You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (842)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5806)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Marriage Issues-1Document21 pagesMarriage Issues-1Edward100% (1)
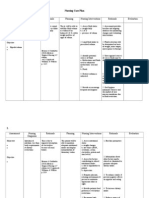
- Nursing Care Plan CKDDocument6 pagesNursing Care Plan CKDReylan Deo Rallo Asio100% (5)
- Synthesis Paper On Nuclear PPDocument3 pagesSynthesis Paper On Nuclear PPchristinekehyengNo ratings yet
- APO SNP Training - GlanceDocument78 pagesAPO SNP Training - GlanceAshwani SharmaNo ratings yet
- CC Assignments CurrentDocument53 pagesCC Assignments Currentranjeet100% (3)
- Bloat: (Ruminal Tympany)Document3 pagesBloat: (Ruminal Tympany)Vishnu PrabhuNo ratings yet
- Clerodendron Inerme An Update of Its Indigenous Uses Phytochemistry and PharmacologyDocument10 pagesClerodendron Inerme An Update of Its Indigenous Uses Phytochemistry and PharmacologyVishnu PrabhuNo ratings yet
- 11.10.21 State Wise Sheep & Goat BreedsDocument1 page11.10.21 State Wise Sheep & Goat BreedsVishnu PrabhuNo ratings yet
- Bioassay Guided Fractionation-An Emerging Technique Influence The Isolation, Identification and Characterization of Lead PhytomoleculesDocument6 pagesBioassay Guided Fractionation-An Emerging Technique Influence The Isolation, Identification and Characterization of Lead PhytomoleculesVishnu PrabhuNo ratings yet
- Original Article A Modified Method For Objective Analysis of Forced Swim Test Using Student PhysiographDocument6 pagesOriginal Article A Modified Method For Objective Analysis of Forced Swim Test Using Student PhysiographVishnu PrabhuNo ratings yet
- Kaalnadai VelanmaiDocument52 pagesKaalnadai VelanmaiVishnu PrabhuNo ratings yet
- Vae 311 Lecture NotesDocument134 pagesVae 311 Lecture NotesVishnu PrabhuNo ratings yet
- ZC-HB09 DatasheetDocument5 pagesZC-HB09 DatasheetManuel Bajista GuitarristaNo ratings yet
- Falkland War - A Brief Overview DraftDocument119 pagesFalkland War - A Brief Overview DraftKanthan JeyaprakashNo ratings yet
- Green Gram CultivationDocument7 pagesGreen Gram CultivationSudhakar JayNo ratings yet
- Assignment On: Course Title: Course Code: Section Submitted byDocument11 pagesAssignment On: Course Title: Course Code: Section Submitted byAl MozahidNo ratings yet
- ENGR 260 - Circuits and Devices: COURSE SYLLABUS - Spring 2015Document4 pagesENGR 260 - Circuits and Devices: COURSE SYLLABUS - Spring 2015saintNo ratings yet
- HUDA Policy Allowing Four BasementsDocument3 pagesHUDA Policy Allowing Four BasementsRahul JindalNo ratings yet
- Weather Proof LouvreDocument6 pagesWeather Proof Louvrentt_121987No ratings yet
- Thermal EngineeringDocument23 pagesThermal Engineeringakeey4uNo ratings yet
- FILE - 20211123 - 141203 - de Thi Mau Tieng AnhDocument17 pagesFILE - 20211123 - 141203 - de Thi Mau Tieng AnhDo Le Quoc LapNo ratings yet
- Epson C82 Service ManualDocument48 pagesEpson C82 Service ManualPablo RothNo ratings yet
- 32LS3400 KoreaDocument60 pages32LS3400 KoreaNightin VargheseNo ratings yet
- F.2 I.S. Vocabulary List (Unit 7-11)Document14 pagesF.2 I.S. Vocabulary List (Unit 7-11)2E (9) HON MARITA JANENo ratings yet
- Korn Walker BlockDocument2 pagesKorn Walker BlockadamsliversNo ratings yet
- Laub Chi-Square Data FittingDocument11 pagesLaub Chi-Square Data Fittingamaresh_rNo ratings yet
- Recombinant DNA MCQDocument6 pagesRecombinant DNA MCQChaze WaldenNo ratings yet
- Paul Quennon HaikusDocument155 pagesPaul Quennon HaikusDiogo MizaelNo ratings yet
- The 8051 Microcontroller and Embedded Systems: Motor Control: Relay, PWM, DC and Stepper MotorsDocument51 pagesThe 8051 Microcontroller and Embedded Systems: Motor Control: Relay, PWM, DC and Stepper MotorsAmAnDeepSingh100% (1)
- Chinese Journal of Chemistry, 31 (1), 15-17 (2013) - DrospirenoneDocument3 pagesChinese Journal of Chemistry, 31 (1), 15-17 (2013) - DrospirenoneSam SonNo ratings yet
- Vol - CXXV-No .184Document44 pagesVol - CXXV-No .184Sonu DeogunNo ratings yet
- Wind PumpDocument6 pagesWind PumpCarlos Castillo PalmaNo ratings yet
- Divisional Chart-IIDocument1 pageDivisional Chart-IIabhisek19870% (1)
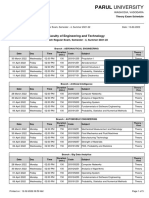
- Parul University: Faculty of Engineering and TechnologyDocument5 pagesParul University: Faculty of Engineering and TechnologySudhanshu SinghNo ratings yet
- (GHS SDS-en) - TAT - SOL-32 - 201901Document5 pages(GHS SDS-en) - TAT - SOL-32 - 201901Ian PrabowoNo ratings yet
- Imagining Persons Robert Duncans Lectures On Charles Olson (Robert Duncan) (Z-Library)Document265 pagesImagining Persons Robert Duncans Lectures On Charles Olson (Robert Duncan) (Z-Library)markNo ratings yet
- CSD 303 Exam 1 Review QuestionsDocument3 pagesCSD 303 Exam 1 Review QuestionsJohn BennettNo ratings yet