24.108. Copyright ARRS. For personal use only; all rights reserved
ic, laboratory, and clinical features of CO- tients with laboratory-confirmed COVID-19 in the CT score system was used to evaluate the extent of
VID-19 pneumonia have been described [2, database of the Radiology Quality Control Cen- disease. The details of the imaging interpretation
14, 17, 18]. A specific epidemiologic history ter, Hunan. The diagnosis of COVID-19 was deter- were described in our previous study [21].
(e.g., exposure to the Huanan seafood mar- mined with following methods: isolation of SARS-
ket in Wuhan) and a prodrome of fever and CoV-2 or at least two positive results of real-time Statistical Analysis
dry cough are highly indicative of infection RT-PCR assay for SARS-CoV-2 or a genetic se- Continuous variables were presented as medians
with SARS-CoV-2 [18]. However, infections quence matched with SARS-CoV-2. A total of 101 and compared by Mann-Whitney U test. Categoric
by other viruses, such as influenza A and in- patients with consecutively laboratory-confirmed variables were presented as numbers and percent-
fluenza B, can cause the same clinical symp- COVID-19 (45 women, 56 men; mean age, 44.44 ± ages and were compared by chi-square or Fisher
toms as COVID-19, which makes the clinical 12.32 [SD] years; median, 43 years; range, 17–75 exact test between emergency and nonemergency
diagnosis of COVID-19 pneumonia difficult, years) who underwent CT in four cities in Hunan, groups. Two-sided p < 0.05 was considered statis-
especially during flu season. For the large China, were included in this study. The numbers of tically significant. All statistical analyses were per-
number of cases of suspected COVID-19, confirmed cases were as follows: 74 in Changsha, formed with SPSS software (version 24.0, IBM).
laboratory detection is time-consuming and seven in YueYang, 10 in ChangDe, and 10 in Xiang-
may not be available for all people with sus- Tan. All available clinical, laboratory, and epidemi- Results
pected infection owing to the shortage of test ologic data were collected for all patients. Accord- Clinical Characteristics
kits for SARS-CoV-2. These challenges in- ing to the guideline on COVID-19 (trial version 5) Among the 101 included patients, 87 (48
crease the risk of spread by free movement [19] issued by the China National Health Commis- men, 39 women) were in the nonemergency
of people with highly suspected disease. In sion, patients were divided into four groups: those group, and 14 (eight men, six women) were in
addition, the laboratory test can have false- with mild-type, common-type, severe-type, and fa- the emergency group. The age distribution is
negative results. tal-type disease. Because treatment regimens vary shown in Table 1; 70.2% of the patients were
Imaging plays an important role in the by disease type, we regrouped patients into non- 21–50 years old. Seventeen (16.8%) patients
diagnosis and management of COVID-19 emergency (mild and common types) and emer- denied any direct exposure history to Wuhan
pneumonia. CT is considered the first-line gency (severe and fatal types) groups. All patients or to people who had a direct exposure his-
imaging modality in highly suspected cases underwent CT after admission. The mean interval tory to Wuhan (i.e., long-term exposure his-
and is helpful for monitoring imaging chang- between admission and CT examination was 1 day tory to Wuhan, traveling in Wuhan before di-
es during treatment. Therefore, CT has been (range, 0–7 days; median, 1 day). agnosis). Among the 17 patients, 12 had an
identified as an efficient clinical diagnostic exposure history to patients with confirmed
tool for people with suspected COVID-19 Imaging Technique disease, and five denied any direct or indirect
[19]. It has potential for identifying people All patients underwent scanning with the fol-
with negative results of a reverse transcrip- lowing four scanners: Anatom 16HD (Anke Med- TABLE 1: Basic Clinical and Epidemic
tion–polymerase chain reaction (RT-PCR) ical Solutions), HiSpeed-Dual (GE Healthcare), Features
assay but in whom COVID-19 is highly sus- 64-MDCT LightSpeed VCT (GE Healthcare), and
All Patients
pected [20, 21]. COVID-19 pneumonia is Somatom Emotion (Siemens Healthcare). The ac-
Feature (n = 101)
the most common clinical presentation of quisition parameters were set at 120 kVp; 100–
COVID-19. The findings on CT images may 200 mAs; pitch, 0.75–1.5; and collimation, 0.625– Sex
reflect the severity of disease. Previous stud- 5 mm. All imaging data were reconstructed by use Male 56 (55.4)
ies [18, 22–24] have shown imaging features of a medium sharp reconstruction algorithm with Female 45 (44.6)
in small sample sizes. The detailed imaging a slice thickness of 0.625–5 mm. CT images were
Age (y)
features and differences in imaging features acquired at full inspiration with the patient in the
between the four clinical types (mild, com- supine position. Mean 44.44
mon, severe, fatal) [19] have not been well Range 17–75
studied for this disease. Imaging Interpretation Age group (y)
The purpose of this study was to clari- Two radiologists (5 and 15 years of experience)
≤ 20 1 (1.0)
fy the chest CT features in laboratory-con- reviewed chest CT scans blindly and independent-
firmed cases of COVID-19 to further help ly in consensus. All images were viewed with both 21–40 44 (43.6)
clinicians screen for suspected COVID-19 lung (width, 1500 HU; level, −700 HU) and medi- 41–50 27 (26.6)
cases and evaluate the confirmed cases. astinal (width, 350 HU; level, 40 HU) settings. We 51–60 14 (13.9)
evaluated 14 imaging features defined in a previ-
61–70 14 (13.9)
Materials and Methods ous study [25]: ground-glass opacities (GGO),
This study received medical ethical commit- consolidation, mixed GGO and consolidation, ≥ 70 1 (1.0)
tee approval, and the requirement for patient in- centrilobular nodules, architectural distortion, (Table 1 continues on next page)
2 AJR:215, October 2020
Chest CT Findings in COVID-19 Pneumonia
TABLE 1: Basic Clinical and Epidemic
Features (continued)
All Patients
Feature (n = 101)
Epidemiologic history
Downloaded from www.ajronline.org by 175.176.24.108 on 03/12/20 from IP address 175.176.24.108. Copyright ARRS. For personal use only; all rights reserved
Direct exposure 84 (83.2)
Indirect exposure 12 (11.9)
No exposure 5 (4.9)
Onset symptoms
Fever 79 (78.2)
Cough 63 (62.4)
Myalgia or fatigue 17 (16.8) A B
Sore throat 12 (11.9)
Dyspnea 1 (1.0)
Diarrhea 3 (3.0)
Nausea and vomiting 2 (2.0)
More than one symptom 67 (66.3)
None 2 (2.0)
Underlying diseasea
Cardiovascular and 16 (15.8)
cerebrovascular diseases
Surgical history 7 (6.9)
Digestive system disease 6 (5.9)
C D
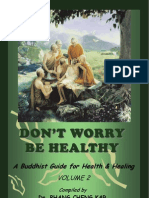
Respiratory system disease 5 (4.9) Fig. 1—37-year-old man with confirmed coronavirus disease (COVID-19), common type. Patient had short-
Endocrine system disease 3 (3.0) term exposure history to Wuhan and onset symptoms of fever (38°C) and cough. CT was performed on day of
admission.
None 71 (70.3) A–D, CT images show bilateral multifocal ground-glass opacities (GGO) and mixed GGO and consolidation
lesions. Traction bronchiectasis (arrowhead, C) and vascular enlargement (arrow, B and D) are also present. CT
Note—Except for age (mean with SD in p arentheses)
involvement score is 5.
data are number with percentage in parentheses.
aSome patients had more than one underlying disease.
(55 [54.5%]). Other evaluated imaging fea- common (78.6%) in the emergency group.
exposure to patients with confirmed disease. tures are shown in Table 2. The mean lung The result was indirectly proved in the ex-
Five (5.0%) patients had disease associated involvement score was 6.39. Cavitation and tent score analysis, which showed that the ex-
with a family outbreak (more than two cases tree-in-bud were not present on the images in tent score was higher in the emergency group
confirmed in one family). Fever was the on- our study. Eight patients had no obvious ab- than in the nonemergency group (p = 0.000).
set symptom for 78.2% of patients. The rates normality on CT images.
of other onset symptoms—cough, myalgia or Discussion
fatigue, sore throat, dyspnea, diarrhea, and Comparison of Basic Clinical Characteristics We comprehensively evaluated and ana-
nausea and vomiting—are shown in Table 1. and CT Findings in Nonemergency and lyzed the radiographic characteristics of 101
Two patients had no onset symptoms. Emergency Groups patients with COVID-19 pneumonia from
Patients in the emergency group were old- the Radiology Quality Control Center, Hu-
CT Findings er than those in the nonemergency group; nan. The basic epidemiologic and clinical
Most patients with COVID-19 had typ- nine (64.3%) patients in the emergency group features were reported. Patients with dis-
ical imaging features, such as GGO (87 were older than 50 years. Regarding under- ease associated with human-to-human trans-
[86.1%]), mixed GGO and consolidation (65 lying disease, no significant difference was mission or a family outbreak need medical
[64.4%]), vascular enlargement in the lesion found between the two groups. Four of the 14 attention. Typical CT findings can help in
(72 [71.3%]), and traction bronchiectasis (53 imaging features—architectural distortion, early screening of patients with suspected
[52.5%]) (Figs. 1 and 2). Several lesion distri- traction bronchiectasis, intrathoracic lymph disease and efficiently evaluate the extent of
bution patterns were identified (Table 2). Le- node enlargement, and pleural effusions— COVID-19 acute respiratory disease.
sions present on CT images of patients with were more likely to be found in the emergen- The increasing frequency of confirmed
COVID-19 were more likely to have a pe- cy group (p < 0.05) (Table 2). The craniocau- COVID-19 cases is striking, and the number
ripheral distribution (88 [87.1%]), have bilat- dal, transverse, and lung region distributions of cases has risen over the number of SARS
eral involvement (83 [82.2%]), be lower lung were not significantly different between the cases [17]. Because the origin and biologic
predominant (55 [54.5%]), and be multifocal two groups, but diffuse lesions were more characteristics of COVID-19 have not been
AJR:215, October 2020 3
Zhao et al.
tients had vascular enlargement of the lesion
(71.3%) that might have been caused by an
acute inflammatory response. However, the
vascular change did not resemble the changes
of malignant lesions, such as lung adenocarci-
noma, which presented distorted or irregular
Downloaded from www.ajronline.org by 175.176.24.108 on 03/12/20 from IP address 175.176.24.108. Copyright ARRS. For personal use only; all rights reserved
vascular dilatation and vascular convergence,
which can be caused by chronic progression
and infiltration of the tumor [27]. Regarding
lesion distribution, patients with COVID-19
A B were more likely to have peripheral distribu-
tion (87.1%), bilateral involvement (82.2%),
lower lung predominance (54.5%), and mul-
tifocal distribution (54.5%), which are consis-
tent with results of previous studies [18].
The differences between the nonemer-
gency and emergency groups regarding ba-
sic clinical and radiographic features were
also analyzed. The patients in the emer-
gency group were older than the patients in
the nonemergency group. However, the rate
of underlying disease was not significantly
C D
different in the two groups, indicating that
Fig. 2—63-year-old woman with confirmed coronavirus disease (COVID-19), severe type. Patient had long-term
other factors (e.g., viral load) may be more
exposure history to Wuhan and onset symptoms of fever and cough. CT was performed 1 day after admission.
A–D, CT images show bilateral diffuse ground-glass opacities and reticulation (arrow, C). CT involvement score of a reflection of the severity and extent of
is 18. COVID-19 pneumonia. Architectural dis-
tortion, traction bronchiectasis, and pleu-
well investigated to date, no medicine can ef- were associated with a family outbreak. These ral effusions, which may reflect the viral
fectively treat the disease, but this is not the results indicate the importance of early iden- load and virulence of COVID-19, were sta-
worst circumstance. The continually increas- tification of patients with disease and separat- tistically different between the two groups
ing number of confirmed and suspected cas- ing the patients without disease from those and may help us to identify the emergency
es is overwhelming medical staff. Laboratory with suspected disease to reduce human- type disease. The performance of intratho-
testing has become the standard for the diag- to-human transmission. racic lymph node enlargement, a rare fea-
nosis of COVID-19 pneumonia, but the sup- CT is considered the routine imaging mo- ture that had a significant difference in our
ply of laboratory kits cannot meet the demand dality for diagnosis and for monitoring the cohort (only one patient), requires further
of the increasing number of suspected cases. care of patients with COVID-19 pneumonia. validation. Moreover, we found that the in-
At the same time, the problem of false-nega- It may help in early detection of lung abnor- cidence of diffuse lesions in the patients in
tive results of the laboratory test has been dis- malities for screening out patients with high- the emergency group was greater than the in-
cussed by clinicians in China. As of February ly suspected disease, especially patients with cidence in the nonemergency group (78.6%
17, 2020, 6242 suspected cases of COVID-19 an initial negative RT-PCR screening result vs 24.1%). Not surprisingly, the extent score
were waiting for final diagnosis [4]. The pa- [21]. In our study, typical imaging features, was also higher in the emergency group than
tients with these suspected cases may indi- such as GGO (86.1%), mixed GGO and con- in the nonemergency group (p = 0.000).
rectly promote virus transmission and cross- solidation (64.4%), and reticulation (48.5%) Two patients had no symptoms or any ab-
infection. In our cohort, 12 (11.9%) patients were present. These results are similar to normal CT findings at onset, and eight pa-
denied any direct exposure history to Wuhan. those of the CT features of other viral infec- tients had no abnormal CT findings. Among
Five (4.9%) patients denied any direct or indi- tions of the lung, such as SARS and MERS the eight patients, three patients had a history
rect exposure history. Five (4.9%) other cases [26, 27]. Interestingly, we found that most pa- of exposure to people with confirmed cases,
TABLE 2: Imaging Findings
Characteristic or Finding All Patients (n = 101) Nonemergency Group (n = 87) Emergency Group (n = 14) p
Age (y) 44.44 (12.3)a 42.94 (11.7)a 53.71 (12.6)a 0.003
Sex 0.890
Male 56 (55.4) 48 (55.2) 8 (57.1)
Female 45 (44.6) 39 (44.8) 6 (42.9)
Underlying disease 30 (29.7) 23 (26.4) 7 (50) 0.073
(Table 2 continues on next page)
4 AJR:215, October 2020
Chest CT Findings in COVID-19 Pneumonia
TABLE 2: Imaging Findings (continued)
Characteristic or Finding All Patients (n = 101) Nonemergency Group (n = 87) Emergency Group (n = 14) p
Imaging finding
Ground-glass opacities 87 (86.1) 73 (83.9) 14 (100) 0.106
Consolidation 44 (43.6) 36 (41.4) 8 (57.1) 0.270
Downloaded from www.ajronline.org by 175.176.24.108 on 03/12/20 from IP address 175.176.24.108. Copyright ARRS. For personal use only; all rights reserved
Mixed ground-glass opacities and consolidation 65 (64.4) 56 (64.4) 9 (64.3) 0.995
Centrilobular nodules 23 (22.8) 20 (23.0) 3 (21.4) 0.897
Architectural distortion 22 (21.8) 16 (18.4) 6 (42.8) 0.040
Bronchial wall thickening 29 (28.7) 22 (25.3) 6 (42.8) 0.173
Reticulation 49 (48.5) 39 (44.8) 9 (64.3) 0.176
Subpleural bands 28 (27.7) 23 (26.4) 4 (28.6) 0.867
Traction bronchiectasis 53 (52.5) 41 (47.1) 12 (85.7) 0.007
Intrathoracic lymph node enlargement 1 (1.0) 0 (0) 1 (7.1) 0.012
Vascular enlargement 72 (71.3) 59 (67.8) 13 (92.9) 0.109
Pleural effusions 14 (13.9) 9 (10.3) 5 (35.7) 0.011
Craniocaudal distribution 0.258
Upper lung predominant 6 (5.9) 6 (6.9) 0 (0)
Lower lung predominant 55 (54.5) 48 (55.2) 7 (50)
No craniocaudal distribution 32 (31.7) 25 (28.7) 7 (50)
Transverse distribution 0.493
Central 1 (1.0) 1 (1.1) 0 (0)
Peripheral 88 (87.1) 74 (85.1) 14 (100)
No transverse distribution 4 (4.0) 4 (4.6) 0 (0)
Lung region distribution 0.172
Unilateral 10 (9.9) 10 (11.5) 0 (0)
Bilateral 83 (82.2) 69 (79.3) 14 (100)
Scattered distribution 0.001
Focal 6 (5.9) 6 (6.9) 0 (0)
Multifocal 55 (54.5) 52 (59.8) 3 (21.4)
Diffuse 32 (31.7) 21 (24.1) 11 (78.6)
Extent of lesion 6.39 (0–20)b 5.34 (3.84)a 12.86 (4.59)a 0.000
No. without CT findings 8 (7.9) 8 (9.2) 0 (0) NA
Note—Except where otherwise indicated, data are number with percentage in parentheses. NA = not applicable.
aMean (SD).
bMean (range).
and five patients had a specific epidemic his- imaging features of patients with negative re- suspected cases and in evaluating the sever-
tory in Wuhan. It once again reminded phy- sults and other virus infections may help us ity and extent of the disease.
sicians of the importance of inquiring about to differentiate COVID-19 pneumonia from
details of epidemic exposure history when other lung infections and then to screen pa- References
seeing patients in an outpatient clinic. There- tients with highly suspected cases. Second, 1. World Health Organization website. Novel coro-
fore, the combination of chest CT and PCR we did not evaluate follow-up CT findings navirus: China. www.who.int/csr/don/12-january-
screening is necessary for early diagnosis. in our study. Exploring the CT changes and 2020-novel-coronavirus-china/en/. Published January
One of the eight patients had abnormal fol- comparing them with the clinical parame- 12, 2020. Accessed January 19, 2020
low-up CT findings that necessitated addi- ters may help us monitor and predict outcome 2. Ren LL, Wang YM, Wu ZQ, et al. Identification of
tional scanning. [28] and support clinical decision making. a novel coronavirus causing severe pneumonia in
The study had several limitations. First, human: a descriptive study. Chin Med J 2020 Feb
only 101 patients with confirmed COVID-19 Conclusion 11 [Epub ahead of print]
were included; negative results and infections Patients with confirmed COVID-19 pneu- 3. World Health Organization website. Naming the
with other viruses were not included in the monia have typical imaging features that coronavirus disease (COVID-2019) and the virus
analyses. Comprehensive investigation of the may be helpful in early screening of highly that causes it. www.who.int/emergencies/diseases/
AJR:215, October 2020 5
Zhao et al.
novel-coronavirus-2019/technical-guidance/nam- SARS Working Group. A novel coronavirus as- satcm.gov.cn/zhengcewenjian/2020-02-06/12847.
ing-the-coronavirus-disease-(covid-2019)-and-the- sociated with severe acute respiratory syndrome. html. Published February 4, 2020. Accessed Febru-
virus-that-causes-it. Accessed February 26, 2020 N Engl J Med 2003; 348:1953–1966 ary 18, 2020
4. China National Health Commission website. Up- 11. Drosten C, Günther S, Preiser W, et al. Identifica- 20. Huang P, Liu T, Huang L, et al. Use of chest CT in
date on the novel coronavirus pneumonia out- tion of a novel coronavirus in patients with severe combination with negative RT-PCR assay for the
break as of 24:00 on February 17. www.nhc.gov. acute respiratory syndrome. N Engl J Med 2003; 2019 novel coronavirus but high clinical suspicion.
Downloaded from www.ajronline.org by 175.176.24.108 on 03/12/20 from IP address 175.176.24.108. Copyright ARRS. For personal use only; all rights reserved
cn/xcs/yqtb/202002/261f72a74be14c4db6e1b5821 348:1967–1976 Radiology 2020 Feb 12 [Epub ahead of print]
33cf4b7.shtml. Published February 17, 2020. Ac- 12. Zaki AM, van Boheemen S, Bestebroer TM, 21. Xie X, Zhong Z, Zhao W, Zheng C, Wang F, Liu J.
cessed February 18, 2020 Osterhaus AD, Fouchier RA. Isolation of a novel Chest CT for typical 2019-nCoV pneumonia: rela-
5. World Health Organization website. Novel corona- coronavirus from a man with pneumonia in Saudi tionship to negative RT-PCR testing. Radiology
virus: Thailand (ex-China). www.who.int/csr/ Arabia. N Engl J Med 2012; 367:1814–1820 2020 Feb 12 [Epub ahead of print]
don/14-january-2020-novel-coronavirus-thailand/ 13. de Groot RJ, Baker SC, Baric RS, et al. Middle East 22. Chung M, Bernheim A, Mei X, et al. CT imaging
en/. Published January 14, 2020. Accessed Febru- respiratory syndrome coronavirus (MERS-CoV): features of 2019 novel coronavirus (2019-nCoV).
ary 18, 2020 announcement of the Coronavirus Study Group. Radiology 2020 Feb 4 [Epub ahead of print]
6. World Health Organization website. Novel corona- J Virol 2013; 87:7790–7792 23. Fang Y, Zhang H, Xu Y, Xie J, Pang P, Ji W. CT
virus: Japan (ex-China). www.who.int/csr/don/16- 14. Chan JF, Yuan S, Kok KH, et al. A familial cluster manifestations of two cases of 2019 novel corona-
january-2020-novel-coronavirus-japan-ex-china/ of pneumonia associated with the 2019 novel virus (2019-nCoV) pneumonia. Radiology 2020
en/. Published January 16, 2020. Accessed Febru- coronavirus indicating person-to-person trans- Feb 7 [Epub ahead of print]
ary 18, 2020 mission: a study of a family cluster. Lancet 2020; 24. Song F, Shi N, Shan F, et al. Emerging coronavirus
7. World Health Organization website. Novel coro- 395:514–523 2019-nCoV pneumonia. Radiology 2020 Feb 6
navirus: Republic of Korea (ex-China). www.who. 15. Phan LT, Nguyen TV, Luong QC, et al. Importa- [Epub ahead of print]
int/csr/don/21-january-2020-novel-coronavirus- tion and human-to-human transmission of a novel 25. Ajlan AM, Ahyad RA, Jamjoom LG, Alharthy A,
republic-of-korea-ex-china/en/. Published January coronavirus in Vietnam. N Engl J Med 2020 Jan Madani TA. Middle East respiratory syndrome
21, 2020. Accessed February 18, 2020 28 [Epub ahead of print] coronavirus (MERS-CoV) infection: chest CT
8. U.S. Centers for Disease Control and Prevention 16. Li Q, Guan X, Wu P, et al. Early transmission dy- findings. AJR 2014; 203:782–787
website. First travel-related case of 2019 novel namics in Wuhan, China, of novel coronavirus- 26. Wong KT, Antonio GE, Hui DS, et al. Thin-sec-
coronavirus detected in United States. www.cdc. infected pneumonia. N Engl J Med 2020 Jan 29 tion CT of severe acute respiratory syndrome:
gov/media/releases/2020/p0121-novel-coronavirus- [Epub ahead of print] evaluation of 73 patients exposed to or with the
travel-case.html. Published January 21, 2020. Ac- 17. Wang C, Horby PW, Hayden FG, Gao GF. A novel disease. Radiology 2003; 228:395–400
cessed February 18, 2020 coronavirus outbreak of global health concern. 27. Gao F, Li M, Ge X, et al. Multi-detector spiral CT
9. World Health Organization website. Statement on Lancet 2020; 395:470–473 study of the relationships between pulmonary
the second meeting of the International Health 18. Huang C, Wang Y, Li X, et al. Clinical features of ground-glass nodules and blood vessels. Eur
Regulations (2005) Emergency Committee re- patients infected with 2019 novel coronavirus in Radiol 2013; 23:3271–3277
garding the outbreak of novel coronavirus (2019- Wuhan, China. Lancet 2020; 395:497–506 28. Pan F, Ye T, Sun P, et al. Time course of lung
nCoV). www.who.int/news-room. Published Janu- 19. China National Health Commission website. Notice changes on chest CT during recovery from 2019
ary 30, 2020. Accessed February 25, 2020 on issuing a new coronavirus infected pneumonia novel coronavirus (COVID-19) pneumonia. Radi-
10. Ksiazek TG, Erdman D, Goldsmith CS, et al.; diagnosis and treatment plan (trial version 5). bgs. ology 2020 Feb 13 [Epub ahead of print]
6 AJR:215, October 2020
You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- ASRS Interpretive Report Parent 2 5 Years SAMPLEDocument9 pagesASRS Interpretive Report Parent 2 5 Years SAMPLERafael MartinsNo ratings yet
- Don't Worry, Be HealthyDocument222 pagesDon't Worry, Be HealthyJocelyn PierceNo ratings yet
- 2pdfnclex ReviewDocument187 pages2pdfnclex ReviewgarvitaNo ratings yet
- Squash ProductionDocument7 pagesSquash ProductionSo Young100% (1)
- Nursing Practice 1Document4 pagesNursing Practice 1marieNo ratings yet
- Disaster Readiness and Risk Reduction: Disasters and Its Effects Learning From Weakness Why Us? Not Others?Document8 pagesDisaster Readiness and Risk Reduction: Disasters and Its Effects Learning From Weakness Why Us? Not Others?Eli67% (12)
- The Vaccine Adverse Event Reporting System (VAERS)Document229 pagesThe Vaccine Adverse Event Reporting System (VAERS)jb_uspu100% (5)
- Intravenous FluidsDocument19 pagesIntravenous Fluidsblack pink in ur area 21100% (1)
- RespiratoryDocument4 pagesRespiratoryDara Krishna Bantugan100% (1)
- Mindoro child with recurrent fever, chills, sweating has malariaDocument16 pagesMindoro child with recurrent fever, chills, sweating has malariaJiezl Abellano Afinidad100% (2)
- Clinical Guideline for Exposed Dental PulpsDocument7 pagesClinical Guideline for Exposed Dental PulpsmahmoudNo ratings yet
- Er MathDocument17 pagesEr MathMichael RamosoNo ratings yet
- Toxicology Emergencies: A Guide to Poison ManagementDocument16 pagesToxicology Emergencies: A Guide to Poison ManagementMichael RamosoNo ratings yet
- Pulmonary Barotrauma Most Common Fatal Blast InjuryDocument11 pagesPulmonary Barotrauma Most Common Fatal Blast InjuryMichael RamosoNo ratings yet
- Jurnal 1Document5 pagesJurnal 1Sarah watiNo ratings yet
- IADT Guidelines 2020 - Fractures and LuxationsDocument17 pagesIADT Guidelines 2020 - Fractures and LuxationsrlahsenmNo ratings yet
- 04 Dejavu or Jamias Vu How The Sars Experience Influenced A Singapore Radiology Departments Response To The Covid 19 Epedemic7324896911872685887Document5 pages04 Dejavu or Jamias Vu How The Sars Experience Influenced A Singapore Radiology Departments Response To The Covid 19 Epedemic7324896911872685887Michael RamosoNo ratings yet
- Jurnal 4Document8 pagesJurnal 4Ahmad Fari Arief LopaNo ratings yet
- Coronavirus Disease 2019 (COVID-19) : Role of Chest CT in Diagnosis and ManagementDocument7 pagesCoronavirus Disease 2019 (COVID-19) : Role of Chest CT in Diagnosis and ManagementOrlin ZlatarskiNo ratings yet
- New COVID-19 entry protocols for FilipinosDocument5 pagesNew COVID-19 entry protocols for FilipinosMichael RamosoNo ratings yet
- COVID-19 entry protocols for foreign nationalsDocument7 pagesCOVID-19 entry protocols for foreign nationalsMichael RamosoNo ratings yet
- 2000 Witnessed Resuscitation by RelativesDocument6 pages2000 Witnessed Resuscitation by RelativesMichael RamosoNo ratings yet
- New Revelations About The Role of STATs in StatureDocument3 pagesNew Revelations About The Role of STATs in StatureMichael RamosoNo ratings yet
- I Atf Resolution 160Document5 pagesI Atf Resolution 160Michael RamosoNo ratings yet
- 1996 Staff Attitudes Towards FPDRDocument7 pages1996 Staff Attitudes Towards FPDRMichael RamosoNo ratings yet
- 1990 CPR Skills Retention in Family Members of Cardiac PatientsDocument6 pages1990 CPR Skills Retention in Family Members of Cardiac PatientsMichael RamosoNo ratings yet
- DV Draft 1Document6 pagesDV Draft 1api-253722866No ratings yet
- Pinhole Defects in Nitrile GlovesDocument1 pagePinhole Defects in Nitrile GlovesDarren TanNo ratings yet
- Cauda Equina SyndromeDocument3 pagesCauda Equina SyndromepuchioNo ratings yet
- Immunology: Benjie M. Clemente, RMT, Mls (Ascpi)Document30 pagesImmunology: Benjie M. Clemente, RMT, Mls (Ascpi)Meriam Juan100% (1)
- BIOCHEMISTRY TEST LOINC CODESDocument15 pagesBIOCHEMISTRY TEST LOINC CODESSowji PNo ratings yet
- Cc2 l5 EndocrinologyDocument4 pagesCc2 l5 EndocrinologyRose Denisse EstrellaNo ratings yet
- The Nervous System: EssentialsDocument27 pagesThe Nervous System: EssentialsSunshine LabraNo ratings yet
- Functions of PlacentaDocument18 pagesFunctions of PlacentaMohammad NabeelNo ratings yet
- Morg Comm Clin Adv 0310Document1 pageMorg Comm Clin Adv 0310Virginia Savely DNPNo ratings yet
- Model Paper 6Document6 pagesModel Paper 6Dr-Sanjay SinghaniaNo ratings yet
- Definitions: The Social Determinants of Health. SummaryDocument4 pagesDefinitions: The Social Determinants of Health. SummaryS VaibhavNo ratings yet
- Catalogue Our Probiotic Strains Probiotical Publ - 06-2020Document46 pagesCatalogue Our Probiotic Strains Probiotical Publ - 06-2020cesar moraisNo ratings yet
- Acitivty Sheets Q1W1 W2Document8 pagesAcitivty Sheets Q1W1 W2Christian BejarinNo ratings yet
- Cancer Immune TherapyDocument452 pagesCancer Immune TherapyatyNo ratings yet
- Drugs and Schizophrenia Review QuizDocument6 pagesDrugs and Schizophrenia Review QuizJames WilkesNo ratings yet
- Establishment of The Stem CellDocument8 pagesEstablishment of The Stem CellCamelia AlexandraNo ratings yet
- Bermuda GrassDocument20 pagesBermuda GrassFurious AssassinNo ratings yet
- Post Operative Pain Management in Elderly Patients: Alketa Dervishi, Kiri ZallariDocument3 pagesPost Operative Pain Management in Elderly Patients: Alketa Dervishi, Kiri ZallarianuradhaNo ratings yet
- What Is The Flu? How Is The Flu Spread?Document2 pagesWhat Is The Flu? How Is The Flu Spread?porfirio ruizNo ratings yet